
Guiding extension catheter facilitated percutaneous coronary intervention for a dextrocardia patient with acute left anterior descending artery occlusion: a case report
2021-01-05 02:14JingNANShuaiMENGYaLiTIANTongZHANGRuiWANGShaoBinWEIZeNingJIN
Journal of Geriatric Cardiology 2020年12期
Jing NAN, Shuai MENG, Ya-Li TIAN, Tong ZHANG, Rui WANG, Shao-Bin WEI, Ze-Ning JIN,3,#
1Department of Cardiology and Macrovascular Disease, Beijing Tiantan Hospital, Capital Medical University, Beijing, China
2Tiantan Neuroimaging Center of Excellence, Beijing Tiantan Hospital, Capital Medical University, Beijing, China
3Department of Cardiology, Beijing Anzhen Hospital, Capital Medical University, Beijing, China
Keywords: Dextrocardia; Guiding extension catheter; Percutaneous coronary intervention
Dextrocardia refers to a right-sided location of the heart within the thoracic cavity which is the primary manifestation of the abnormal lateralisation of the embryonic leftright axis.[1]As a rare cardiac malformation, the prevalence rate of dextrocardia is between 1/6000 to 1/35000 live births.[2]It is reported that the incidence rate of coronary artery disease for dextrocardia patients is similar for patients without dextrocardia.However, the detailed information including electrocardiogram (ECG) manifestation and percutaneous coronary intervention (PCI) technique for dextrocardia patients is still limited.[3,4]Herein, we report a dextrocardia patient who was diagnosed by modified ECG and treated by trans-radial PCI facilitated with guiding extension catheter (GEC).
A 64-year-old male who was known to have dextrocardia since his childhood presented to the chest pain clinic complaining intermittent chest pain for one day.The chest pain was located in the right side of chest and radiated to his right arm.Standard ECG as well as modified ECG were performed immediately.The standard ECG showed positive P waves presented in leads I and aVR as well as significant S waves in all precordial leads.A modified ECG (left and right arm electrodes were reverse and pericardial leads were placed in the right chest) revealed a sinus rhythm (normal P wave) and ST-segment depression as well as T wave inversion in pericardial leads (Figure 1).The patient was diagnosed with acute non-ST-segment elevation myocardial infarction due to the elevation of cardiac enzymes.The patient was treated with aspirin, β-blocker, clopidogrel and low-molecular weight heparin during hospitalization.Coronary angiography via the right radial artery was performed the next day, which showed acute total occlusion of left anterior descending artery (LAD) and mild-moderate stenosis in left circumflex artery and right coronary artery.The PCI was then performed via the right radial artery.We finally succeeded engaging Judking Left (JL, Medtronic, Inc,USA) 4 guiding catheter after we failed to engage with JL 3.5 and Extra Backup (EBU, Medtronic, Inc, USA) 3.5 guiding catheters.After advancing the guidewire (Sion, Ashahi,Inc, Japan) to the distal segment of LAD, we pre-dialated the occlusion lesion with a semi-compliant balloon 2.5 mm ×15 mm (Emerge, Boston Scientific, Inc, USA) at 8–12 atm.We met difficulty when we tried to deliver the stents because mother guiding catheter did not provide sufficient backup support.A GEC (Expressman, APT medical, China) was then applied to facilitate the delivery of three stents (Resolute Integrety, Medtronic, Inc, USA: 2.25 mm × 22 mm,2.75 mm × 30 mm, 3.0 mm × 30 mm) to the target lesion.The final result was satisfied after we post-dialated the stents with non-compliant balloons (Quantum, Boston Scientific, Inc,USA: 2.5 mm × 15 mm, 3.0 mm × 15 mm, 3.5 mm × 15 mm)at 12–18 atm (Figure 2).The patient was discharged on stable condition two days after the procedure.
Dextrocardia is defined as a cardiac position that is a mirror image of normal anatomy.[5]Both the diagnose from ECG manifestation and PCI treatment information in patients with dextrocardia is challenging for dextrocardia patients.[6,7]
The typical manifestations of dextrocardia patients in standard 12-lead ECG include right axis deviation in QRS complex, negative QRS complex and inverted P and T waves in lead I, reversed QRS complexes in leads aVR and aVL, and positive R wave in lead aVR.[8]Modified ECG wherein the left lead is placed on the right arm, the right arm lead is placed on the left arm, and the V1 through V6 leads are placed in the V2, V1, and V3R through V6R positionscan provide correct ECG information for dextrocardia patients.[9–11]
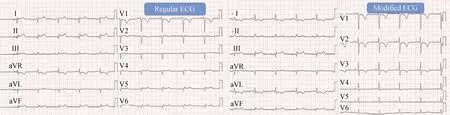
Figure 1.Regular and modified ECG manifestation of this dextrocardia patient on admission.ECG: electrocardiogram.
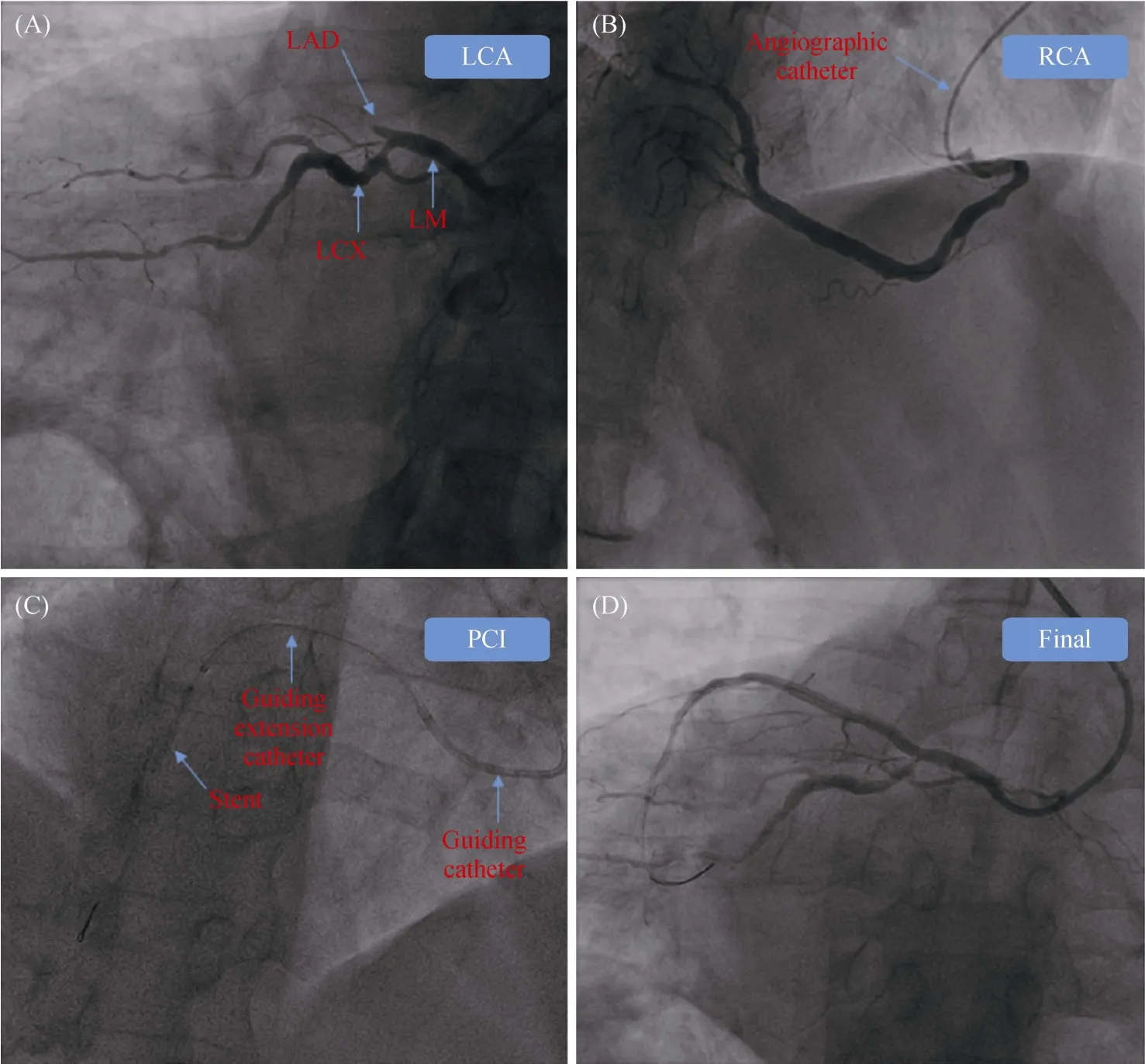
Figure 2.Coronary angiography and PCI.(A): Angiographic result of LCA; (B): angiographic result of RCA; (C): guiding extension catheter facilitated stent delivery; and (D): final result of LCA.LAD: left anterior descending artery; LCA: left coronary artery; LCX: left circumflex artery; LM: left main; PCI: percutaneous coronary intervention; RCA: right coronary artery.
Transradial PCI, as the most common used PCI strategy in patients with acute myocardial infarction (AMI), is challenging in dextrocardia patients.[12]It was until 2007 that the first case of transradial PCI was reported in dextrocardia patient.[13]After that, transradial PCI in dextrocardia patients were acknowledged and applied in patients with triple vessel disease, left main disease, AMI or event chronic total occlusion lesion.[14–17]
Many studies had described the unexpected difficulties which might be encountered during the PCI procedure in dextrocardia patients.[14–17,18]There are a few technical considerations during PCI in dextrocardia patients that we should pay attention to.Firstly, counter-directional torque of the catheter is instrumental in successful coronary engagement.[19]This technique was successfully employed in our procedure.Secondly, right-left mirror-images of traditional angiographic view angles facilitate recognition and navigation of the unusual arterial anatomies.[13]Thirdly, left radial approachor transfemoral approach should be considered in selective patients.[20,21]Fourthly, wider curve of guiding catheter such as EBU 3.75 or EBU 4 and specialized guiding catheters should be considered.[22]Last but not least, GEC is a useful equipment which could provide better backup support when the mother guiding catheter could not provide sufficient backup support.[23]
So far as we know, there was no previous report on the facilitation of GEC during transradial PCI in dextrocardia patients.GEC, as a widely-used facilitation equipment, has been demonstrated to be efficacy in complex PCI procedures by improving the co-axial and enhancing the backup support.[24–26]In this article, we reported a successful transradial PCI for dextrocardia patient with the help of GEC,which might provide useful experience in future clinical practice.
Acknowledgments
This study was supported by the Chinese Cardiovascular Association-V.G.(2017-CCA-VG-042).All authors had no conflicts of interest to disclose.
 Journal of Geriatric Cardiology2020年12期
Journal of Geriatric Cardiology2020年12期
- Journal of Geriatric Cardiology的其它文章
- Advances in Journal of Geriatric Cardiology over the course of a decade
- Catheter ablation for atrial fibrillation is associated with reduced risk of mortality in the elderly: a prospective cohort study and propensity score analysis
- Effects of angiotensin-converting enzyme inhibitor and angiotensin II receptor blocker on one-year outcomes of patients with atrial fibrillation: insights from a multicenter registry study in China
- Parity and carotid atherosclerosis in elderly Chinese women
- Validation of methods for effective orifice area measurement of prosthetic valves by two-dimensional and Doppler echocardiography following transcatheter self-expanding aortic valve implantation
- Venous thromboembolism prophylaxis-prescribing patterns among elderly medical patients in a Saudi tertiary care center: success or failure?