
结直肠黏液腺癌术后患者的预后影响因素分析
2021-01-19 13:19黄庆邹旻红蒋叶李旺林曹杰
新医学 2021年1期
关键词:结直肠癌
黄庆?邹旻红?蒋叶?李旺林?曹杰

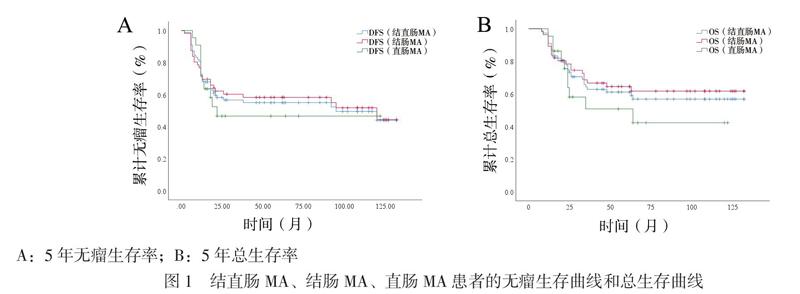
【摘要】目的 探讨结直肠黏液腺癌(MA)术后患者的预后影响因素。方法 收集结直肠MA根治性手术病例81例。使用Kaplan-Meier法分析无病生存期(DFS)和总生存期(OS),单因素和多因素Cox分析结直肠MA术后患者的预后影响因素。结果 结直肠MA、结肠MA、直肠MA的5年无瘤生存率分别是55%、57%和47%;5年总生存率分别为60%、62%和51%。单因素Cox分析发现T4(HR = 2.174)、N2(HR = 3.592)、TNM Ⅲ期(HR = 2.435)、糖类抗原199(CA199) ≥34 U/ml(HR = 3.330)为结直肠MA患者DFS的危险因素;手术时间> 200 min(HR = 2.594)、T4(HR = 2.465)、N2(HR = 5.413)、TNM Ⅲ期(HR = 3.275)、CA199≥34 U/ml(HR = 4.150)和癌胚抗原(CEA)≥5 ng/ml(HR = 2.636)为结直肠MA患者OS的危险因素。多因素Cox分析显示,N2和CA199 ≥34 U/ml是结直肠MA预后的危险因素,N2的DFS和OS的HR分别为2.763和4.113,CA199≥34 U/ml的DFS和OS的HR值分别为2.560和2.948。分层分析发现,N2(HR = 5.628)是結肠MA患者DFS的危险因素,N2(HR = 7.547)和CA199 ≥ 34 U/ml (HR = 2.947)是结肠MA患者OS的危险因素;行辅助化学治疗是直肠MA预后的保护因素,DFS和OS的HR值分别为0.063和0.182(P均< 0.05)。结论 N2分期、CA199≥34 U/ml是结直肠MA术后预后的独立危险因素,辅助化学治疗是直肠MA术后患者预后的保护因素。
【关键词】结直肠癌;黏液腺癌;预后;根治性手术
Analysis of prognostic factors in patients with colorectal mucinous adenocarcinoma after radical surgery Huang Qing, Zou Minhong, Jiang Ye, Li Wanglin, Cao Jie. Department of General Surgery, Guang-
zhou First Peoples Hospital, the Second Affiliated Hospital of South China University of Technology, Guangzhou 510180, China
Corresponding author, Cao Jie, E-mail: czhongt@ 126. com
【Abstract】Objective To explore the prognostic factors of patients with colorectal mucinous adenocarcinoma (MA) after radical surgery. Methods Eighty-one patients with colorectal MA undergoing radical surgery were recruited. Disease-free survival (DFS) and overall survival (OS) were analyzed using the Kaplan-Meier method. The prognostic factors of patients with colorectal MA were identified by using univariate and multivariate Coxs regression analyses. Results The 5-year DFS of colorectal MA, colonic MA and rectal MA were 55%, 57% and 47% respectively. The 5-year OS were 60%, 62%, 51%, respectively. Univariate Coxs regression analysis found that T4(HR = 2.174), N2(HR = 3.592), TNM stageⅢ(HR = 2.435), CA199≥34 U/ml(HR = 3.33) were the risk factors for DFS of patients with colorectal MA. The operation time > 200 minutes (HR = 2.594), T4 (HR = 2.465), N2 (HR = 5.413), TNM stage Ⅲ (HR = 3.275), CA199≥34 U/ml(HR = 4.150) and CEA≥5 ng/ml(HR = 2.636) were the risk factors for OS of colorectal MA patients. Multivariate Coxs regression analysis demonstrated that N2 and CA199 ≥ 34 U/ml were the risk factors for the prognosis of colorectal MA patients. The HR of DFS and OS for N2 were 2.763 and 4.113. The HR of DFS and OS for CA199≥ 34 U/ml were 2.560 and 2.948. Stratified analysis revealed that N2(HR = 5.628)was the risk factor for DFS of colonic MA. N2(HR = 7.547) and CA199 ≥ 34 U/ml (HR = 2.947) were risk factors for OS of colonic MA. Adjuvant chemotherapy was a protective factor for the prognosis of rectal MA patients, the HR of DFS and OS were 0.063 and 0.182 (both P < 0.05). Conclusions N2 stage and CA199≥34 U/ml are the risk factors for clinical prognosis of patients with colorectal MA. Adjuvant chemotherapy is a protective factor for clinical prognosis of patients with rectal MA.
四、结肠MA的预后影响因素分析
单因素Cox分析发现N2(HR = 5.628)、 TNM Ⅲ期(HR = 4.203)、CA199≥34 U/ml(HR = 3.300)是结肠MA患者DFS的危险因素(P均< 0.05);手术时间> 200 min(HR = 2.574)、N2(HR = 10.233)、TNM Ⅲ期(HR = 3.275)、CA199≥34 U/ml(HR = 4.650)和CEA≥5 ng/ml(HR = 2.844)是结肠MA患者OS的危险因素(P均< 0.05)。
多因素Cox分析发现N2[HR(95%CI)= 5.628(2.205 ~ 14.362)]是结肠MA患者DFS的危险因素;N2[HR(95%CI)= 7.547(2.083 ~ 27.347)]和CA199≥34 U/ml[HR(95%CI)= 2.947(1.177 ~ 7.380)]也是结肠MA患者OS的危险因素(P均< 0.05)。
五、直肠MA的预后影响因素分析
单因素和多因素Cox分析发现辅助化学治疗是直肠MA患者DFS和OS的保护因素,DFS和OS的HR (95%CI) 分别为0.063 (0.011 ~ 0.353)和0.182(0.050 ~ 0.663),P均< 0.05。
讨论
MA作为一种结直肠癌的特殊病理类型,占原发性结直肠癌的比例为5% ~ 15%,亚洲人群占比更低,通常为5%左右。MA与腺癌有诸多不同点,如趋于年轻化、近端好发、容易发生腹膜和远处转移、对化学治疗敏感性差,但目前治疗方法仍然按腺癌的治疗指南,因此结直肠MA的治疗仍然具有争议。有学者建议结直肠MA的治疗需单独考虑[3]。
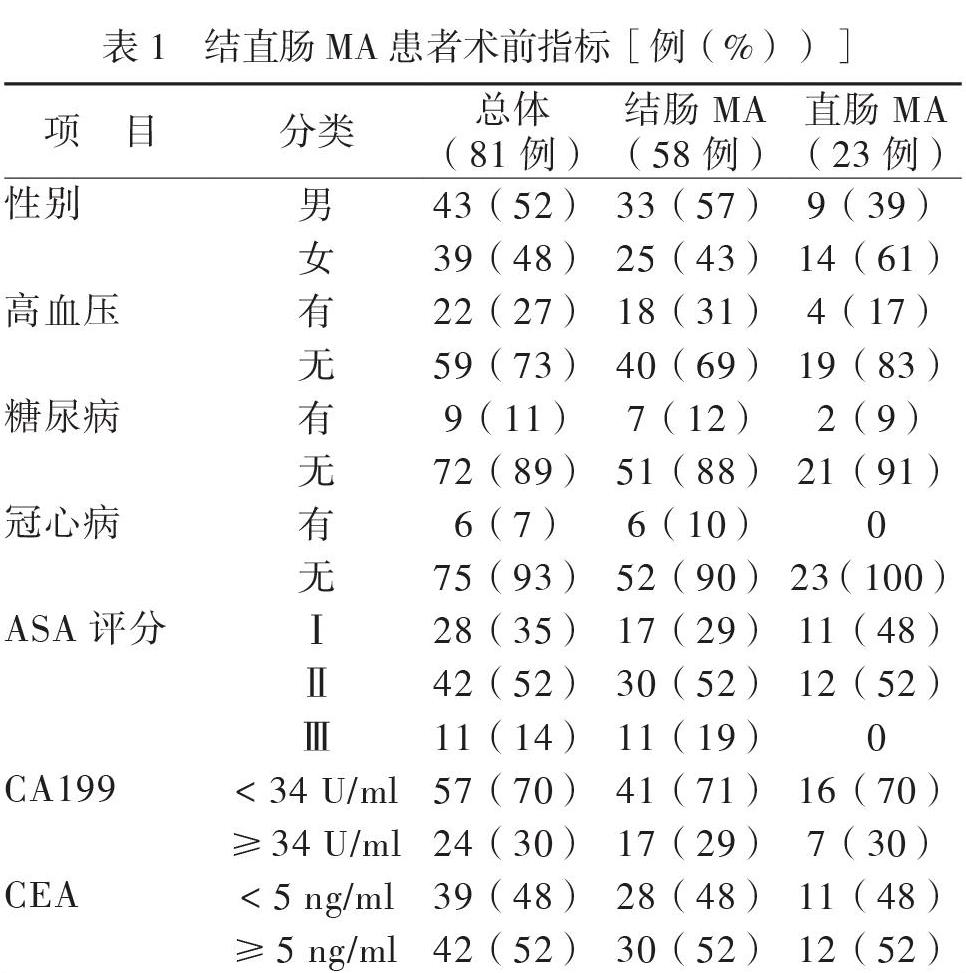
我们收集了2009至2018年广州市第一人民医院81例分期为Ⅰ ~ Ⅲ期的结直肠MA根治性手术患者,分析其预后影响因素,为MA的治疗和随访提供依据。我们发现结直肠MA在我院占比为5%,男女比例没有差异,右半结肠占比较高(42%),这与既往研究的结果相似[9]。我们还发现结直肠MA、结肠MA、直肠MA的5年无瘤生存率分别是55%、57%和47%;5年总生存率分别为60%、62%和51%。有研究显示MA的5年OS低于结直肠癌总体5年OS,据报道结直肠癌的5年OS是73.87%,明显高于我们结直肠MA的5年OS[10-11]。我们认为原因可能是结直肠MA的预后更差、我们收集的MA病理分期更高或其他方面等原因。
结直肠MA术后的预后影响因素很多,研究显示年龄和女性是MA预后的影响因素,术前高血压、糖尿病、冠心病病史对手术有一定影响,手术的质量决定患者恢复的情况[8]。而我们的研究显示年龄和性别并不影响结直肠MA的预后,既往病史(高血压、糖尿病、冠心病)也并未影响到结直肠MA的预后。
微创手术是结直肠外科发展的方向,目前腹腔镜手术已经成为结直肠癌治疗的标准,但单独研究MA腹腔镜治疗的文献较少。我们研究显示手术方式(腹腔镜和开放)不是结直肠MA的预后影响因素,提示腹腔镜治疗MA仍然具有优势。我们的研究显示出血量(> 100 ml)、术中输血并非结直肠MA的预后影响因素,但單因素分析显示手术时间(> 200 min)是结直肠MA的危险因素,我们分析了手术时间> 200 min的病例,发现其中绝大部分病例是肿瘤分期较高,特别是肿瘤局部侵犯较严重,导致手术时间延长,我们认为这可能是其中的混杂因素引起。有研究显示术后并发症是结直肠癌预后的危险因素,一方面术后并发症可能影响机体抵御癌症的免疫能力,另一方面术后并发症可能影响患者的化学治疗情况[12-13]。本研究显示术后并发症并未影响结直肠MA的预后。
结直肠癌的病理分期也会影响到结直肠癌预后,但本研究显示结直肠MA的T4、N2、TNM Ⅲ期是预后的危险因素。其中,N分期对预后影响更大,多因素分析显示N2是结直肠MA患者DFS和OS的独立危险因素。因此建议治疗结直肠MA患者,如果肿瘤分期高,在常规治疗后的随访密度应加强或者可尝试调整化学治疗方案(可加入靶向和免疫治疗)。术前CA199和CEA水平是结直肠癌术后的预后影响因素,对结直肠癌治疗和随访有重要参考作用[14-18]。CA199≥34 U/ml是结直肠MA的DFS危险因素,CA199≥34 U/ml和CEA≥5 ng/ml是结直肠MA患者OS的危险因素。多因素分析显示CA199≥34 U/ml是结直肠MA患者DFS和OS的独立危险因素。由于本研究中大部分CA199≥34 U/ml的患者,术前的CEA水平都高于10 ng/ml,可能术前CEA水平在比较高的水平才是结直肠MA预后的独立危险因素。这提示我们在治疗MA的时候仍然要注意患者术前的CEA和CA199水平,如果太高可以建议提高随访频率。
结直肠MA对化学治疗的敏感性仍然存在争议,研究显示晚期结直肠MA对化学治疗的敏感性更差,一方面可能是因为MA患者的微卫星不稳定的比率较高,影响其对化学治疗的反应[3, 19]。另一方面可能是因为MA高表达拓扑异构酶-1,导致其对氟尿嘧啶化学治疗不敏感。本研究中(部分病历未做微卫星不稳定检测)20%(6/30)的患者微卫星不稳定,微卫星不稳定患者比率较高。尽管有些学者提出MA对化学治疗的敏感性更差,但Hugen(2013年)提出辅助化学治疗对MA治疗意义重大,我们的研究结果也显示辅助化学治疗是直肠MA患者的保护因素,提示直肠MA患者可以从化学治疗中获益。因此,结直肠MA的辅助化学治疗仍然有必要。
我们的研究也存在不足,比如因为MA发病率低,获取研究样本较少;同时我们为回顾性研究,可能存在偏倚,希望未来有更大型的前瞻性研究,进一步规范结直肠MA治疗和随诊。
综上所述,N2分期、CA199 ≥34 U/ml是结直肠MA术后患者预后的独立危险因素,辅助化学治疗是直肠MA术后患者预后的保护因素。
参 考 文 献
[1] Arnold M, Sierra MS, Laversanne M, Soerjomataram I, Jemal A, Bray F. Global patterns and trends in colorectal cancer incidence and mortality. Gut,2017,66(4):683-691.
[2] Bosman FT. WHO classification of tumours of the digestive system. 4th Edition ed. Lyon: IARC Press,2010:134-146.
[3] Hugen N, Brown G, Glynne-Jones R, de Wilt JH, Nagtegaal ID. Advances in the care of patients with mucinous colorectal cancer. Nat Rev Clin Oncol,2016,13(6):361-369.
[4] Luo C, Cen S, Ding G, Wu W. Mucinous colorectal adeno-carcinoma: clinical pathology and treatment options. Cancer Commun (Lond),2019,39(1):13.
[5] Catalano V, Loupakis F, Graziano F, Torresi U, Bisonni R, Mari D, Fornaro L, Baldelli AM, Giordani P, Rossi D, Alessandroni P, Giustini L, Silva RR, Falcone A, DEmidio S, Fedeli SL. Mucinous histology predicts for poor response rate and overall survival of patients with colorectal cancer and treated with first-line oxaliplatin-and/or irinotecan-based chemotherapy. Br J Cancer,2009,100(6):881-887.
[6] Numata M, Shiozawa M, Watanabe T, Tamagawa H, Yama-moto N, Morinaga S, Watanabe K, Godai T, Oshima T, Fujii S, Kunisaki C, Rino Y, Masuda M, Akaike M. The clinicopathological features of colorectal mucinous adeno-carcinoma and a therapeutic strategy for the disease. World J Surg Oncol,2012,10:109.
[7] Li X, Sun K, Liao X, Gao H, Zhu H, Xu R. Colorectal carcinomas with mucinous differentiation are associated with high frequent mutation of KRAS or BRAF mutations, irrespective of quantity of mucinous component. BMC Cancer,2020,20(1):400.
[8] Emile SH, Magdy A, Elnahas W, Hamdy O, Abdelnaby M, Khafagy W. Predictors for local recurrence and distant metastasis of mucinous colorectal adenocarcinoma. Surgery,2018,1:S0039-6060(17)30879-6.
[9] Li C, Zheng H, Jia H, Huang D, Gu W, Cai S, Zhu J. Prognosis of three histological subtypes of colorectal adeno-carcinoma: A retrospective analysis of 8005 Chinese patients. Cancer Med,2019,8(7):3411-3419.
[10] Li ZP, Liu XY, Kao XM, Chen YT, Han SQ, Huang MX, Liu C, Tang XY, Chen YY, Xiang D, Huang YD, Lei ZJ, Chu XY. Clinicopathological characteristics and prognosis of colorectal mucinous adenocarcinoma and nonmucinous adenocarcinoma: a surveillance, epidemiology, and end results (SEER) population-based study. Ann Transl Med,2020,8(5):205.
[11] 周昌明,郭天安,莫淼,袁晶,沈潔,王泽洲,黄丹,朱骥,李心翔,蔡国响,徐烨,蔡三军,郑莹. 以大型单中心医院登记为基础的1.37万例结直肠癌手术患者生存报告. 中国癌症杂志,2020,30(4):246-253.
[12] Arnarson ?, Butt-Tuna S, Syk I. Postoperative complications following colonic resection for cancer are associated with impaired long-term survival. Colorectal Dis,2019,21(7):805-815.
[13] Aoyama T, Oba K, Honda M, Sadahiro S, Hamada C, Mayanagi S, Kanda M, Maeda H, Kashiwabara K, Sakamoto J, Saji S, Yoshikawa T. Impact of postoperative complications on the colorectal cancer survival and recurrence: analyses of pooled individual patients data from three large phase III randomized trials. Cancer Med,2017,6(7):1573-1580.
[14] Huh JW, Oh BR, Kim HR, Kim YJ. Preoperative carcin-oembryonic antigen level as an independent prognostic factor in potentially curative colon cancer. J Surg Oncol,2010,101(5):396-400.
[15] Becerra AZ, Probst CP, Tejani MA, Aquina CT, González MG, Hensley BJ, Noyes K, Monson JR, Fleming FJ. Evaluating the prognostic role of elevated preoperative carcinoembryonic antigen levels in colon cancer patients: results from the national cancer database. Ann Surg Oncol,2016,23(5):1554-1561.
[16] 黃利军,邵军,郑宗珩. 术后术前CEA比值对术前CEA升高结直肠癌患者预后评估的价值. 新医学,2018,49(12):873-877.
[17] 陈蕾,姜北海,邸佳柏,张成海,王早早,张楠,邢加迪,崔明,杨宏,姚震旦,苏向前. 术前检测癌胚抗原和糖链抗原199对结直肠癌Ⅱ~Ⅲ期患者预后的判断价值. 中华胃肠外科杂志,2015,18(9):914-919.
[18] Sisik A, Kaya M, Bas G, Basak F, Alimoglu O. CEA and CA 19-9 are still valuable markers for the prognosis of colorectal and gastric cancer patients. Asian Pac J Cancer Prev,2013,14(7):4289-4294.
[19] Maisano R, Azzarello D, Maisano M, Mafodda A, Bottari M, Egitto G, Nardi M. Mucinous histology of colon cancer predicts poor outcomes with FOLFOX regimen in metastatic colon cancer. J Chemother,2012,24(4):212-216.
(收稿日期:2020-10-12)
(本文编辑:杨江瑜)
猜你喜欢
现代仪器与医疗(2016年6期)2017-01-12
中国民族民间医药·上半月(2016年11期)2016-12-26
上海医药(2016年23期)2016-12-22
上海医药(2016年23期)2016-12-22
中国现代医生(2016年27期)2016-12-21
中国实用医药(2016年28期)2016-12-07
中国实用医药(2016年27期)2016-11-30
中国实用医药(2016年27期)2016-11-30
医学信息(2016年29期)2016-11-28
上海医药(2016年14期)2016-08-10
