
Quantitative assessment of choroidal vascular sublayers in patients with pre-eclampsia compared to healthy pregnant women
2021-04-12 07:13
国际眼科杂志 2021年4期
Abstract
INTRODUCTION
Pre-eclampsia (PE) is a major cause of maternal, fetal, or newborn mortality and morbidity[1]. PE is defined as the onset of new or worsening of existing hypertension with proteinuria after the 20wk of gestation[2]. PE is a complex disease characterized by thrombocytopenia, elevated liver transaminases, renal insufficiency, and lung edema. Visual or cerebral dysfunction frequently are reported as clinical symptoms in PE. Abnormal visual symptoms associated with PE include blurry vision, temporary loss of vision, diplopia, and photopsia, among others[3]. Optical coherence tomography (OCT) is a valuable tool for detecting alterations in the choroid layer of the eye. Numerous studies have utilized spectral-domain OCT (SD-OCT) to measure the choroidal thickness (CT) to assess the relationship between CT and the pathogenesis of a range of ocular disorders, including age-related macular degeneration (ARMD), central serous chorioretinopathy (CSC), and high myopia[4-6]. It has been shown that PE can lead to increased CT[7-8]. Quantitative studies on the vascular sublayers of the choroid, such as the thickness of the large choroidal vessels (Haller’s layer) (LCVT)and the medium choroidal vessels (Sattler’s layer) (MCVT), have contributed to a better understanding of the choroid in the pathophysiology of CSC or myopic eyes[9-10]. The aim of this study was to analyze CT at five different locations in the choroid as well as the LCVT and MCVT in women diagnosed with PE. The data presented here suggest a possible role of alterations in the choroidal vascular sublayers associated with PE in the pathogenesis of visual disturbances.
SUBJECTS AND METHODS
This cross-sectional observational study was carried out in Beijing Anzhen Hospital at the Capital Medical University in China. This study obtained approval from the Ethics Committee of Beijing Anzhen Hospital and was conducted in accordance with the Declaration of Helsinki. All participants provided written informed consent prior to being enrolled in the study, also agreed to publish these findings and figures.
SubjectsThis study was comprised of a total of 100 women, including 40 normal non-pregnant individuals (normal group), 23 healthy pregnant women (healthy pregnancy group), and 37 women diagnosed with PE (PE group). A comparative analysis was performed on the thickness of the total choroid, Sattler’s layer, and Haller’s layer among the different groups. We measured CT at the fovea, as well as four other sites that were 750 μm temporal/nasal or 1500 μm temporal/nasal to the fovea, and the five sites were designated as SFCT, T750, N750, T1500, and N1500, respectively. All study subjects were Han Chinese, and the patients included in this study were recruited from May 2016 to October 2018 from Ophthalmology Clinics.
CriteriaThe criteria for inclusion were as follows: 1) Healthy pregnant women were included who were in their third trimester of a singleton pregnancy and exhibited a spherical equivalent (SE) ranging from -6 D to 6 D; 2) PE patients who displayed hypertension (BP≥140/90 mmHg) after 20wk of gestation and new-onset proteinuria, which was defined as having a dipstick reading ≥+ or a 24h urine collection ≥0.3g/d); 3) Healthy control individuals included non-pregnant women aged 20-40 with a SE that ranged from -6 D to 6 D. Individuals were excluded from this study for the following reasons. The individual had undergone previous ocular surgery, had a history of smoking, or was diagnosed with any systemic disorder, including chronic hypertension, diabetes, anemia, and renal, rheumatic, or cardiovascular disease.
A comprehensive ocular examination was performed that included best corrected visual acuity testing, non-contact tonometry (Canon CT-80A), SE refractive errors (Canon Autorefractor RK-F1), slit-lamp biomicroscopy, and SD-OCT (Topcon 3D-OCT-1000 Mark II). The choroid mode was used to acquire choroidal images. First, we used eye-tracking technology to conduct a 6 mm single line scan for which the scans were captured 50 times for each location. Then, high-resolution images were obtained by averaging 50 B-scans using the software.
In this study, CT, LCVT, and MCVT were defined, respectively, as the vertical distance from the posterior rim of the hyperreflective retinal pigment epithelium to the choroidoscleral border, a thick layer of oval hyperreflective profiling with hyporeflective cores in the outer choroid, and the thickness of medium vessels and the choriocapillaries. Accordingly, the measurements were carried out as follows. The fovea and four other sites that were 750 μm temporal and nasal or 1500 μm temporal and nasal to the fovea were chosen to assess CT. The LCVT was determined perpendicularly from the inner rim of the sclera to the innermost point of a selected large vessel of the choroid, as illustrated elsewhere[10-11]. The MCVT was determined by deducting the thickness of the large vessel from the SFCT, as shown in Figure 1.
The OCT scans were performed in the afternoon between 1 p.m. and 4 p.m. for all subjects. The above measurements were carried out independently by two experienced examiners using the built-in caliper application included in the OCT software. The average values of these parameters were subjected to statistical analysis. The two examiners were blinded as to the group identity of the study subjects. This study included one of the two eyes with good image quality from each subject.

Table 1 Demographic characteristics and choroidal thickness measurements among the three indicated groups
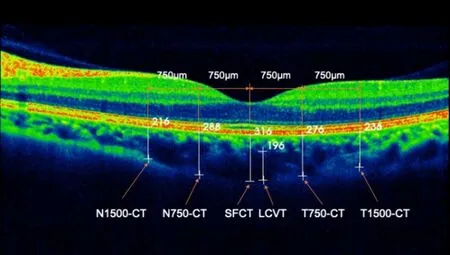
Figure 1 SD-OCT showing choroidal thickness measurements including SFCT, LCVT, CT at 750 μm temporal/nasal, or 1500 μm temporal/nasal to the fovea.
StatisticalAnalysisSPSS Statistics version 23.0 (IBM-SPSS, Chicago, USA) was used to conduct statistical analysis. The data were presented as means±SD. The Kruskal-Wallis test, Mann-WhitneyU-test, and a paired-samplet-test were used to analyze the differences in age, SE, CT, LCVT, and MCVT among the three groups, differences in age, SE, gestational age, CT, LCVT, and MCVT between every two groups, and the difference in CT between the temporal and nasal areas, respectively. Statistically,P<0.05 was used to determine significance.
RESULTS
DemographicCharacteristicsA total of 100 women aged 20-41 years, with a mean age of 30.61±4.39 years, were included in the study. The subjects were divided into three groups: 37 patients diagnosed with PE (ages 27-41 years), 23 healthy pregnant women (ages 23-38 years), and 40 normal non-pregnant women (ages 20-36 years). Among the 37 PE patients, five eventually progressed to eclampsia. As summarized in Table 1, no significant difference was observed among the three groups for the mean age (P=0.240) or the SE (P=0.338). Likewise, no differences were observed in the gestational age among the healthy pregnancy and patient groups (P=0.783).
ChoroidalThicknessMeasurementThe measurements for choroidal thickness are shown in Table 1. There were significant differences in LCVT, MCVT, and CT at various indicated locations among the three groups (P<0.05 for each measurement). In the normal, non-pregnant group, T1500-CT (238.20±44.73 μm) was significantly greater than N1500-CT (209.53±60.32 μm) (P<0.05). On the other hand, no difference was detected between N1500-CT and T1500-CT in either the healthy pregnancy or PE groups. Likewise, T750-CT (243.93±54.29 μm) was markedly increased compared with N750-CT (230.73±61.76 μm) in the normal group (P<0.05). In contrast, there was no significant difference between N750-CT and T750-CT in either the healthy pregnant women or PE patients. Comparative analysis revealed a significant difference in LCVT among the normal (173.88±55.76 μm), healthy pregnancy (214.13±43.57 μm), and PE (252.35±70.19 μm) groups (P<0.05). A significant difference in MCVT was found among the normal (79.48±28.08 μm), healthy pregnancy (95.26±18.73 μm), and PE patient (94.51±26.85 μm) groups (P<0.05). In this case, the difference between the normal group and healthy pregnancy or PE group was significant (P<0.05), but the healthy pregnancy and PE groups were not different from each other (P>0.05).
DISCUSSION
The retina has high metabolic demands, and the choroid provides over 85% of the blood flow for the eye, including the outer retina. Altered choroidal blood flow or changes in hemodynamics may cause dysfunction and death of retinal photoreceptors[12]. Thus, the choroid has been critically involved in the pathogenesis of various ocular disorders, such as ARMD, CSC, and diabetic retinopathy[4,13-14].
Here, we presented the first report that the total CT, the thickness of Haller’s layer, and CT of medium vessels were measured in healthy pregnant women and patients with PE. A previous study reported that CT was increased in healthy pregnant women compared to normal non-pregnant women[15]. Likewise, it has been shown that SFCT in healthy pregnant women was significantly greater than in normal non-pregnant subjects. This observation might be attributed to pregnancy-related physiological changes in hemodynamics that include enhanced cardiac output and arterial compliance, as well as reduced systemic vascular resistance[16]. By contrast, other studies have shown that the difference in CT was statistically insignificant between healthy non-pregnant and pregnant women in their third trimester[17-18]. In the present report, we identified a significant increase in LCVT, MCVT, and CT at five locations in healthy pregnant women compared with non-pregnant women. Notably, in the normal non-pregnant group, T1500-CT and T750-CT were significantly greater than N1500-CT and N750-CT, respectively, whereas no significant difference was detected between N1500-CT and T1500-CT or N750-CT and T750-CT in the healthy pregnancy or PE patient group. These findings revealed that the nasal CT increased more than the temporal CT in normal pregnant women and pregnant subjects suffering from PE. Recently, a study hypothesized that choroidal thickening in PE begins in the nasal area[19].
A number of studies have been conducted to compare CT between normal pregnant women and PE patients. In one study, CT was compared during the postpartum period among 15 women who experienced PE during pregnancy, 15 normal pregnant women, and 19 healthy non-pregnant women. The comparative analysis revealed that CT was significantly increased in women who had experienced PE compared with control subjects[8]. This observation could be attributed to increased expression of vascular endothelial growth factor. Similarly, another study reported that CT in PE patients was significantly greater than that in healthy non-pregnant or pregnant women[7]. That study showed that PE rather than pregnancy itself was likely to elicit an increase in CT, suggesting an inductive role of other unidentified hyperpermeability factors during pregnancy[7]. However, the specific layer (s) implicated in the increased CT remained to be determined. In the present study, we observed that increased CT occurred in the choroidal sublayers. Specifically, we found that while significantly increased CT and LCVT were detected in the PE patients compared with the healthy pregnant women, the difference in MCVT was insignificant. Our findings imply that the thickening of Haller’s layer might be the cause of the increase in CT detected in PE patients.
PE is a hypertension-associated disease that can lead to multiple organ failure in the mother as well as fetal distress[20]. This disease is characterized by hypovolemia, which is linked to increased sympathetic activity[21]. The choroid has large, membrane-lined lacunae, nonvascular smooth muscle cells (NVSMCs), and intrinsic choroidal neurons that receive sympathetic, parasympathetic, and nitrergic innervation[22]. The parasympathetic innervation regulates vasodilation and increases blood flow in the choroid. Conversely, the sympathetic innervation controls vasoconstriction and decreases blood flow in the choroid. In addition, sensory input conveys information about pain and thermal sensations centrally, acts locally in vasodilation, and facilitates blood flow[23]. One study[24]suggested that increased sympathetic regulation and decreased parasympathetic input occurred during normal pregnancy, and enhancement of the changes described above could be detected in pregnant women with PE. In such circumstances, there could be alternative causes for choroidal thickening. Chungetal[9]reported that the NVSMCs might be the cause of the thickening of Haller’s layer observed in CSC. Given that pregnancy is considered to be a risk factor for CSC, especially in the third trimester[25], the choroidal thickening in PE patients may involve a mechanism that is similar to that observed in CSC.
In this study, we observed that the difference in MCVT between healthy non-pregnant and pregnant women was significant. In contrast, no significant difference was observed between healthy pregnant women and PE patients. This observation concerning the MCVT was different from what was observed for the LCVT. In this case, it is crucial to investigate how the choroidal thickening is related to blood flow within the choroid. We reasoned that increased LCVT in normal pregnant women could be protective, based on the observation that the thickening in Haller’s layer was attributed to stromal expansion. Several factors limited this study. First, the number of enrolled subjects was relatively small. Second, the sympathetic, parasympathetic, and sensory fibers, as well as their terminals appeared to be distributed in arterial walls and the choroidal veins, and not in choriocapillaries. In this study, we chose to combine choriocapillaries with the medium vessel layer of the choroid, because the separation of choriocapillaries from the vessel layer is difficult using SD-OCT. Lastly, we did not collect panel data from the patients after pregnancy. Therefore, a large-scale and longitudinal investigation needs to be conducted to address this issue.
In summary, we demonstrated that while CT at five sites and LCVT were significantly increased in women with PE, a marked increase in CT at four sites as well as MCVT also was detected in healthy pregnant women. These data suggest that parasympathetic and sympathetic mediated regulation and NVSMCs play a role in the thickness variation observed in the choroidal vascular sublayers in pregnancy and PE.
