
Hydroxychloroquine alone or in combination with azithromycin and corrected QT prolongation in COVID-19 patients: A systematic review
2021-02-12 07:19HalehAshrafParhamGhafouriSinaKazemianAbbasSoleimaniAzadehSadatNaseriShahrokhKarbalaiAliKazemiSaeid
World Journal of Meta-Analysis 2021年6期
Haleh Ashraf, Parham Ghafouri, Sina Kazemian, Abbas Soleimani, Azadeh Sadat Naseri, Shahrokh Karbalai, Ali Kazemi Saeid
Haleh Ashraf, Research Development Center, Sina Hospital, Tehran University of Medical Sciences, Tehran 11367-46911, Iran
Haleh Ashraf, Sina Kazemian, Cardiac Primary Prevention Research Center (CPPRC), Tehran Heart Center, Tehran University of Medical Sciences, Tehran 11367-46911, Iran
Parham Ghafouri, Sina Kazemian, Students' Scientific Research Center (SSRC), Tehran University of Medical Sciences, Tehran 11367-46911, Iran
Parham Ghafouri, School of medicine, Tehran University of Medical Science, Tehran 11367-46911, Iran
Abbas Soleimani, Azadeh Sadat Naseri, Shahrokh Karbalai, Ali Kazemi Saeid, Department of Cardiology, Sina Hospital, Tehran University of Medical Sciences, Tehran 11367-46911, Iran
Abstract BACKGROUND Despite the controversies about the effectiveness of the current drug regimens for coronavirus disease 2019 (COVID-19), these drugs are still the only options available.Moreover, the safety of these drugs is yet to be confirmed.A serious concern is the occurrence of various cardiac arrhythmias, particularly QT prolongation.AIM To summarize the incidence and estimate the risk of QT interval prolongation in patients scheduling for conventional treatment (hydroxychloroquine alone or in combination with azithromycin) for COVID-19.METHODS We comprehensively searched Medline, Web of Knowledge, Google Scholar, Scopus, and Cochrane Central Register of Controlled Trials databases until October 31, 2020 for all eligible studies under the considered keywords COVID-19, arrhythmia, QT interval, therapy, azithromycin, and hydroxychloroquine until.The study protocols were established in compliance with PRISMA-P guidelines (Preferred Reporting Items for Systematic Review and Meta-Analysis - Protocols), and a nine-star Newcastle-Ottawa Scale scoring system was used to assess the methodological quality of all eligible studies.Outcome measures were corrected QT (QTc) prolongation, cardiac arrhythmias, or sudden cardiac death.RESULTS Fifteen studies enrolling 8298 patients with targeted COVID-19 therapeutic regimes were included.The eligible studies found a significant increase in the mean QTc interval following treatment with the described medications compared to baseline QTc with weighted standard differences in means of 0.766.The pooled prevalence rate of QTc prolongation was estimated to be 9.2% (95% confidence interval: 4.5% to 18.1%).CONCLUSION Hydroxychloroquine ± azithromycin regimen can significantly increase the risk of developing QTc prolongation.
Key Words: Azithromycin; COVID-19; Hydroxychloroquine; QTc interval
INTRODUCTION
With the outbreak of the coronavirus disease 2019 (COVID-19) pandemic, we have seen high mortality rates from the disease in almost all countries involved[1].Besides the pulmonary involvement in form of acute respiratory distress syndrome, one of the main features of this disease is the involvement of other systems, like cardiovascular, gastrointestinal, central nervous system, and even skin and mucosal involvement[2-4].However, respiratory failure and subsequent cardiovascular compromise were major determinants for patients' survival[5].So far, there are no successful and safe drug regimens for the treatment and prevention of COVID-19.Current approaches have either failed or have been withheld due to potential side effects.Thus, the side effects have added to the high mortality and morbidity caused by COVID-19[6].
Current evidence suggests that using hydroxychloroquine and azithromycin for COVID-19 increases the risk of cardiac arrhythmias[7,8].Previous studies reported that these drugs caused corrected QT (QTc) prolongation, leading to life-threatening conditions like torsades de pointes (TdP) and sudden cardiac death[9,10].Although bothin vivoandin vitrostudies recommended the combination therapy of azithromycin and hydroxychloroquine, even as the first-line approach in preventing disease, it has also led to QTc prolongation[11].In addition to cardiac monitoring, identifying patients, who are prone to the side effects, helps to minimize the potential harms.By identifying susceptible individuals, it may be possible to use other drug protocols to maintain patient survival.Herein, we summarize the findings about the prevalence and the risk of QTc prolongation in patients treated with hydroxychloroquine ± azithromycin.Also, we discuss the life-threatening conditions in patients taking these medications.
MATERIALS AND METHODS
Search strategy
We performed this review according to established methods and in compliance with PRISMA-P (Preferred Reporting Items for Systematic Review and Meta-Analysis) Protocols.Two investigators searched the manuscript databases including Medline, Web of Knowledge, Google Scholar, Scopus, and Cochrane Central Register of Controlled Trials in The Cochrane Library until October 31, 2020 for all eligible studies under the considered keywords including COVID-19, arrhythmia, QT interval, therapy, azithromycin, and hydroxychloroquine until.The studies were restricted to the English language.We included all randomized controlled trials, including individually randomized and cluster-randomized trials.We reviewed the studies reported as full-text and those published as abstracts.We also conducted a search of ClinicalTrials.gov and the World Health Organization International Clinical Trials Registry Platform Search Portal for ongoing or unpublished trials.The inclusion criterion was a study population of adult patients, who suffered from a definitive diagnosis of COVID-19 and were treated with at least one or a combination of these medications: hydroxychloroquine, chloroquine, and azithromycin.The exclusion criteria were: (1) A lack of clear and reproducible results; (2) Non-English studies; (3) Lack of access to the full texts of the articles; and (4) Case reports, case series, and review papers.If a subset of patients in a study met our inclusion criteria and data from this specific population were missing in the original publication, at first, we tried to contact the corresponding author to get the necessary data.Afterward, if the relevant data was not accessible, we only included the studies when more than 50% of the participants met the inclusion criteria.However, we performed sensitivity analysis and excluded studies in which < 100% of patients met the inclusion criteria.
Data abstraction and validity assessment
Two un-blinded reviewers performed the data abstraction independently in structured collection forms with no divergences in the data collection method.We resolved disagreements by consensus or by involving a third person.One of the authors transferred data into the Review Manager file.We double-checked for correct data entry, comparing the data presented in the systematic review with the data extraction form.The second author spotted-check study characteristics for accuracy against the trial report.The details will be assessed by systematically reviewing the manuscripts are as follows:
The study quality was evaluated based on the following criteria: (1) The systematic review and meta-analysis based on the questions primarily described and formulated; (2) Inclusion and exclusion criteria predefined in the studies as eligibility criteria; (3) Searching the literature performed on a systematic and comprehensive approach; (4) To minimize the bias, two authors reviewed the full texts of the articles; (5) The quality of included studies were rated independently by the reviewers for appraising internal validity; (6) The characteristics and findings of the studies were listed comprehensively; (7) The publication and risk of bias were listed; and (8) Heterogeneity was also assessed.The endpoints were to determine the overall prevalence of QT prolongation and estimate the occurrence of fatal arrhythmia.Along with pooled relative risk for QT prolongation, the year of publishing, the number of patients included, and the method of the design was also pointed.
Statistical analysis
We assessed the risk of bias for each study with the criteria outlined in the Cochrane Handbook for Systematic Reviews of Interventions.Any disagreement was resolved by discussion in the whole study team.We assessed the risk of bias according to the following domains: random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, and selective outcome reporting.We judged each potential source of bias as high, low, or unclear and provided a quote from the study report together with a justification for our judgment in the "Risk of bias" table.We summarized the risk of bias judgments across different studies for each of the domains listed.When considering therapeutical effects, we took the risk of bias into account for studies that contribute to that outcome.We contacted investigators or study sponsors to verify key study characteristics and obtain missing numerical outcome data where possible, for example, when a study is identified as abstract only.We used the RevMan calculator (version 5.3) to calculate missing standard deviations from other statistics, such as confidence intervals (CI) orP-values.Where it was not possible, we imputed the missing standard deviations and explored the impact of including such studies in the overall assessment of results by a sensitivity analysis.Dichotomous variables were reported as proportions and percentages, and continuous variables as mean values.Binary outcomes from individual studies were combined with both the Mantel-Hansel fixed-effect model.The risk ratios (RRs) and 95%CI for RR were used as summary statistics to compare dichotomous variables and to determine the likelihood of each adverse event after interventions.
We used Cochran's Q test to estimate the statistical heterogeneity, complemented with theI2statistic.It quantifies the proportion of total variation across studies that is due to heterogeneity rather than chance.A value ofI2of 0%-25% indicates insignificant heterogeneity, 26%-50% low heterogeneity, 51%-75% moderate heterogeneity, and 76%-100% high heterogeneity.Publication bias was assessed by the rank correlation test and also confirmed by the funnel plot analysis.The nine-star Newcastle-Ottawa Scale scoring system was employed to assess the methodological quality of all eligible studies.In this quality assessment technique, each study assessed qualitatively for the three criteria of (1) The selection of the study groups; (2) The comparability of study groups; and (3) The ascertainment of the outcome and is finally scored that the studies awarding 7 stars or over were deemed as high quality.Reported values were two-tailed, and hypothesis testing results were considered statistically significant atP= 0.05.Statistical analysis was performed using the Comprehensive Meta-Analysis Software (CMA, version 3.0).
RESULTS
Figure 1 demonstrates the flow diagram of the study selection.Initially, 133 articles were collected by database searching and other sources.After removing duplications, 116 records were primarily under-screened.Based on the titles and abstracts, 98 records were excluded, and the remaining 18 citations were assessed for further eligibility.Of those, 3 were also excluded due to incompleteness of the data and contents.Finally, 15 articles [12-26] were eligible for the final analysis (Figure 1).The studies included were assessed qualitatively by the QUADAS-2 tool.According to our risk of bias assessment, all 15 studies yielded good quality, and none of them had a high risk of bias.Therefore, the pooled results should be persuasive (Figure 2).In total, 15 studies (twelve retrospective and three prospective) were included in our final analysis.The anti-COVID-19 medications focused in the studies were mostly a combination of hydroxychloroquine plus azithromycin[13-24], hydroxychloroquine plus moxifloxacin[12], and hydroxychloroquine alone[25,26].Overall, 8298 patients suffering from COVID-19 were treated with these regimens.The details of the participants are summarized in Table 1.As shown in Table 2, all studies found a significant increase in the mean QTc compared to the baseline.The weighted standard differences in means are 0.766 (95%CI: 0.394 to 1.137,P <0.001), with significant heterogeneity across the studies relevant to the I2value of 99.33% (P <0.001) (Figures 3 and 4).In this regard, the pooled prevalence rate of QT prolongation was estimated to be 9.2% (95%CI: 4.5% to 18.1%) with a significant level of heterogeneity across the studies (I2= 98.10%,P <0.001).The Egger test also detected significant publication bias for all assessments.
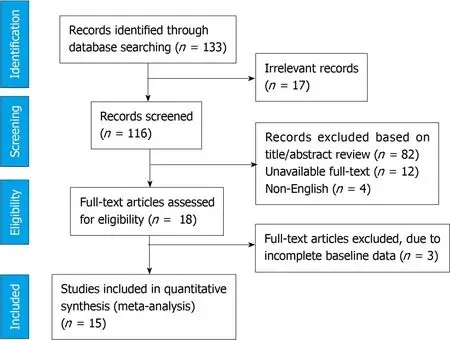
Figure 1 The flowchart of screening the eligible studies.
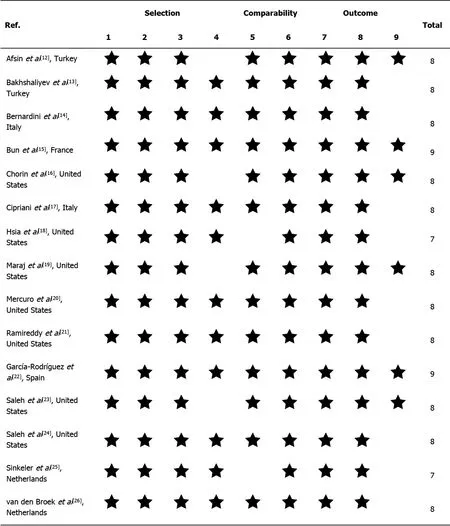
Figure 2 The quality assessment of the studies according to the nine-star Newcastle-Ottawa Scale scoring system.
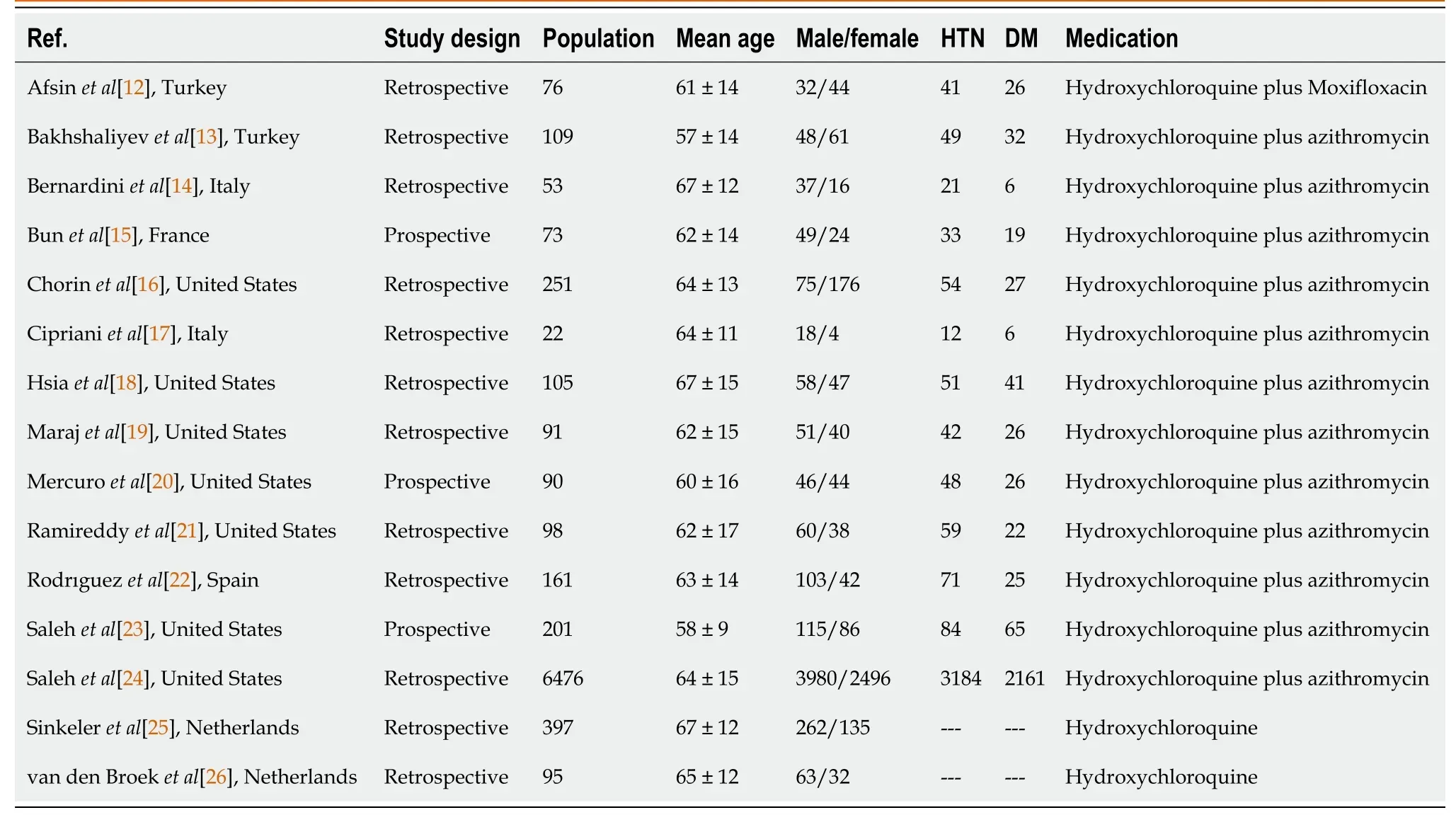
Table 1 The baseline details of studies included in meta-analysis
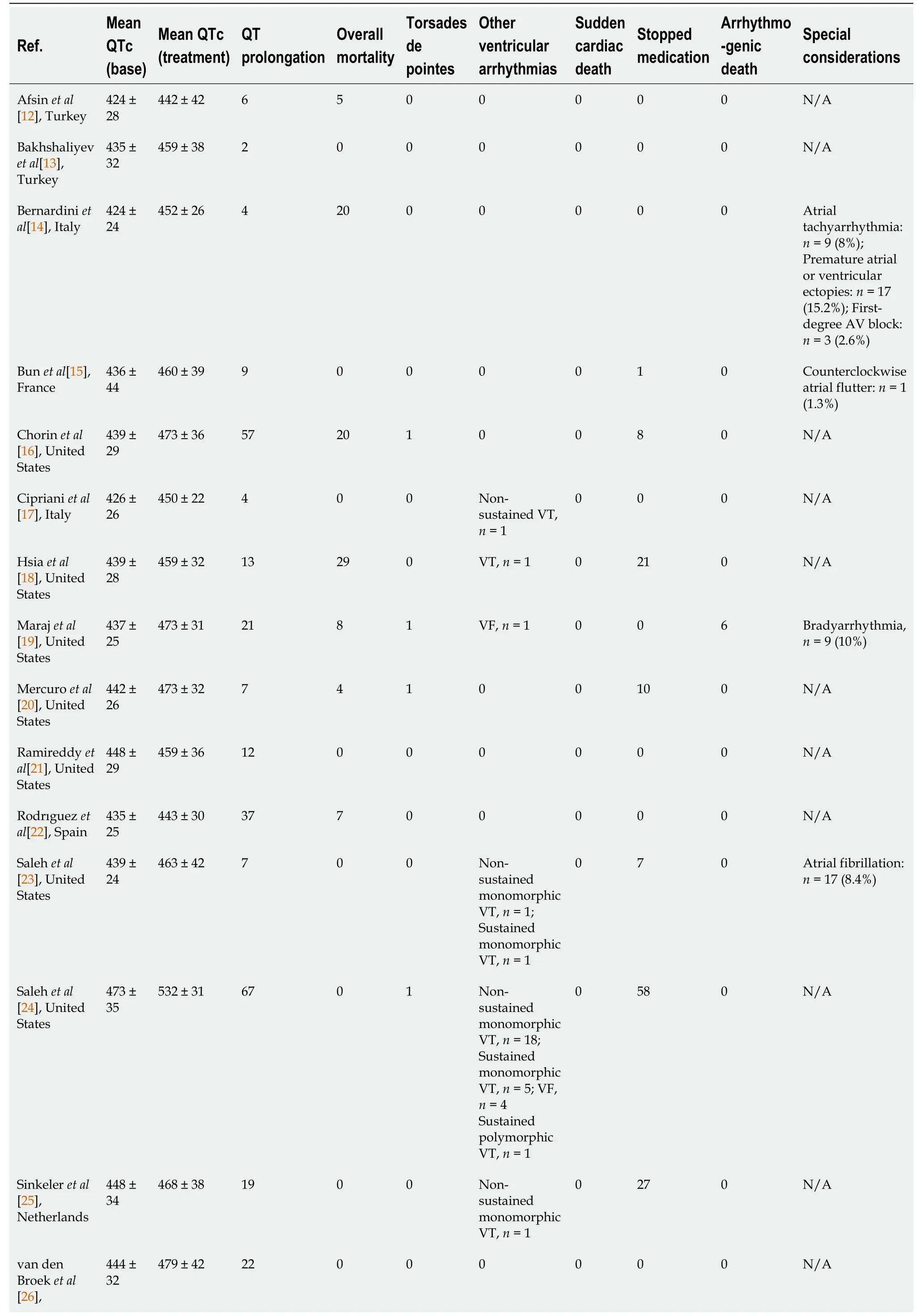
Table 2 The change in QTc interval and pooled prevalence of QT prolongation following medication
Across all studies, 132 patients stopped taking the medications due to QTc ≥ 500 ms or an increase of more than 60 ms in QTc.The pooled prevalence was 0.9% (95%CI: 0.6% to 1.1%) with significant level of heterogeneity across the studies (I2= 81.50%,P< 0.001).
Studies did not report any mortality caused by sudden cardiac death or arrhythmogenic death.However, 4 cases of TdP and 34 cases of ventricular tachycardia/fibrillation were reported with a pooled prevalence of 0.1% < and 0.4% (95%CI: 0.2% to 0.5%), respectively.
DISCUSSION
There are controversies about the effectiveness and safety of medications used to treat COVID-19.In some cases, serious side effects following the use of these drugs may contribute to the morbidity caused by the disease and even may lead to its progression.QTc prolongation is a potential side effect of hydroxychloroquine and, also, one of the most critical complications, leading to some fatal arrhythmias like TdP.Interestingly, mechanisms other than drug-related toxicity have been suggested to cause QTc prolongation.In this regard, we can mention cardiac ischemia due to direct viral invasion, electrolyte imbalances, activation of inflammatory cascades, and oxidative stress destroying myocardial tissue[27].Studies have shown that myocardial ischemia may result in repolarization abnormality leading to cardiac arrhythmias[28].Also, inflammatory processes, per se, may lead to disruption of cardiomyocyte ion channels by enhancing inward calcium currents and delaying outward potassium currents.It causes prolonged action potential duration and stimulation of cardiomyocytes[29].Therefore, the occurrence of such arrhythmia may not be primarily related to drug-induced toxicity.However, our study shows a significant increase in QTc after taking hydroxychloroquine/chloroquine.These findings are in line with the previous studies, which suggest that QTc prolongation is due to drug toxicity.Further interventional studies and clinical trials are required to find an explanation for this controversy.
Besides, there is strong evidence that using azithromycin can induce QTc prolongation.According to case-control studies, azithromycin has increased the risk of QTc prolongation up to 1.5 times[30].Of course, it seems that pre-existing cardiovascular conditions or concomitant use of other QT-prolonging drugs are the conditions for the effectiveness of this drug are in inducing arrhythmia[31].
Overall, a significant proportion of patients with COVID-19 have experienced QTc prolongation.According to our meta-analysis, 4.5% to 18.1% of COVID-19 patients have episodes of QTc prolongation, regardless of the drugs they are taking.Despite this, based on the studies, mortality from the disease does not appear to be due to arrhythmogenic events.However, providing reliable guidelines is essential for managing patients who develop QTc prolongation during treatment.A conventional cut-off for discontinuing treatment with QT-prolonging drugs is a QTc ≥ 500 ms or a rise in QTc more than 60 ms.This strategy is widely popular among the studies that we reviewed, and it led to 4 episodes of TdP and 34 episodes of ventricular tachycardia/fibrillation among 8298 participants.The authors suggest that patients with other risk factors for QTc prolongation should have continuous cardiac monitoring.Furthermore, if the patient had any indications and the clinical status deteriorated, clinicians should discontinue the medications to protect the patient from the potentially fatal arrhythmias.

Netherlands
CONCLUSION
In conclusion, according to our systematic review and meta-analysis, a significant change in QTc interval following the use of hydroxychloroquine alone or in combination with azithromycin is highly expected that may be life-threatening.However, it should be noted that these changes may not be solely due to the toxicity of drugs.Interventional studies are required to confirm this hypothesis.
ARTICLE HIGHLIGHTS
Research background
Current evidence suggests that using hydroxychloroquine and azithromycin for coronavirus disease 2019 (COVID-19) increases the risk of cardiac arrhythmias.Previous studies reported that these drugs caused corrected QT (QTc) prolongation,leading to life-threatening conditions like torsades de pointes and sudden cardiac death.Although both in vivo and in vitro studies recommended the combination therapy of azithromycin and hydroxychloroquine, even as the first-line approach in preventing disease, it has also led to QTc prolongation.
Research motivation
In addition to cardiac monitoring, identifying patients, who are prone to side effects,helps to minimize the potential harms.By identifying susceptible individuals, it may be possible to use other drug protocols to maintain patient survival.
Research objectives
We summarize the findings about the prevalence and the risk of QTc prolongation in patients treated with hydroxychloroquine ± azithromycin.Also, we discuss the lifethreatening conditions in patients taking these medications.
Research methods
We comprehensively searched Medline, Web of Knowledge, Google Scholar, Scopus,and Cochrane Central Register of Controlled Trials databases until October 31, 2020 for all eligible studies under the considered keywords COVID-19, arrhythmia, QT interval, therapy, azithromycin, and hydroxychloroquine until.The study protocols were established in compliance with PRISMA-P guidelines.Outcome measures were QTc prolongation, cardiac arrhythmias, or sudden cardiac death.
Research results
Fifteen studies enrolling 8298 patients with targeted COVID-19 therapeutic regimes were included.The eligible studies found a significant increase in the mean QTc interval following treatment with the described medications compared to baseline QTc with weighted standard differences in means of 0.766.The pooled prevalence rate of QTc prolongation was estimated to be 9.2% (95%CI: 4.5% to 18.1%).
Research conclusions
Hydroxychloroquine ± azithromycin regimen can significantly increase the risk of developing QTc prolongation.
Research perspectives
According to our systematic review and meta-analysis, a significant change in QTc interval following the use of hydroxychloroquine alone or in combination with azithromycin is highly expected that may be life-threatening.However, it should be noted that these changes may not be solely due to the toxicity of drugs.Interventional studies are required to confirm this hypothesis.
ACKNOWLEDGEMENTS
We are indebted to Research Development Center of Sina Hospital for their technical help.We also thank Sherry Hughes Garne for editing this paper for proper English language, grammar, punctuation, spelling, and overall style.The authors are grateful to Mrs.Mahin Ahmadi Pishkuhi for statistical consultation and for evaluating the statistical methods and tests mentioned.
 World Journal of Meta-Analysis2021年6期
World Journal of Meta-Analysis2021年6期
- World Journal of Meta-Analysis的其它文章
- Simulating the mind and applications - a theory-based chance for understanding psychic transformations in somatic symptom disorders
- Is dose modification or discontinuation of nilotinib necessary in nilotinib-induced hyperbilirubinemia?
- Preclinical safety, effectiveness evaluation, and screening of functional bacteria for fecal microbiota transplantation based on germ-free animals
- Gastrointestinal tumors and infectious agents: A wide field to explore
- Newer developments in viral hepatitis: Looking beyond hepatotropic viruses
- Prediabetes and cardiovascular complications study: Highlights on gestational diabetes, self-management and primary health care