
Ankle injuries in athletes: A review of the literature
2021-05-29 01:52:34JenitaJonaJamesOdayAlDadah
World Journal of Meta-Analysis 2021年2期
Jenita Jona James, Oday Al-Dadah
Jenita Jona James, The Medical School, Newcastle University, Newcastle-upon-Tyne NE2 4HH, United Kingdom
Oday Al-Dadah, Translational and Clinical Research Institute, Faculty of Medical Sciences, Newcastle University, Newcastle-upon-Tyne NE2 4HH, United Kingdom
Abstract Ankle injuries are commonplace in the athletic population, with lateral ligament sprains accounting for the majority of them.The medial ligament complex, the distal tibiofibular syndesmosis as well as any of the bones that constitute the ankle joint can also be injured.Typical mechanisms of injury include inversion-plantarflexion and external rotation on a supinated, dorsiflexed or pronated foot.Lesions of the ankle present with similar symptoms of pain, swelling and tenderness.Therefore, a thorough history and physical examination must be obtained to make the correct diagnosis.This is especially critical for athletes as certain injuries can lead to termination of their career if not treated accurately on time.Imaging may be useful in some cases to confirm or rule out differential diagnoses.Most injuries can be managed conservatively using the Protection, Rest, Ice, Compression and Elevation protocol followed by a comprehensive rehabilitation programme.Surgery is reserved for grade III ligament tears that are refractory to initial nonoperative treatment and displaced fractures that are unlikely to unite without surgical intervention.The objective of this review is to discuss the common ankle injuries encountered in the athletic population and the approaches to their diagnosis and management.
Key Words: Ankle sprain; Athlete; Deltoid ligament; Lateral ligament; Syndesmosis; Fracture
INTRODUCTION
The health and social benefits of undertaking exercise are extensive.However, sports are the second highest cause of injuries after home and leisure accidents, and a major cause of pain, loss of mobility, disability and even death[1].The incidence of ankle injuries in the general population is 1 in 10000 per day, but this number increases to 5.23 in athletes, with up to 9.35 ankle injuries per 10000 athletes during competition[2,3].Ankles are the most common site of sports injuries; lateral ligament sprains account for 76.7% of injuries followed by fractures at 16.3%[4,5].High incidences of sprains were seen in team sports such as soccer and rugby, which necessitate quick directional changes whilst running.In contrast, fractures were frequent in high-impact sports like trampolining, parachuting and mountaineering[3,4].Less frequently, syndesmotic injuries, or “high” ankle sprains, which occur above the ankle joint, are reported.These usually occur in sports that are highspeed and high-impact and take place on uneven surfaces, for example, downhill skiing, football and basketball[4,6].
The purpose of this review is to provide an overview of the common ankle injuries occurring in the athletic population and the approaches to assessing and managing them.
ANATOMY
The talocrural, or “true” ankle joint, is articulated by the tibia and fibula of the lower leg and the talus of the foot.It is a synovial hinge joint allowing dorsiflexion and plantarflexion of the foot relative to the lower leg.Stabilising the joint further are the medial and posterior malleoli of the tibia and the lateral malleolus of the fibula.The talocalcaneal, or subtalar joint, is directly below the ankle joint and is composed of the talus and the calcaneus.This joint enables inversion and eversion of the foot[7].
The ligaments of the ankle are divided into the lateral collateral ligaments, the medial (deltoid) collateral ligaments and the syndesmotic ligaments (Figure 1)[7].The lateral ligament consists of three separate ligaments: the anterior talofibular ligament (ATFL), the posterior talofibular ligament (PTFL) and the calcaneofibular ligament (CFL)[2,7].The ATFL and CFL originate from the lateral malleolus and insert into the talar neck and calcaneus, respectively.Whilst the ATFL works to limit pathological inversion and plantar flexion, the CFL restricts over-inversion of the ankle joint[8].The PTFL arises from the malleolar fossa of the lateral malleolus and inserts into the posterior talus.It is under tension when the foot is in dorsiflexion and relaxed when the foot is in plantarflexion or in a neutral position.It is the strongest of the lateral ligaments, and therefore isolated PTFL injuries are rare unless there is complete ankle dislocation.The PTFL does not have an independent role in maintaining ankle stability when the other lateral ligaments are intact.However, if the other ligaments are ruptured, the short and long fibres of the PTFL restrict external rotation of the talus, talar tilt and dorsiflexion, with the short fibres also limiting internal rotation[9].
The deltoid ligament has four parts superficially: tibionavicular, tibiocalcaneal, tibiospring and the posterior tibiotalar ligaments.These cross the ankle and the subtalar joint attaching to the medial malleolus proximally and to the talus, calcaneus and navicular distally.The deep components comprise the anterior tibiotalar ligament and the deep posterior tibiotalar ligament, which only cross the ankle joint.The superficial layers restrict talar abduction and the deep layers prevent external rotation.Both layers work together to limit pronation of the talus[10].The distal tibiofibular syndesmosis binds the tibia and fibula and is held together by four major ligaments: the anterior inferior tibiofibular ligament, the posterior inferior tibiofibular ligament, the transverse tibiofibular ligament and the interosseous ligament.This syndesmosis complex is crucial to maintaining ankle stability and resisting forces that would otherwise separate the tibia and fibula and widen the ankle mortise[6-8,11].This arrangement of ligaments provides static as well as dynamic congruity[12].The movements of the ankle joint have been summarised in Figure 2.

Figure 1 Lateral and medial view of the ankle.
LATERAL LIGAMENT ANKLE SPRAINS
Mechanism of injury
The term ankle sprain is used to describe a range of pathology from an overstretched ligament to complete tearing of the ligaments of the ankle joint[13].In the majority of cases, the mechanism of injury involves inversion of the plantarflexed weight-bearing foot[13,14].Lateral ligaments are most commonly damaged; in 65% of cases, the ATFL alone is injured as it resists inversion and is the weakest of the three lateral ligaments[2,15].Less commonly, both the ATFL and the CFL are affected, whilst injury of the PTFL is rarer and only due to severe ankle joint dislocation[15].
History
A previous lateral ligament sprain is a risk factor for recurring ones and is often reported when a history is undertaken[16].Pain is the major symptom, located laterally over the ATFL area[17].The gold standard for diagnosing lateral ligament injury is delayed physical examination of the ankle joint[13,18].In the hours and days immediately following the injury, pain and tenderness are felt diffusely and haematoma has not developed, so diagnosis is not accurate.However, after 4 to 5 d, the location of pain and tenderness on palpation, plus the characteristic haematoma and swelling can be localised.The specificity and sensitivity at this stage is 84% and 96%, respectively, in deducing the presence or absence of an ATFL injury[18].
Physical examination
Two provocative tests can be performed to assess the stability of the ankle joint, both of which must be compared with the uninjured leg: the anterior drawer test and the talar tilt test[15].These are best done a few days after the injury when the patient can be relaxed and in less pain[17].An anterior drawer test evaluates the integrity of the ATFL.The patient is seated with the knee joint flexed to 90° to relax the calf muscles, and the ankle joint in a 10°-15° plantarflexed position.With the tibia held firmly, the calcaneus is pulled forward.An absent or poor endpoint due to increased anterior talar displacement combined with laxity of the joint indicates a positive test finding.In 50% of cases, a dimple sign can be seen over the area of the ATFL during the manoeuvre.The talar tilt test assesses the integrity of the CFL.The patient is supine, and the ankle is in a neutral position.With the heel braced and both the talus and calcaneus held, the heel is inverted relative to the tibia.A positive test finding is indicated when a firm endpoint cannot be established, and there is increased joint laxity[15,17].
Investigations
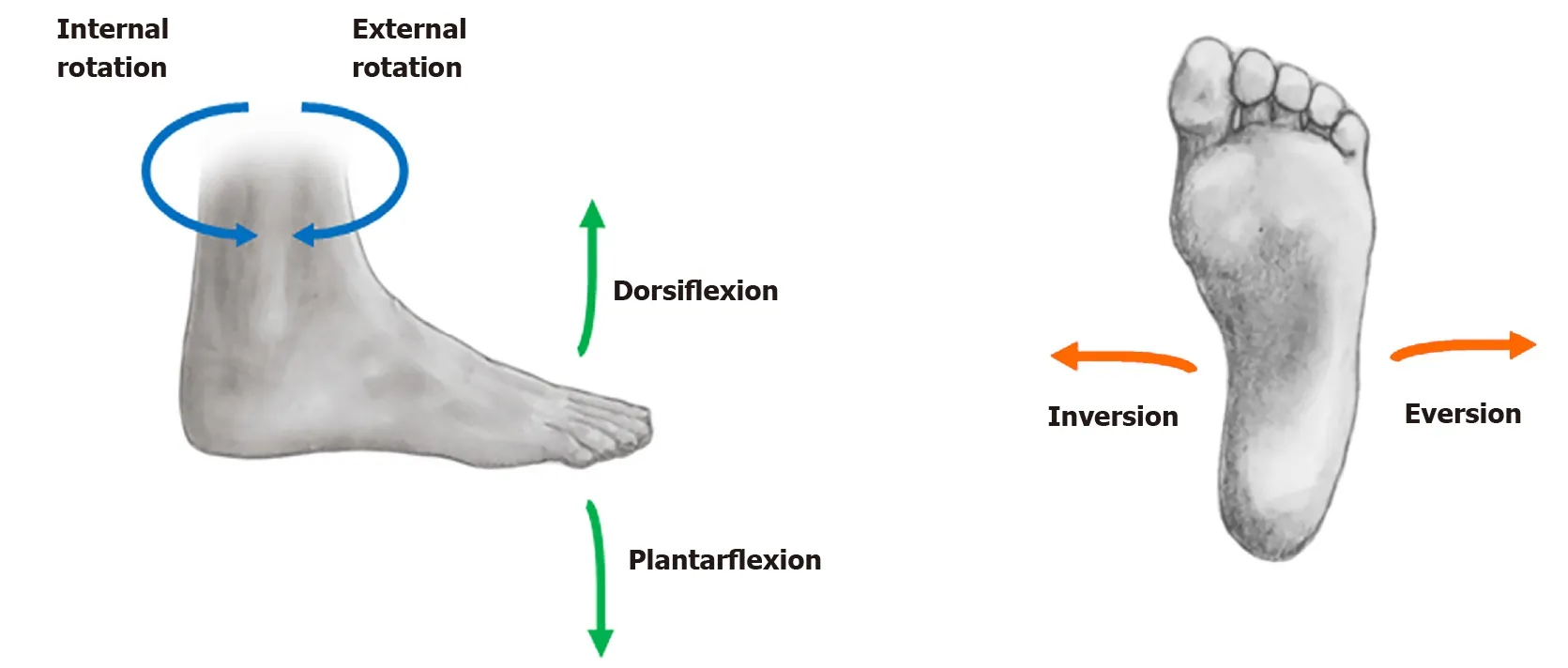
Figure 2 Ankle joint planes of motion (Adapted from CrossFit[45]).
Radiographic analysis is not typically indicated for ankle sprains as a physical examination is deemed sufficient.Magnetic resonance imaging (MRI) if used has 75%-100% sensitivity in diagnosing lateral ligament sprains.However, its high costs combined with the high incidence of ankle sprains render its use uneconomical[15].Occasionally an X-ray is required as determined by the Ottawa Ankle Rules criteria to rule out a fracture[17].
Classification
Ankle sprains ca n be categorised anatomically and functionally according to severity.Grade I injuries are where the ATFL has been stretched and may have microscopic tearing.Mild swelling occurs, and walking is possible with minimal pain.Grade II injuries are caused by a stretched ATFL, and sometimes CFL, where there is partial tearing of the fibres.There is moderate swelling and ecchymosis, and walking is painful.Grade III injuries are the most severe as the ATFL, CFL and PTFL are injured, and the ankle joint is unstable.Severe immediate swelling and ecchymosis is seen, and the intense pain makes it difficult to bear weight[2,17,19].A superior approach to grading ankle sprains divides them into stable and unstable injuries depending on the outcomes of the anterior drawer test and talar tilt test.If both tests are negative, this is a stable grade I injury.A positive anterior drawer test makes it an unstable grade II injury, whereas if both tests are positive, it is classed as an unstable grade III injury.Although this system only accounts for injury to the ATFL and CFL, its reproducibility and ease of use make it ideal for use in the Emergency Department[15].It should be noted that grading is highly subjective with much debate about the classification systems, and differences in inter-rater agreement have been observed[17].Return-toplay (RTP) for grade I injuries is between 1 to 2 wk whilst grade III injuries take 4 to 6 wk longer.
Nonoperative management
The majority of ankle sprains can be managed with conservative treatment.For mildmoderate injuries, protection of the ankle joint with functional support coupled with progressive exercise is thought to be superior to immobilisation[7,18,20].Cast immobilisation may cause muscle stiffness and wasting whilst functional support such as ankle tape and/or tubular elastic bandage allows a quicker RTP and less residual pain[15,21,22].Moreover, semi-rigid support such as an Aircast Air-Stirrup ankle brace (DJO Global Inc., Vista, California, United States) has been shown to provide significant improvement in ankle joint function at 10 d and 30 d compared to elastic support bandage[21].For stable grade I and II injuries, the Protection, Rest, Ice, Compression and Elevation (PRICE) treatment method is recommended to reduce swelling and inflammation alongside functional support and early exercise, which concentrates on increasing range of motion[2,15].Grade II injuries may require additional orthotic support like the Aircast for a longer period of up to 6 wk.Thereafter, a rehabilitation programme including peroneal strengthening and proprioceptive exercises should be followed to enable quicker recovery and RTP[2].Early mobilisation allows healing by stimulating the collagen bundle orientation[7].As grade III injuries are unstable, immobilisation for up to 1 mo is advised alongside strengthening exercises.Generally, in the acute phase, the use of nonsteroidal antiinflammatory drugs (NSAIDs) leads to a significant reduction in pain[23].However, one study reported that the swift return to activities that NSAIDs provide might impair the healing process, as trial participants who were given piroxicam had greater swelling and instability 14 d post-injury[20].Evaluation of the effects of therapeutic ultrasound in the treatment of acute ankle sprains shows limited evidence[24].
Surgical intervention
Whilst most patients heal successfully, those with persistent symptoms past 3 mo despite nonoperative management should be evaluated for chronic lateral ankle instability.This is primarily managed with physical therapy and bracing.However, surgery is indicated in those who show no improvement after 3-6 mo[2,7,15,25].Surgery is typically performed as an outpatient procedure under general anaesthesia with a popliteal nerve block.The surgical procedures are classed as anatomical or nonanatomical reconstruction.Anatomical reconstruction includes the Broström and modified Broström procedures whereby the ATFL and CFL are shortened and reinserted.These are excellent in restoring ankle stability and provide longevity.Nonanatomical reconstruction involves tendon transfers, such as the Watson-Jones, Evans and Chrisman Snook procedures.These surgical techniques have the potential postoperative risks and complications of functional instability and early arthritis and can also limit range of motion[2,25].
MEDIAL LIGAMENT ANKLE SPRAINS
Mechanism of injury
Sprains of the medial ligament of the ankle joint are uncommon and are typically found to be in conjunction with fibular fractures and sprains of the tibiofibular syndesmosis[15,17].Only around 4% of all ankle ligament injuries are due to injury to the deltoid ligament[26].The usual mechanism of injury tends to be a pronationexternal rotation position of the foot, though pronation-abduction and supinationexternal rotation positions are also observed[10,17].These injuries tend to occur in sports such as basketball, dancing and long jump[26].
History
Pain, tenderness and swelling are present on the medial side of the ankle, and ecchymosis may present a few days later.Weightbearing will be difficult on the affected foot and may be associated with a feeling of instability.Some patients also report a popping sensation or a feeling of the foot ‘giving way’ especially when walking downhill[5,10,17].
Physical examination
When examining the affected ankle, it is important to check for signs of fractures and syndesmotic sprains as these commonly present alongside deltoid ligament injuries.If the ligament is ruptured completely, this may be palpated beneath the medial malleolus.During the external rotation stress test, deltoid ligament damage is indicated if the talus moves away from the medial malleolus[10,17,27,28].
Investigations
Standard weight-bearing radiographs in the anteroposterior (AP), lateral and mortise views may provide further clues to aid diagnosis.A width of 4 mm or higher of the medial clear space between the talus and medial malleolus indicates disruption of the deltoid ligament and syndesmosis.Isolated deltoid injuries do not cause widening of the medial clear space as the lateral malleolus will hold the talus in place[5,10,17].
Classification
Deltoid ligament sprains are categorised by the extent of involvement of the ligament.Type I lesions are a proximal tear, type II lesions involve the intermediate component, and type III lesions are distal injuries of the deltoid ligament[10,26,29].
Nonoperative management
Similar to lateral ligament sprains, the PRICE protocol is the recommended method of management for medial ligament ankle sprains.Immobilisation in a cast with additional support from bracing or taping further facilitates recovery.Following this, a rehabilitation programme focussing on building strength and improving coordination and proprioception is advised.Return to training at light intensity can be expected in 6-8 wk[10,27].
Surgical intervention
Surgery is not routinely indicated for isolated deltoid ligament injuries[27].
SYNDESMOTIC ANKLE SPRAINS
Mechanism of injury
Unlike lateral ankle sprains, syndesmotic ankle sprains are thought to be caused due to external rotational forces acting on a dorsiflexed foot.The exact mechanism cannot be determined as the movement occurs too quickly to be sufficiently recognised.In this position, the ligaments typically injured are the anterior inferior tibiofibular ligament and the interosseous ligament depending on the everted or neutral position of the foot, respectively[6,7,11,20].Isolated syndesmotic ankle sprains are relatively unusual, as they are usually associated with fibular fractures and/or deltoid ligament sprains.Syndesmotic injuries can lead to functional limitations and chronic pain, so prompt diagnosis and treatment are crucial[11,30].
History
Pain is the principal complaint, localised to the anterior inferior tibiofibular ligament and often exacerbated by active and passive external rotation and/or dorsiflexion of the foot.Upon palpation, the ankle is tender in this area.Pain may also be felt proximally due to damage to the interosseous membrane or more serious injury.Swelling is significantly less than that for lateral ligament sprains.However, poor/absent weight-bearing and/or plantar flexion is seen[11,15,17].
Physical examination
Three tests can be undertaken to determine injury to the syndesmosis: the squeeze, crossed-leg and external rotation stress test (Kleiger’s test).In the squeeze test, the foot is dorsiflexed, and the midshaft of the tibia and fibula are squeezed together.For the crossed-leg test, the patient rests the distal third of the fibula of the affected leg on the knee of the opposite leg.A gentle downward compressive force is then applied to the knee of the injured leg.To perform the external rotation test, the patient is seated.The tibia is then stabilised as the foot is dorsiflexed and rotated externally relative to the tibia.During all three manoeuvres, pain over the syndesmotic area indicates a positive sign[15,17,30].
Investigations
As syndesmotic injuries are so rare, the above tests have only been validated in a small group of patients.Their sensitivity and specificity cannot be reliably determined.Therefore, imaging is recommended in this scenario[15].Standard ankle weightbearing radiographs in the AP, mortise and lateral views should be performed to rule out fractures and determine syndesmosis widening[31].If syndesmosis widening is seen or there is proximal fibular tenderness, then full length radiographs of the tibia and fibula in the AP and lateral views are required to exclude a Maisonneuve fracture.There is no consensus on the guidelines indicating syndesmosis diastasis.However, a joint space widening of greater than 5 mm or tibiofibular overlap of less than 10 mm on AP view is frequently used.Stress radiographs in the lateral view with the foot externally rotated in both dorsiflexion and plantarflexion may also show the diastasis and any posterolateral displacement of the fibula[11,17].MRI is highly sensitive (100%), specific (93%) and accurate (96%) in determining the extent of syndesmotic injury[6,15,30].A high-intensity signal resembling the Greek letter lambda (λ) is seen on a coronal MRI, known as the ‘lambda sign’.Although not a diagnostic indicator in itself, in combination with positive physical examination findings, the lambda sign can help clinicians determine which patients require surgical intervention[32].MRI can also demonstrate secondary findings such as a bone bruise, osteochondral lesions and anterior talofibular ligament injury, all of which are associated with poorer response to rehabilitation and longer recovery periods.Arthroscopy shows promise for its use as a diagnostic tool; one study has found it to be 100% accurate in identifying syndesmotic injury[11].
Classification
The classification system for syndesmotic ankle sprains grades injuries from I to III by severity, similar to lateral ligament sprains.Athletes should be informed that recovery times for syndesmotic ankle sprains are up to two times longer than that for lateral ligament sprains, especially if managed conservatively[6,8].One study found that the time to RTP and/or functional disability was directly correlated to the degree of tenderness of the interosseous membrane[33].
Nonoperative management
Conservative treatment is the standard management for athletes who have a sprain without diastasis.Initially, PRICE is recommended to reduce pain and associated symptoms.Whilst lateral ligament sprains benefit from early mobilisation, syndesmotic injuries are more severe and therefore require nonweight-bearing immobilisation and stability such as bracing, walking boots and casting during the acute phase.This allows healing, protects the syndesmosis from further injury and prevents further rotation of the talus and fibula.As the pain subsides, protected weight-bearing training can begin using crutches.Light balance training on a balance pad and low-level strength training using Theraband (The Hygienic Corp., Akron, Ohio, United States) can commence.Exercises such as seated heel raises can also help with strengthening.As the patient recovers, functional exercises such as double to single heel raises and hops are added to the rehabilitation program.The final stage involves progression from walking fast to jogging, running and sport-specific training.Ankle braces and/or taping must be used for stability when returning to play[6,11,20,30,31].
Surgical intervention
Surgery is indicated for patients who have diastasis of the syndesmosis with or without concurrent fibular fracture and for those with lower grade injuries that are refractory to conservative treatment.The syndesmosis has to be reduced initially, and this can be done open, closed or arthroscopically and checked with fluoroscopy.Two surgical methods are commonly used.In syndesmotic screw fixation, screws are placed in position to hold the syndesmosis in place until healing can occur.The postoperative plan includes being nonweight-bearing for 6-8 wk, and the functional outcomes are excellent if the syndesmosis is reduced adequately.There is no significant difference between routinely retaining or removing syndesmotic screws as both groups of patients have similar clinical outcomes, and such a removal is not necessarily routinely recommended.If screw breakage occurs in situ over time, they may be removed in symptomatic patients after 8 to 12 wk from the original surgical procedure.However, for the vast majority of patients, breakage of the screws will have little clinical consequence[34].
Generally, one or two cortical screws are inserted above the ankle joint going through three or four bone cortices in an anteromedial direction (fibula to tibia) to avoid malreduction.At present, there is no consensus in terms of number of screws used or cortices purchased, screw diameter size or the exact location of the fixation.It also depends on patient variables such as a history of osteoporosis and smoking and degree of syndesmotic instability.Two screws are usually preferred as they offer greater resistance.The screw type can be cortical, which is fully threaded, or cancellous, which is fully or partially threaded.Cortical screws are used for positioning such as with plate fixation whilst cancellous screws are useful as lag screws, exerting a compressive force.There is no strong evidence to support placement through threevsfour cortices[6,31,34,35].The Syndesmosis TightRope XP implant fixation system (Arthrex Inc., Naples, Florida, United States) uses a strong suture loop that is tensioned between two buttons attached to the tibia and fibula.There is no risk of hardware failure or need for device removal with this method.Furthermore, studies report that the functional outcomes are equal or superior to that achieved with screw fixation and that TightRope fixation allows earlier RTP[6,30].
ANKLE FRACTURES
Mechanism of injury
In sports, ankle fractures generally occur alongside ankle sprains and therefore result from a wide variety of trauma.The commonest mechanism of injury is an external rotation force acting on a supinated foot transferred through the talus to the malleoli[36].Any of the malleoli can be injured: lateral, medial or posterior.Their fracture pattern can be unimalleolar, bimalleolar (typically lateral and medial) or trimalleolar.Trimalleolar fractures indicate a high energy transfer injury resulting in soft tissue damage and a higher risk of complications.In bimalleolar equivalent fractures, the medial ligament is injured alongside the fibula or the lateral malleolus, making the ankle unstable.Alternatively, disruption of the distal tibiofibular syndesmosis or a medial malleolar fracture combined with a fracture of the proximal head of the fibula is known as a Maisonneuve fracture.Pilon fractures involve a break in the tibia near the ankle and often the fibula too.The fracture pattern is dependent on the direction of the external force and the positioning of the foot at the time of injury[12,36].
History
Symptoms include immediate severe pain, swelling, bruising, tenderness and an inability to bear weight on the affected foot.If the ankle joint is dislocated, a gross deformity can be seen.A thorough history should be undertaken including mechanism of injury, the position of the foot and the force of impact, all which can help determine the injury patterns and therefore whether ankle stability is compromised.It is important to identify medications.For instance, long-term use of corticosteroids may increase the risk of osteoporosis and fractures.A history of smoking and chronic medical conditions such as peripheral vascular disease and metabolic bone disease should be noted as these affect treatment plans.Other important aspects of the history include occupation if not a professional athlete and living conditions (for example, whether there are stairs in the house)[12,14,36,37].
Physical examination
Along with palpation of the ankle joint and proximal fibula and tibia, an assessment of the neurovascular status and a thorough examination of the soft tissue should be carried out.The joints above and below the ankle joint (knee and foot, respectively) as well as active and passive range of movement of the ankle joint should be checked.A thorough motor and sensory examination is key to determining whether any neurological deficits seen postoperatively are caused due to the fracture or due to iatrogenesis such as a regional nerve block.Tenderness over the proximal fibula suggests a Maisonneuve fracture.Any gross deformities should be reduced as soon as possible under conscious sedation or with an intra-articular block to reduce neurovascular and soft tissue complication risks[12,36].
Investigations
The Ottawa Ankle Rules indicate when an ankle X-ray is required.The rules state that pain in the malleolar zone and one of bony tenderness in the distal 6 cm of the posterior edge of medial malleolus, bony tenderness in the distal 6 cm of the posterior edge of lateral malleolus or inability to bear weight immediately or in the Emergency Department necessitate imaging[38].X-rays should be standard three view images in AP, lateral and mortise views.The mortise film should be obtained with the foot rotated approximately 15° internally so that the shadow of the tibia on the fibula is eliminated.MRI is not routinely indicated for ankle fractures but may be useful later on to assess concurrent ligamentous injuries.Computed tomography scans are particularly useful in Pilon fractures to further delineate the exact fracture pattern and help facilitate preoperative planning and guide surgical fixation strategies[39].
Classification
There are two classification systems for ankle fractures.The Danis-Weber system is anatomic and categorises fractures based on their location on the fibula in relation to the syndesmosis.Type A fractures are infrasyndesmotic and do not usually cause ankle instability, type B is trans-syndesmotic, and type C is suprasyndesmotic.The Lauge-Hansen system classifies fractures based on the position of the foot and the direction of the force applied to it at the time of injury.Although comprehensive, it does not always reliably predict patterns of injury[12,36].
Nonoperative management
For stable fractures with minor / no displacement, provision of analgesia and cast immobilisation for 6 wk is sufficient to aid healing in most cases.This can slowly be progressed to crutch-assisted weight-bearing and physical therapy once the cast is removed.Throughout the period in cast immobilisation, radiographs are obtained at set intervals (1 wk, 2 wk and 6 wk) to monitor progress[40,41].Thromboprophylaxis is prescribed in adults during the time the lower leg is immobilised in cast and has been shown to be both clinically effective and cost-effective as it reduces the risk of venous thromboembolism, including both deep-vein thrombosis and pulmonary embolism[42].
Surgical intervention
Unstable and displaced medial and / or lateral malleolar fractures or posterior malleolar fractures greater than a third of the articular surface of the distal tibia with talar tilt and / or talar shift require surgical intervention.This is commonly done by open reduction and internal fixation using a variety of documented surgical techniques with various hardware to achieve anatomic realignment of the fracture.A period of postoperative cast immobilisation is common practice.Thereafter a structured physiotherapy rehabilitation programme to progress the patient back to preinjury level of activity is recommended[37,40,41].
CONCLUSION
The high incidence of ankle sprains and fractures in the athletic population necessitates rapid diagnosis to prevent long-term functional limitations.As these injuries have overlapping symptoms, it is vital to differentiate between them using the history, physical examination and imaging studies.An accurate diagnosis leads to prompt treatment and enables earlier recovery and RTP for the athlete.As the majority of injuries can be treated with the PRICE approach, immobilisation and rehabilitation, surgery is reserved for soft-tissue injuries that are refractory to conservative treatment or displaced and unstable ankle fractures.
 World Journal of Meta-Analysis2021年2期
World Journal of Meta-Analysis2021年2期
- World Journal of Meta-Analysis的其它文章
- Helicobacter pylori infection and susceptibility to cardiac syndrome X: A systematic review and meta-analysis
- Laboratory hematologic features of COVID-19 associated liver injury:A systematic review
- Therapeutic applications of dental pulp stem cells in regenerating dental, periodontal and oral-related structures
- Nonalcoholic fatty liver disease and cardiovascular concerns: The time for hepatologist and cardiologist close collaboration
- Metabolic and biological changes in children with obesity and diabetes
- Viral hepatitis: A brief introduction, review of management,advances and challenges