
上海郊区某社区老年衰弱患病率及生活方式影响因素分析
2021-03-18 03:32:13黄建华陈川陈久林潘丽红宋海萍
上海医药 2021年4期
黄建华 陈川 陈久林 潘丽红 宋海萍

摘 要 目的:分析上海郊區某社区老年衰弱患病率及生活方式影响因素,为社区老年衰弱防治提供依据。方法:在社区老年健康体检人群中,分级抽取527例60岁及以上老年人进行调查。年龄63~89岁,平均年龄为(71.70±5.75)岁;其中男性222人,平均年龄为(71.71±5.59)岁;女性305人,平均年龄为(71.69±5.87)岁。通过现场采集病史及Fried衰弱表型量表等信息,测定4米步速及握力,分析老年衰弱的患病率及影响因素。结果:社区老年衰弱患病率8.0%,男性患病率低于女性(3.2%比11.5%,P<0.01),女性老年人衰弱患病率随年龄增加而升高(P<0.01)。相较于无衰弱老人,衰弱前期、衰弱老人的年龄(P<0.01)和慢病数量增加(P<0.05)。文盲或半文盲、小学、初中文化老人衰弱患病率依次为12.5%、4.1%、1.7%(P<0.01);丧偶老人患病率高于已婚老人(15.4%比6.5%,P<0.01);独居老人患病率高于同住老人(15.2%比6.7%,P<0.01)。Logistic回归分析显示,女性、高龄、慢病数量是社区老年衰弱的危险因素,与人同住、多锻炼是保护因素。结论:上海郊区某社区老人衰弱患病率8.0%,性别、年龄、居住状况、锻炼次数和慢病数量是老年衰弱的影响因素。
关键词 老年衰弱;患病率;影响因素;Fried衰弱表型
中图分类号:R592 文献标志码:A 文章编号:1006-1533(2021)04-0033-04
Analysis of the prevalence of frailty and influencing factors of lifestyle in a community in the suburbs of Shanghai
HUANG Jianhua1, CHEN Chuan2, CHEN Jiulin2, PAN Lihong1, SONG Haiping1(1. General Practice Department of Situan Community Health Service Center of Fengxian District, Shanghai 201413, China; 2. Basic Research Office of Institute of Geriatrics of Traditional Chinese Medicine, Shanghai 200031, China)
ABSTRACT Objective: To analyze the prevalence of frailty and influencing factors of lifestyle in a community in the outer suburbs of Shanghai to provide evidence for the prevention and treatment of frailty in the community. Methods: In the community elderly health check-up population, 527 cases of the elderly over 60 years old were selected for investigation. The age was from 63 to 89 years old, and the average age was (71.70±5.75) years old; among them, there were 222 males with an average age of (71.71±5.59) years; there were 305 females with an average age of (71.69±5.87) years. Through field collection of medical history and Fried frailty phenotype scale and other information, and 4m pace and grip strength measurement, the prevalence and influencing factors of frailty in the elderly were analyzed. Results: The prevalence of frail elderly in the community was 8.0%, the prevalence of the male was lower than that of the female (3.2% vs 11.5%, P<0.01), and the prevalence of female elderly frailty increased with age(P<0.01). Compared with the non-debilitated elderly, the age of the pre-debilitated, and debilitated elderly(P<0.01), and the number of chronic diseases increased(P<0.05). The prevalence of frailty among illiterate or semiilliterate, elementary and junior high school seniors was 12.5%, 4.1%, and 1.7%(P<0.01); the prevalence of the elderly living alone was higher than that of the elderly living together(15.2% vs. 6.7%, P<0.01). Logistic regression analysis showed that women, advanced age, and the number of chronic diseases were risk factors for elderly debilitating in the community, while living with others and exercising were protective factors. Conclusion: The prevalence of frailty among the elderly in a community in the suburbs of Shanghai is 8.0%, and gender, age, living status, exercise frequency and the number of chronic diseases are the influencing factors of frailty in the elderly.
KEY WORDS frailty; prevalence; influence factor; Fried frailty phenotype
截至2018年底,我国65岁及以上老年人接近1.67亿,占总人口的11.9%[1];预计2050年老年人口将增长到4.83亿,老年人口占比将升至34.1%[2]。随着老年人口的增长,老年人健康日益引起关注,老年衰弱成为近年来老年医学研究的热点之一。老年衰弱是“由于年龄相关神经肌肉、代谢和免疫系统的生理储备下降,从而更易受应激因素影响的状态”[3]。衰弱与跌倒、失能、谵妄、死亡、残疾等负面事件密切相关[4-5]。老年衰弱及其不良后果影响患者的健康,给家庭和社会增加了负担。本研究旨在分析社區老年衰弱患病率及其影响因素,为社区老年衰弱的健康管理提供依据。
1 对象与方法
1.1 对象
于2019年6-9月对在上海市奉贤区四团社区卫生服务中心进行健康体检的60岁及以上老年人通过分级抽样,抽取527例老年人进行调查。年龄63~89岁,平均年龄为(71.70±5.75)岁;其中男性222人,平均年龄为(71.71±5.59)岁;女性305人,平均年龄为(71.69±5.87)岁。
纳入标准:(1)年龄≥60岁,性别不限;(2)上海市户籍,并在本研究实施的社区长期居住(≥5年);(3)具备基本沟通能力和理解能力;(4)愿意签订本次研究的知情同意书者。排除标准:(1)躯体功能因脑卒中、帕金森氏症、肿瘤、骨折等疾病或残疾而受影响者;(2)患有精神分裂症、抑郁症、焦虑症等精神疾病并依赖药物控制者;(3)阿尔茨海默病或有明显认知功能障碍者;(4)不愿意签订知情同意书者。本研究经上海市中医药大学附属龙华医院伦理委员会审核批准。
1.2 方法
1.2.1 调查内容
(1)一般资料。采用自制一般资料调查问卷,由经过统一培训的调查员询问老人后填写。内容包括:姓名、性别、年龄、婚姻状况、文化程度、居住状况、饮食习惯、锻炼次数及方式、吸烟史、饮酒史、既往史等。(2)人体学指标信息从上海市奉贤区四团社区卫生服务中心体检数据库导出。内容包括:身高、体质量、腰围、臀围、步速、握力。步速采用4 m固定距离,测量受试者以平常步速经过的时间,以米/秒(m/s)表示。握力使用握力计,单位为千克(kg),测量时,受试者两脚自然分开站立,两臂自然下垂,手持握力计用力达到最大值持续3 s,记录读数,左右手交替进行,各2次,取最大值。(3)疲劳感与体能由经过培训的调查员采用Fried衰弱表型(Fried Frailty Phenotype,FP)量表询问老人后填写[6]。
1.2.2 衰弱评定
FP是以体质量减轻[(当年体质量-去年体质量)/去年体质量×100%<-5%]、步速减慢(步速≤0.8 m/s)、肌力减退(男性握力≤25 kg,女性握力≤18 kg)、疲劳感、低体能等5项临床表型进行评估;符合3项及以上,评估为衰弱;符合1~2项为衰弱前期;无符合项为无衰弱[6]。
1.3 统计学分析
2 结果
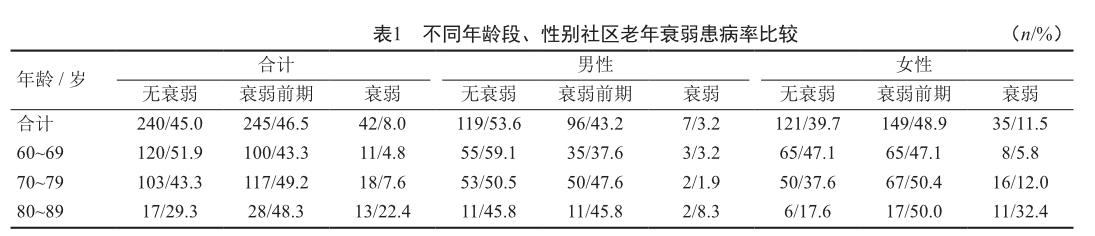
2.1 社区老年衰弱患病率及年龄、性别分布
527例老年人中,衰弱前期245人,占46.5%;衰弱者42人,占8.0%。女性衰弱患病率明显高于男性(c2=17.511,P<0.01)。男性老年人,各年龄段衰弱患病率差异无统计学意义(P>0.05),女性老年人衰弱患病率随年龄增长而升高,差异有统计学意义(c2=23.209,P<0.01)。见表1。
2.2 不同文化程度和生活方式的社区老年人衰弱患病率的比较
文盲或半文盲、小学、初中文化老人的衰弱患病率依次为12.5%、4.1%、1.7%,在高中及以上文化老人中未发现衰弱患者,不同文化程度老年人的衰弱患病率差异有统计学意义(P=0.005)。不同婚姻状况和不同居住状况老年人的衰弱患病率差异有统计学意义(P<0.01)。见2。
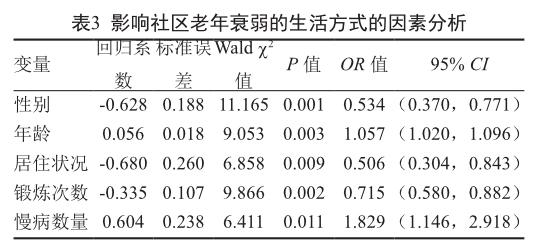
2.3 影响社区老年衰弱的生活方式的回归分析
以衰弱分期为因变量(赋值:0=无衰弱、1=有衰弱及衰弱前期),以性别(赋值:0=女性,1=男性)、年龄、婚姻状况、文化程度、居住状况、饮食习惯、锻炼次数及方式、吸烟史、饮酒史、既往病史、慢病数量为自变量,采用二元Logistic回归向前步进模型进行回归分析。结果显示,性别、年龄、居住状况、锻炼次数和慢病数量是老年衰弱的影响因素,女性、高龄、基础疾病多是社区老年衰弱的风险因素,同住、多锻炼则是保护因素。见表3。
3 讨论
在老年人群早期识别衰弱,了解辖区老年衰弱患病状况是社区老年人健康管理的重要组成部分。美国一项社区男性老年居民的研究发现,衰弱及衰弱前期患病率分别为4%和40%[7]。北京市衰弱、衰弱前期患病率分别为11.1%、45.7%[8],广州市衰弱、衰弱前期患病率分别为10.3%、30.7%[9],哈尔滨市的衰弱患病率高达49%[10]。本研究发现,辖区内60岁及以上老人衰弱患病率8.0%、衰弱前期46.5%,男性衰弱患病率3.2%、衰弱前期43.2%,女性衰弱患病率11.5%、衰弱前期48.9%,与Wong等[11]的研究结果类似。本次研究结果显示,女性老年人的衰弱患病率随年龄增长明显增加,提示女性的衰弱患病率更有年龄依耐性,这可能是因为女性内分泌系统的变化导致了肌肉减少和肌力衰退[12]。Woo等[13]研究认为,多病状态(3种及以上)是衰弱的危险因素。本研究结果也显示慢病数量是老年衰弱的影响因素。因此,社区的老年健康管理应重视共病管理。
受教育程度较高人群自我保健意识较强,可能影响其健康水平。Ophetveld等[14]发现,低、中、高受教育水平的老年人衰弱患病率分别为78.8%、16.2%、5.0%。本研究结果显示,高中及以上文化老人中未发现衰弱患者,在文盲或半文盲、小学、初中文化老人的衰弱患病率依次降低,表明受教育程度越高衰弱患病率越低。有研究结果显示,已婚老年人的衰弱患病率低于独居/丧偶/离异老人[15-16]。本研究结果也显示,已婚老人衰弱患病率低于丧偶老人;同住老人患病率低于独居老人。回归分析显示,女性、高龄、基础疾病多是衰弱的风险因素,与人同住、多锻炼是其保护因素。因此,鼓励老年人参与社区活动、坚持适量体力活动,减少基础疾病有利于降低衰弱风险。
綜上,衰弱是年龄、性别、生活方式、多病共存等多种因素共同作用,是导致老年人生理储备累积损失的结果。社区医护人员应通过健康宣教等方式促进老年人群改善生活方式、加强体力运动,并重视多病老年人的共病管理,提高老年人生活质量。
参考文献
[1] 中华人民共和国国家统计局. 中国统计年鉴[M]. 北京: 中国统计出版社, 2019: 75.
[2] 总报告起草组. 国家应对人口老龄化战略研究总报告[J].老龄科学研究, 2015, 3(3): 4-38.
[3] Walston J, Hadley EC, Ferrucci L, et al. Research agenda for frailty in older adults: toward a better understanding of physiology and etiology: summary from the American Geriatrics Society/National Institute on Aging Research Conference on Frailty in Older Adults[J]. J Am Geriatr Soc. 2006, 54(6): 991-1001.
[4] Bandeen-Roche K, Xue QL, Ferrucci L, et al. Phenotype of frailty: characterization in the womens health and aging studies[J]. J Gerontol A Biol Sci Med Sci, 2006, 61(3): 262-266.
[5] Ensrud KE, Ewing SK, Cawthon PM, et al. A comparison of frailty indexes for the prediction of falls, disability, fractures, and mortality in older men[J]. J Am Geriatr Soc, 2009, 57(3): 492-498.
[6] Fried LP, Ferrucci L, Darer J, et al. Untangling the concepts of disability, frailty, and comorbidity: implications for improved targeting and care[J]. J Gerontol A Biol Sci Med Sci. 2004, 59(3): 255-263.
[7] Cawthon PM, Marshall LM, Michael Y, et al. Frailty in older men: prevalence, progression, and relationship with mortality[J]. J Am Geriatr Soc. 2007, 55(8): 1216-1223.
[8] 奚兴, 郭桂芳. 社区老年人衰弱现状及其影响因素研究[J]. 中国护理管理, 2014, 14(12): 1315-1319.
[9] 任青卓, 周静静, 郑雅婧, 等. 广州市老年人衰弱现状及其影响因素[J]. 中国公共卫生, 2019, 35(4): 413-417.
[10] 李阳, 张立萍, 罗洋. 哈尔滨市社区老年人衰弱现状及其影响因素调查[J]. 护理研究, 2018, 32(2): 224-228.
[11] Wong CH, Weiss D, Sourial N, et al. Frailty and its association with disability and comorbidity in a communitydwelling sample of seniors in Montreal: a cross-sectional study[J]. Aging Clin Exp Res. 2010, 22(1): 54-62.
[12] Province MA, Hadley EC, Hornbrook MC, et al. The effects of exercise on falls in elderly patients. A preplanned meta-analysis of the FICSIT Trials. Frailty and Injuries: Cooperative Studies of Intervention Techniques[J]. JAMA. 1995, 273(17): 1341-1347.
[13] Woo J, Zheng Z, Leung J, et al. Prevalence of frailty and contributory factors in three Chinese populations with different socioeconomic and healthcare characteristics[J]. BMC Geriatr. 2015, 15: 163.
[14] Op het Veld LP, van Rossum E, Kempen GI, et al. Fried phenotype of frailty: cross-sectional comparison of three frailty stages on various health domains[J]. BMC Geriatr. 2015, 15: 77.
[15] Herr M, Robine JM, Pinot J, et al. Polypharmacy and frailty: prevalence, relationship, and impact on mortality in a French sample of 2350 old people[J]. Pharmacoepidemiol Drug Saf. 2015, 24(6): 637-646.
[16] Boulos C, Salameh P, Barberger-Gateau P. Malnutrition and frailty in community dwelling older adults living in a rural setting[J]. Clin Nutr. 2016, 35(1): 138-143.
猜你喜欢
健康体检与管理(2022年2期)2022-04-15 22:33:17
昆明医科大学学报(2021年1期)2021-02-07 01:06:44
中国科技博览(2016年18期)2016-10-19 06:39:44
中国市场(2016年36期)2016-10-19 03:54:01
中国市场(2016年35期)2016-10-19 02:30:10
商(2016年27期)2016-10-17 07:09:07
商(2016年27期)2016-10-17 04:40:12
科技视界(2016年20期)2016-09-29 13:45:52
中国男科学杂志(2016年9期)2016-03-20 15:00:09
中国健康心理学杂志(2015年5期)2015-09-05 09:55:52
