
Catheter ablation for atrial fibrillation is associated with reduced risk of mortality in the elderly: a prospective cohort study and propensity score analysis
2021-01-05 02:14XinSUXinDUShangXinLUChaoJIANGJingDUShiJunXIAZhaoJieDONGZhaoXuJIADeYongLONGCaiHuaSANGRiBoTANGNianLIUSongNanLIRongBAIJianZengDONGChangShengMA
Journal of Geriatric Cardiology 2020年12期
Xin SU, Xin DU,2,3,#, Shang-Xin LU, Chao JIANG, Jing DU, Shi-Jun XIA, Zhao-Jie DONG,Zhao-Xu JIA, De-Yong LONG, Cai-Hua SANG, Ri-Bo TANG, Nian LIU, Song-Nan LI, Rong BAI,Jian-Zeng DONG, Chang-Sheng MA,#
1Department of Cardiology, Beijing Anzhen Hospital, Capital Medical University, National Clinical Research Centre for Cardiovascular Diseases, Beijing, China
2Heart Health Research Center, Beijing, China
3The George Institute for Global Health, Faculty of Medicine, University of New South Wales, Sydney, Australia
4Beijing Centre for Disease Prevention and Control, Beijing, China
Abstract Background It is unclear whether catheter ablation (CA) for atrial fibrillation (AF) affects the long-term prognosis in the elderly.This study aims to evaluate the relationship between CA and long-term outcomes in elderly patients with AF.Methods Patients more than 75 years old with non-valvular AF were prospectively enrolled between August 2011 and December 2017 in the Chinese Atrial Fibrillation Registry Study.Participants who underwent CA at baseline were propensity score matched (1:1) with those who did not receive CA.The outcome events included all-cause mortality, cardiovascular mortality, stroke/transient ischemic attack (TIA), and cardiovascular hospitalization.Results Overall, this cohort included 571 ablated patients and 571 non-ablated patients with similar characteristics on 18 dimensions.During a mean follow-up of 39.75 ± 19.98 months (minimum six months), 24 patients died in the ablation group, compared with 60 deaths in the non-ablation group [hazard ratio (HR) = 0.49, 95% confidence interval (CI): 0.30–0.79, P = 0.0024].Besides, 6 ablated and 29 non-ablated subjects died of cardiovascular disease (HR = 0.25, 95% CI: 0.11–0.61, P = 0.0022).A total of 27 ablated and 40 non-ablated patients suffered stroke/TIA (HR = 0.79, 95% CI: 0.48–1.28, P = 0.3431).In addition, 140 ablated and 194 non-ablated participants suffered cardiovascular hospitalization (HR = 0.84, 95% CI: 0.67–1.04, P = 0.1084).Subgroup analyses according to gender, type of AF, time since onset of AF, and anticoagulants exposure in initiation did not show significant heterogeneity.Conclusions In elderly patients with AF, CA may be associated with a lower incidence of all-cause and cardiovascular mortality.
Keywords: Atrial fibrillation; Catheter ablation; Mortality; Stroke; The elderly
1 Introduction
Atrial fibrillation (AF) is the most common arrhythmia.[1,2]The incidence of AF increases with age.[3,4]Based on the predicted life expectancy, the incidence of AF is expected to double in the next 50 years.[5]Elderly patients with AF are more likely to have comorbidities, including hypertension, diabetes mellitus (DM), heart failure (HF), and renal failure, placing them at increased risk for cardiovascular events and mortality.[6,7]In addition, the effect of antiarrhythmic drugs is less predictable in aging population with more frequent side effects.[8]
At present, catheter ablation (CA) has proven to be an efficacious method to treat symptomatic AF.[9]CA could reduce AF burden, improve exercise capacity, and ameliorate AF-related symptoms.[10–12]Meanwhile, increasing studies found that CA for AF in elderly subjects was efficacious,and major complications might be more frequent in the elderly.[13–18]However, few studies have evaluated the association between CA and long-term prognosis in elderly patients with AF.The objective of the current study was to access the association between CA and long-term outcomes [allcause mortality, cardiovascular mortality, stroke/transient ischemic attack (TIA), and cardiovascular hospitalization]in elderly patients with AF.
2 Methods
2.1 Study population
The Chinese Atrial Fibrillation (China-AF) Registry is a prospective, multicenter, hospital-based, ongoing registry study of patients diagnosed with AF in Beijing, China.We have described the details of the cohort earlier.[19]All subjects enrolled in the current study were identified from the China-AF database.Data collected between August 2011 and December 2017 were used for analyses.Eligible participants were ≥ 75 years old, with a documented AF confirmed by 12-lead electrocardiogram (ECG) or 24-hour Holter monitoring within the past six months.Exclusion criteria were as follows: follow-up of less than six months; previous ablation for AF; patients diagnosed with rheumatic mitral stenosis or having mitral valve prostheses; and data missing.Then, the subjects were divided into two groups: the ablation group and non-ablation group.The flowchart of patient selection was presented in Figure 1.
The research was approved by the Ethics Committee of Beijing Anzhen Hospital (D11110700300000) and participants were required to provide written consent in this study.
2.2 Data collection
Information on patient characteristics, including age,gender, body mass index (BMI), type of AF, time since onset of AF, insurance, education, smoking, drinking, comorbidities (DM, hypertension, HF, stroke/TIA, vascular disease,and prior bleeding), medication (rhythm/rate control drugs and anticoagulants), left ventricular ejection fraction, as well as CHA2DS2-VASc score, was collected when patients were enrolled.
2.3 Catheter ablation for atrial fibrillation
The CA strategy used in participating centers has been previously described, namely, pulmonary vein isolation for paroxysmal AF, and three additional linear ablations at the left atrial roof, cavotricuspid isthmus and mitral isthmus for persistent AF.[20]
2.4 Medical therapy and anticoagulation management
For patients in the ablation group, warfarin or a kind of non-vitamin K antagonist oral anticoagulants (NOACs) was given to all the patients for at least three months after CA.A kind of I or III antiarrhythmic drugs would be prescribed for the eligible patients after ablation for three months.Thereafter, the choice of continuing anticoagulants and antiarrhythmic drugs was left to the physician’s discretion.Besides, for individuals in the non-ablation group, anticoagulation treatment was recommended when the CHA2DS2-VASc score was ≥ 2, and antiarrhythmic therapy for AF was at the treating physician’s discretion.
2.5 Follow-up
Each enrolled patient was followed up at three and six months and then every six months, via telephone interviews or at outpatient clinics.During each follow-up, we collected information on drug treatments, arrhythmia symptoms,clinical outcomes and results of ECG and 24-hour Holtermonitoring.Additional 24-hour Holter monitoring or ECG was performed if arrhythmic symptoms occurred.
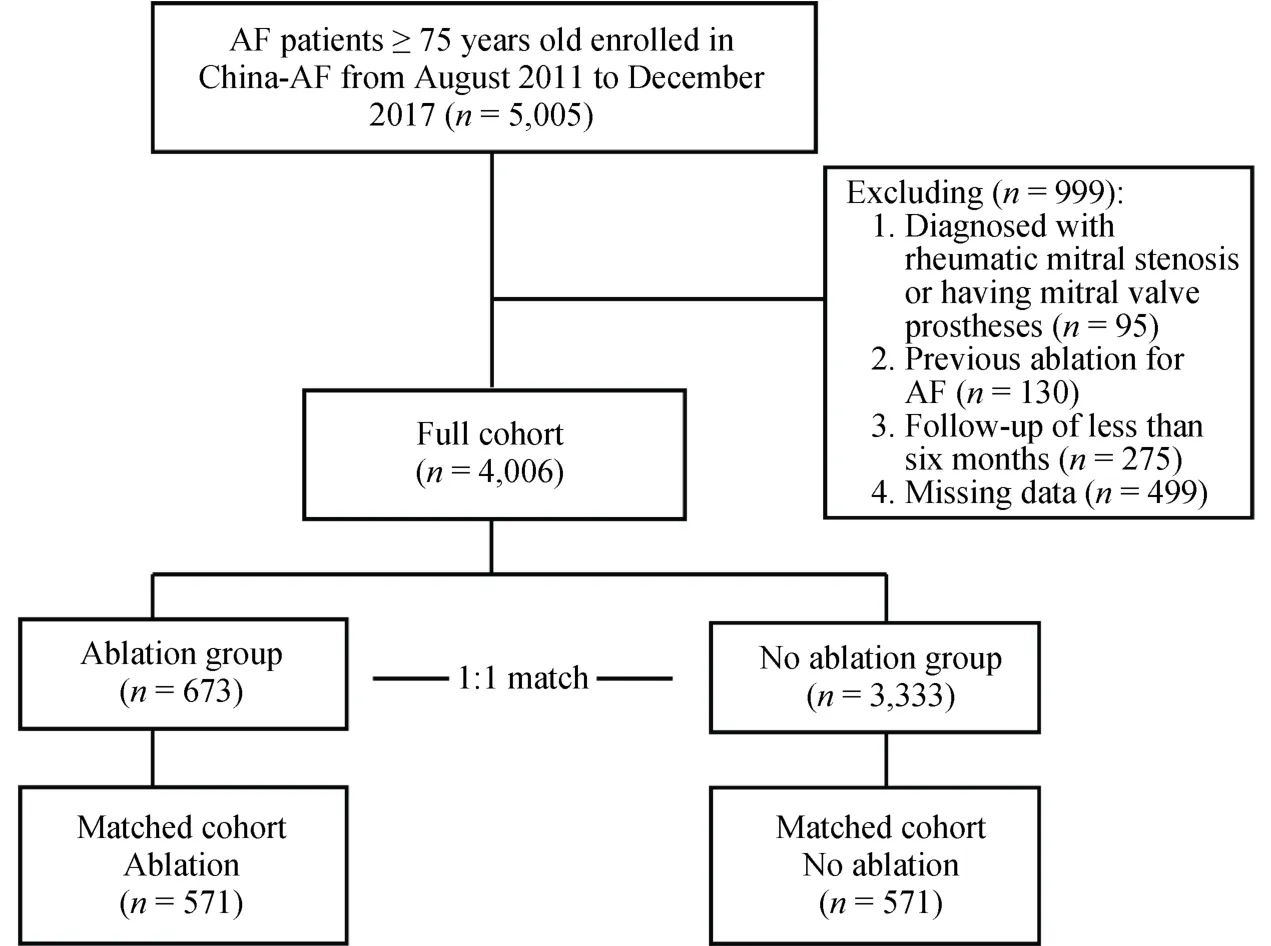
Figure 1.Study flowchart.AF: atrial fibrillation.
2.6 Definition of outcomes
The primary outcome was time to all-cause mortality and the secondary outcome was time to cardiovascular mortality,stroke/TIA or cardiovascular hospitalization.In this study,participants were followed up from the date of enrollment until loss of follow-up, first outcome event, or December 31, 2017.
Atrial tachyarrhythmia (AT) episode was defined as recorded AT/atrial flutter/AF ≥ 30 seconds by 12-lead ECG or 24-hour Holter monitoring.Successful CA was defined as no onset of AT episode ≥ 30 seconds beyond three months blanking period.
2.7 Statistical analysis
To eliminate the influence of selection bias in the assessment of therapeutic effect, baseline differences were adjusted by propensity score matching.The propensity score matching was based on 18 demographic and clinical variables, including age, gender, BMI, type of AF, time since onset of AF, insurance, education, smoking, drinking, hypertension, HF, DM, ischemic stroke/TIA/peripheral thromboembolism, vascular disease, prior bleeding, rhythm/rate control drugs, anticoagulants, and CHA2DS2-VASc score.Subjects in the two groups were matched in a 1:1 ratio with the caliper width of 0.1.No replacements were used.
Continuous variables were presented as mean ± SD,whereas categorical variables were shown as numbers and proportions.Continuous variables were compared using the one-way ANOVA analysis, whereas categorical variables were compared using theχ2test.Cumulative incidence rates were estimated by Kaplan-Meier method, and statistical significance was examined using the log-rank test.Cox regression analysis was used to calculate the hazard ratio (HR)and 95% confidence interval (CI) of outcomes and to assess the association between outcomes and CA.Subgroup analyses were conducted stratified by gender, type of AF,time since onset of AF, and anticoagulants exposure in initiation.In the sensitivity analyses, multivariate Cox regression models were further used to estimate the association between CA and all-cause and cardiovascular mortality.A two-sidedP-value < 0.05 was considered statistically significant.All statistical analyses were conducted by using SAS 9.4 (SAS Institute, Cary, NC, USA).
3 Results
3.1 Study population
From August 2011 to December 2017, 5,005 AF patients more than 75 years old were enrolled in the China-AF registry cohort.We identified 673 patients receiving CA and 3,333 patients as controls after excluding 95 subjects diagnosed with rheumatic mitral stenosis, 130 subjects receiving ablation before enrolled in this cohort, 275 subjects with follow-up time less than six months and 499 subjects with data missing.Finally, 571 ablated and 571 non-ablated subjects at baseline were selected based on the propensity score matching (Figure 1).
3.2 Baseline characteristics
The baseline characteristics of the two groups were illustrated in Table 1.Before matching, subjects in the ablation group were younger, mostly male, with lower BMI, a higher proportion of paroxysmal AF, well educated, and well health insurance coverage.Patients in the ablation group were less likely to have a history of congestive HF, ischemic stroke/TIA/peripheral thromboembolism, and vascular disease.Besides, subjects receiving CA were more likely to use anticoagulants (92.12%vs.39.12%,P< 0.0001).After propensity score matching, the differences between the two groups were balanced.
In this matched cohort, one-year adherence rates of the ablation and non-ablation groups were 92.03% and 94.71%,respectively.The mean number of ablations in the ablation group was 1.07 ± 0.26 per patient.
3.3 All-cause mortality
During a mean follow-up of 39.75 ± 19.98 months, 24 patients died in the ablation group (incidence rate: 1.71 per 100 person-years), and 60 patients died in the non-ablation group (incidence rate: 3.65 per 100 person-years).The cumulative incidence of mortality was lower in the ablation group than in the non-ablation group (log-rankP= 0.0024).CA was associated with a 51% lower risk of all-cause mortality (HR = 0.49, 95% CI: 0.30–0.79) (Figure 2A).
3.4 Cardiovascular mortality
Of the propensity score-matched cohort, 6 subjects died of cardiovascular disease in the ablation group (incidence rate: 0.42 per 100 person-years), and 29 subjects died of cardiovascular disease in the non-ablation group (incidence rate: 1.75 per 100 person-years).CA was associated with a lower risk of cardiovascular mortality (HR = 0.25, 95% CI:0.11–0.61) (Figure 2B).
3.5 Stroke/TIA
During the follow-up, 27 patients receiving CA developed stroke/TIA (incidence rate: 1.96 per 100 person-years),and 40 patients receiving medical therapy developed stroke/TIA (incidence rate: 2.48 per 100 person-years).There was no statistically significant difference in the cumulative incidence of stroke/TIA between the ablation group and the non-ablation group (log-rankP= 0.3431), and HR for stroke/TIA was 0.79 (95% CI: 0.48–1.28) in the ablation group compared with the non-ablation group (Figure 2C).

Table 1.Baseline characteristics of AF patients (≥ 75 years old) with and without ablation before and after propensity score matching.
3.6 Cardiovascular hospitalization
Of the propensity score-matched cohort, 140 subjects developed cardiovascular hospitalization in the ablation group (incidence rate: 11.25 per 100 person-years), and 194 subjects developed cardiovascular hospitalization in the non-ablation group (incidence rate: 13.72 per 100 person-years).There was no statistically significant difference in the cumulative incidence of cardiovascular hospitalization between ablation group and non-ablation group (log-rankP= 0.1084), and HR for cardiovascular hospitalization was 0.84 (95% CI: 0.67–1.04) in the ablation group compared with the non-ablation group (Figure 2D).
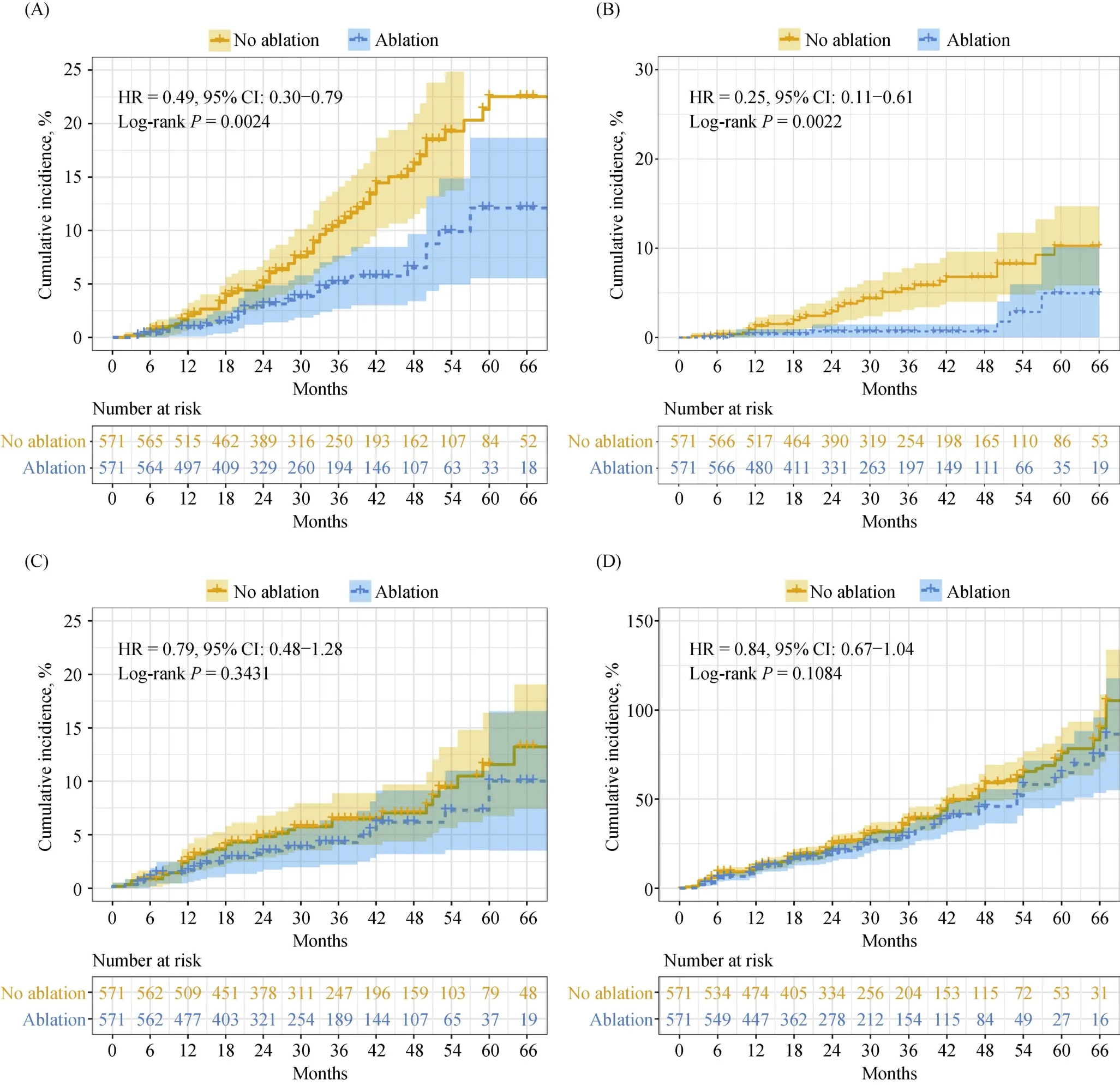
Figure 2.The cumulative incidence of outcomes concerning atrial fibrillation ablation.(A): All-cause mortality; (B): cardiovascular mortality; (C): stroke/transient cerebral ischemia; and (D): cardiovascular hospitalization.HR: hazards ratio.
3.7 AT episode and anticoagulants use during each follow-up interval
The proportions of patients with AT episodes during each follow-up interval were shown in Figure 3A.In addition, during the follow-up, 341 patients (59.7%) in the ablation group remained AF-free, and 97 subjects (17.0%) in the non-ablation group remained AF-free.Ablation was associated with a 42% lower risk of AT recurrence (HR = 0.58,95% CI: 0.49–0.68,P< 0.0001).The proportions of patients receiving anticoagulation therapy during each follow-up interval were illustrated in Figure 3B.The proportions of anticoagulants use in the ablation group were lower than those in the matched group.
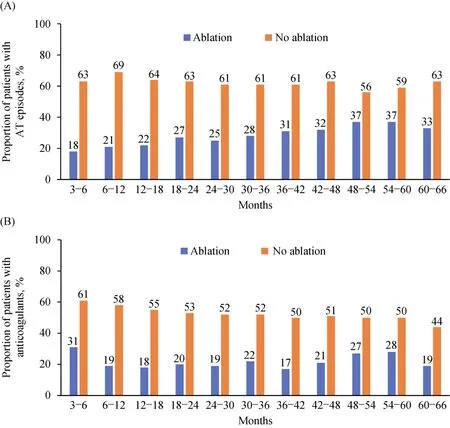
Figure 3.Proportion of AT episodes (A) and anticoagulants exposure (B) during follow-up intervals.AT: atrial tachyarrhythmia.
3.8 Periprocedural complications
During the periprocedural period, stroke occurred in 2 patients, acute cardiac tamponade in 7 patients, groin hematomas in 4 patients, pseudoaneurysm in 4 patients, and arteriovenous fistula in 2 patients.No other periprocedural complications such as atrioesophageal fistula, pulmonary vein stenosis, major bleeding, or death were observed in the ablation group.
3.9 Subgroup analyses
The subgroup analyses, according to gender, type of AF,time since onset of AF, and anticoagulants exposure in initiation were shown in Figure 4.The results did not show significant heterogeneity in analyses of the subgroups, with one exception.The effect of CA on cardiovascular hospitalization differed by type of AF (Pinteraction-value = 0.0177).Cardiovascular mortality was not analyzed in subgroups due to fewer events.
3.10 Sensitivity analyses
In this matched cohort, we further conducted regression analyses of factors associated with all-cause and cardiovascular mortality.Age, congestive HF, hypertension, DM, stroke/TIA, vascular disease, and prior bleeding were controlled in the analyses of all-cause and cardiovascular mortality.In multivariate Cox regression analyses, ablation remained statistically associated with a lower risk of all-cause mortality(HR = 0.49, 95% CI: 0.30–0.78) and cardiovascular mortality (HR = 0.25, 95% CI: 0.10–0.59) (supplemental material, Table 1S & Table 2S).
4 Discussion
Our main finding in the prospective observational study was that ablated elderly patients with AF had a lower risk of all-cause and cardiovascular mortality than non-ablated elderly patients.Besides, we did not find a statistical difference between propensity-matched groups in the rate of stroke/TIA and cardiovascular hospitalization.Furthermore, subgroup analyses demonstrated that the risk of all-cause mortality was not affected by gender, type of AF, time since onset of AF, and anticoagulants exposure in initiation.
AF is an arrhythmia with an increased prevalence in the elderly.[3,4]Meanwhile, AF is associated with an increased risk of HF,[21]loss of cognitive functions,[22]and AF-related cerebrovascular accidents,[23]all of which tend to be more devastating and debilitating in elderly patients.At present,
CA has been proved to be an efficacious method for AF patients.[9]The beneficial effects of CA on maintaining sinus rhythm and improving quality of life were already confirmed,[10,11]whereas the association between CA and longterm benefits was controversial.Most of patients in large trials of CA for AF were young people, and there were few data on CA for AF in elderly patients.Considering the high incidence of AF in the elderly, more attention should be paid to AF ablation in the elderly.
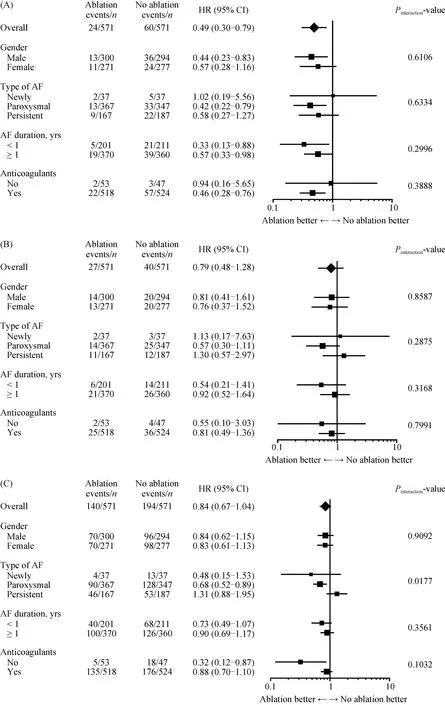
Figure 4.Risk of the all-cause mortality (A), stroke/transient ischemic attack (B) and cardiovascular hospitalization (C) in clinically relevant subgroups.AF: atrial fibrillation; HR: hazards ratio.
So far, some published studies have revealed that AF ablation was efficacious in the elderly.[13–18]Overall, most of these studies have shown similar clinical success rates between the younger and older groups, and major complications might be more frequent in the elderly.However, few observational studies reported in the literature have assessed the long-term benefits of CA in the elderly.Hence, studies focusing on the long-term effect of CA for AF in the elderly are needed.In this study, we prospectively enrolled the AF patients more than 75 years old, collected data purposely,used the propensity score matching, and accessed the relationship between CA and long-term outcomes in elderly patients with AF.
Previous observational studies in the general population have compared outcomes between subjects who received CA and those who did not, and the outcomes were conflicting.[24–27]CABANA randomized trial showed the strategy of CA did not significantly reduce the composite endpoint of death, disabling stroke, serious bleeding, or cardiac arrest compared to medical therapy among AF patients.[28]However, the lower-than-expected event rates and treatment crossovers in this trial affected the treatment effect of ablation.Thus, whether CA for AF prolongs survival remains obscure.Considering that the majority of participants in previous observational studies were younger, it is unclear whether elderly patients with AF can benefit from CA.The present study showed a strong association between ablation and survival in elderly patients with AF (HR = 0.49, 95% CI:0.30–0.79).In line with our findings, Nademanee,et al.[29]compared CA with antiarrhythmic drugs in AF patients (age≥ 75 years old) and found that elderly patients with AF benefited from CA, which was associated with lower mortality risk (annual mortality rate 4% in catheter group and 9.8% in non-ablation group).However, this study compared crude rates and included a limited number of individuals(261 ablated and 63 pharmacologically treated elderly patients with AF).Theoretically, the mortality risk was reduced by multiple factors, including prevented worsening of HF,restoration of sinus rhythm, and reduced AF burden.[1,30]
Elderly patients with AF have a higher risk of stroke.[31]The risk of stroke in patients with AF is strongly influenced by several demographic and clinical factors, including age,sex, HF, hypertension, DM, prior stroke or TIA, and vascular disease.[32]Anticoagulant therapy was an effective therapy to prevent AF patients from suffering strokes.[33]Meanwhile,among elderly patients with AF, anticoagulants were consistently associated with a lower risk of stroke and positive net clinical benefit, with the highest benefit in elderly patients treated with warfarin who achieved therapeutic range≥ 60% or high dose of NOACs.[34,35]Our previous study found that the proportion of AF patients receiving anticoagulants was only 37.5%, 32.7%, and 25.4% for patients with CHADS2≥ 2, 1, and 0, respectively.[36]In recent years,with the popularization of NOACs and the improvement of doctors’ awareness of prescribing anticoagulants, the overall rate of anticoagulants initiation was increasing.In the present study, 90.72% of patients in the ablation group and 91.77% of patients in the non-ablation group were treated with anticoagulants after propensity score-matched.Therefore, it was not surprising that the risk of stroke/TIA was not significantly reduced in this study.
It has been demonstrated that AF patients were at higher risk of hospitalization.An analysis from ROCKET AF showed that the hospitalization rate was 10.2 per 100 personyears of follow-up in AF subjects, and cardiovascular causes contributed nearly a half.[37]Mitral regurgitation was aggravated, atrial systolic function was lost and left ventricular systolic dysfunction occurred in AF patients.Therefore,elimination of AF with CA may improve HF symptoms and reduce cardiovascular hospital admissions associated with AF.[38,39]Recently, some randomized trials explored the effect of CA on hospitalization in AF patients with HF and noted that the hospitalization rate of patients undergoing CA was significantly lower than that of the medical treatment group.[12,40,41]However, there was limited evidence for assessing the relationship between CA for AF and cardiovascular hospitalization in elderly patients.In the present study,we found that CA for AF did not reduce cardiovascular hospitalization in elderly patients compared with medical therapy.It might be that elderly patients suffer from multiple cardiovascular diseases simultaneously, and cardiovascular hospitalization not caused by AF increased in elderly patients.Because we didn’t collect the causes of cardiovascular hospitalization, the effect of ablation on HF in elderly patients with AF remained unknown.
4.1 Limitations
This study has several limitations.Firstly, although the propensity score matching was used to ensure the consistency of baseline data between the two groups, there maystill be some residual bias due to unmeasured covariates.Secondly, among 571 subjects assigned to the medical treatment group, 48 patients (8.41%) underwent CA during the follow-up period, and intention-to-treat analysis was used in this study.Thirdly, CA techniques and medical treatments may have changed during the long-term study,which may affect the outcomes.Last but not least, because our research is an observational study, it could not determine a causal relationship.
4.2 Conclusions
In elderly patients with AF, CA may be associated with a lower incidence of mortality and does not statistically reduce the risk of stroke/TIA and cardiovascular hospitalization.Therefore, CA may be the preferred treatment for elderly patients with symptomatic and drug-refractory AF.
Acknowledgments
This study was supported by the National Key Research and Development Program of China (2017YFC0908803 &2018YFC1312501 & 2016YFC0900901 & 2016YFC1301002& 2020YFC2004803).All authors had no conflicts of interest to disclose.The authors gratefully acknowledge the China-AF investigators for assistance in the data collection.
 Journal of Geriatric Cardiology2020年12期
Journal of Geriatric Cardiology2020年12期
- Journal of Geriatric Cardiology的其它文章
- Advances in Journal of Geriatric Cardiology over the course of a decade
- Effects of angiotensin-converting enzyme inhibitor and angiotensin II receptor blocker on one-year outcomes of patients with atrial fibrillation: insights from a multicenter registry study in China
- Parity and carotid atherosclerosis in elderly Chinese women
- Validation of methods for effective orifice area measurement of prosthetic valves by two-dimensional and Doppler echocardiography following transcatheter self-expanding aortic valve implantation
- Venous thromboembolism prophylaxis-prescribing patterns among elderly medical patients in a Saudi tertiary care center: success or failure?
- Can sacubitril/valsartan become the promising drug to delay the progression of chronic kidney disease?