
Prioritization of factors related to mental health of women during an earthquake: A qualitative study
2019-06-17 12:33:42RaheleSamoueiShahinShooshtariMasudBahramiMohammadRezaAbediMohammadRezaMaracy
Rahele Samouei, Shahin Shooshtari, Masud Bahrami, Mohammad Reza Abedi, Mohammad Reza Maracy
1 Social Determinants of Health Research Center, Isfahan University of Medical Sciences, Isfahan, Iran
2 Student Research Committee, Isfahan University of Medical Sciences, Isfahan, Iran
3 Department of Community Health Sciences, Rady Faculty of Health Sciences, University of Manitoba, Winnipeg,Manitoba, Canada
4 Nursing and Midwifery Care Research Center, Faculty of Nursing and Midwifery, Isfahan University of Medical Sciences,Isfahan, Iran
5 Department of Counseling, Faculty of Education and Psychology, University of Isfahan, Isfahan, Iran
6 Department of Epidemiology and Biostatistics, Environment Research Center, Research Institute for Primordial Prevention of Non-communicable Disease, School of Public Health, Isfahan University of Medical Sciences, Isfahan, Iran
KEY WORDS: Mental health; Women; Earthquake; Qualitative study
INTRODUCTION
Disasters are events from the outcomes of which no one in the world is safe. Survivors of disasters experience a wide range of psychological responses with varying degrees of impact.[1]According to the results of a study, women account for the highest rate of victims of disasters with mental health problems.[2]Although health-related findings have highlighted the need for considering psychological issues in natural disasters, this issue has been underestimated.[3,4]
Women are more vulnerable in disasters compared to men due to some genetic, psychological, physiological,legal, and social factors.[5]A study[6]conducted through 33 qualitative interviews with disaster experts in Iran referred to the biological, social, and psychological dimensions of women’s vulnerability to disasters.Moreover, another study on the earthquake in East Azarbaijan Province, Iran, pointed to severe poverty and violence.[7]In a study on the earthquake in Lorestan Province, Iran, which was performed using a focus group discussion (FGD), it was concluded that women encountered socioeconomic needs, loss of assets,insecurity, and fertility problems.[8]A qualitative study carried out through consultation with scholars,highlighted issues including basic living and security needs, social and status development, access to facilities and values, awareness of rights, and participation in policy-making and the community for women in disasters.[9]In a group discussion with 35 experts in a qualitative study, issues like water, shelter, security,respect, suitable communication, awareness, and employment were introduced as the requirements of earthquake survivors.[10]Furthermore, in a study on 4 groups of women participating in Red Crescent public organizations, clothing, hygiene, conditions of pregnancy and lactation periods, cosmetic and hygienic needs,psychological variables, and domestic violence control were reported as the requirements of women during disasters.[11]Two separate studies in the Nepal earthquake and East Azarbaijan earthquake in Iran referred to the menstrual period and fertility health needs, and cultural limitations of women in disaster situations.[12,13]In an investigation on mental health requirements in the Sri Lanka earthquake, the new national mental health policy and a proposal for a mental health regulation were stressed.[14]In a study implemented on women exposed to the tsunami in India, psychosocial care was introduced as an important and effective mental health strategy for women at risk of disasters.[15]In a study on 1,253 women exposed to earthquakes, it was proposed that social relationships protect women’s mental health from damages due to earthquake.[16]In addition, another study introduced factors including the management of physical,psychological, and emotional outcomes, fertility, and environmental health as important factors in this f ield.[17]
In Jang et al[18]study, 165 Nepali women aged 18-59 years were assessed about the psychological aspects of earthquake using Patient Health Questionnaire-15 (PHQ-15). The results showed that earthquake increased the rate of diseases, as well as life non-satisfaction, and decreased religious belief among the women. Lack of knowledge about the access to emergency services, low literacy and income, and deficiency of mental health cares and social affairs tended to post-traumatic stress disorder (PTSD). Sezgin and Punamäki studied 195 women aged 15-65 years who were residents in an earthquake-affected town in South Eastern Turkey. They found that relocation was associated with mental health problems, especially with intrusive PTSD, somatization,and hostility symptoms, and interpersonal problems among the women.[19]
Reviewing f indings of previous studies, it was found that most of the studies have addressed the mental health problems and vulnerability of disaster survivors, and few studies have discussed and prioritized the requirements related to mental health, in particular in women. Studies conducted in Iran in this area have reported limited results,[20-22]while health promotion and prevention of its related problems can be implemented through identifying the factors related to mental health and prioritizing these factors. The measurement of these factors and responding to them generally include extensive and costly programs,and prioritization is required given the limited available resources. In this field, no studies, specifically studies in Iran, have been conducted on the prioritization of the psychological needs of women in disasters. To be able to prioritize the needs, it was necessary to know experts’ viewpoints and reach to consensus of experts(group consensus), so we used Delphi method. This method brought us the possibility to receive viewpoints of homogeneous but independent experts in a large geographic area. Considering the opportunity to comment freely and to revise the viewpoints during different rounds of Delphi method, it is expected to reach a more desirable prioritization.
In addition, the literature has not comprehensively highlighted the relevant content, especially culture-based content, needed in this area. Therefore, the present study was designed in a qualitative manner to provide a deeper response to the research question regarding prioritizing factors related to mental health in disasters by producing and explaining the related content based on the views of experts.
METHODS
This study was conducted using the Delphi method in medical universities, the Ministry of Health,Treatment, and Medical Education, Deputy Health and Medical Center, Welfare Organization, and Red Crescent Organization in Tehran, Isfahan, Ahvaz,and Tabriz Provinces, Iran, in 2017. The participants included experts in the f ields of psychology, counseling,psychiatry, social medicine, and health management with experience and knowledge in disasters, especially earthquakes. They were selected using purposive and snowball sampling methods. The validity of the Delphi method in the above-mentioned studies was based on the scientif ic validity of participants rather than their number.Moreover, there was no definite scope for determining the sample size in the Delphi method in the resources.Hence, based on a general agreement, the sample size was determined to be at least 10 individuals,[23]and the number of participants was 20 at this stage of the study.However, in the f irst and second stages of Delphi, 20 and 19 individuals responded to the Delphi method.
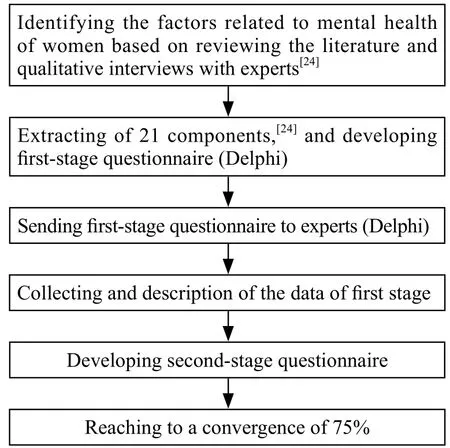
Figure 1. The stages of study based on the Delphi method.
The data in this study were obtained using the modified Delphi method.[23]This study was derived from a PhD dissertation and was part of a larger study;the results of the previous study were used as data in the present study.[24]In addition, the factors, which were obtained through semi-structured interviews with experts and using scientific literature, related to the mental health of women in the previous study were used for prioritization in this study (Figure 1). Moreover, the Delphi questionnaire was adjusted based on the concepts,components and sub-components obtained from the interview results. Therefore, the modif ied Delphi method was used; 21 components were extracted in the areas of genetic behavior, hormonal and sexual behavior,group relationships and support in emergency situations,fair treatment in the provision of women’s rights and services, the dignity and position of women in situations of harm, the role and responsibilities of women in crisis, social security in disasters, injurious behaviors in disastrous situations, policy setting in accordance with the status of women in disasters, the establishment and implementation of fair rules for women, the governing culture in the disaster area, relationship of spirituality and disaster, of psychological well-being training,psychological well-being through the treatment of mental disorders, nutrition and physical activity in disasters,awareness of high-risk behavioral habits, health-related behaviors in disasters, crisis awareness and behavior management in diff icult situations, gaining of skills and experiences, climatic elements in the area of damage,and regional environmental design in the Likert range.These factors were obtained based on the classification of similar codes in more abstract classes. In addition,2 evaluators examined the classification to assess the validity of the tool, then corrective actions were applied in a collective agreement. After identifying the 21 classes, the form was designed in such a way that the respondent was able to delete the item, create a new item,and prioritize existing items in terms of numbering. In front of each item in the questionnaire, 3 columns were considered, including the ability to execute, importance,and effectiveness, which could be scored based on a Likert scale ranging from 1 to 5. In one sentence at the bottom of the page, it was stated that if the respondents intended to delete or add a clause, they could express their suggestion in the last column in the section of considerations.
After completing the necessary coordination and expressing the purpose of the study, the questionnaires were sent to the invited subjects accompanying the instructions and response guidelines, and the conditions and manner of return. Reminder messages were sent regularly via email, and repeated and repeated to get the answer. It was followed up to ensure that they responded within 2 weeks. It took a total of 1 month to collect the questionnaires. In the letter sent with the questionnaire to the respondents, while appreciating the time they assigned to completing the questionnaire, the purpose of the study and the response instructions were presented to them. Moreover, information was provided on the rate of performing the method, the time and manner of returning, and also the importance of the study. The number of times required to reach the consensus of respondents was considered with a 75% convergence.[23]
In this study, since the components were previously extracted through interviews with the relevant experts and knowledgeable individuals, their validity was confirmed. However, the developed form was shared with 3 associated professors and editing corrections were applied. In addition, 2 questionnaires were primarily completed, and given that no specific corrective comments were proposed, their data were considered in the study. In the extraction of data, consensus was considered to be above 75%. Thus, if the collective agreement of the participants was less than 50%, the desired item would be eliminated. A poll was held on the agreement rate of between 50% and 75% along with the new proposed components in the next round and the agreement rate of 75% or higher was accepted as the final component. Data were analyzed using descriptive statistics including rate, percentage, mean, standard deviation (SD), and median in the SPSS software(version 21, IBM Corporation, Armonk, NY, USA).
The participants signed the agreement; however, they were informed that they could withdraw from the study.The results of the questionnaires were not exploited for personal goals and the individual information of the respondents remained confidential. In addition,the process of recording information was performed without bias and judgment of the researcher to the extent possible.
RESULTS
Table 1 shows the demographic characteristics of experts participated in this study.
Findings based on the views of experts on the prioritization of the factors related to mental health of women during an earthquake related to the second phase of implementation of the Delphi method have been reported in Tables 2 and 3.
The results presented in Table 2 demonstrate the descriptive statistics of indicators of applicability,significance, and effectiveness of each group of factors related to mental health of women during an earthquake;these factors were ranked by the experts. The first 3priorities in terms of views of the experts based on the mean scores included psychological well-being, group relationships and support in emergency situations, and fair treatment in the provision of rights and services to women with mean values of 13.4, 13.1, and 12.7,respectively.

Table 1. Demographic characteristics of experts (n=19)
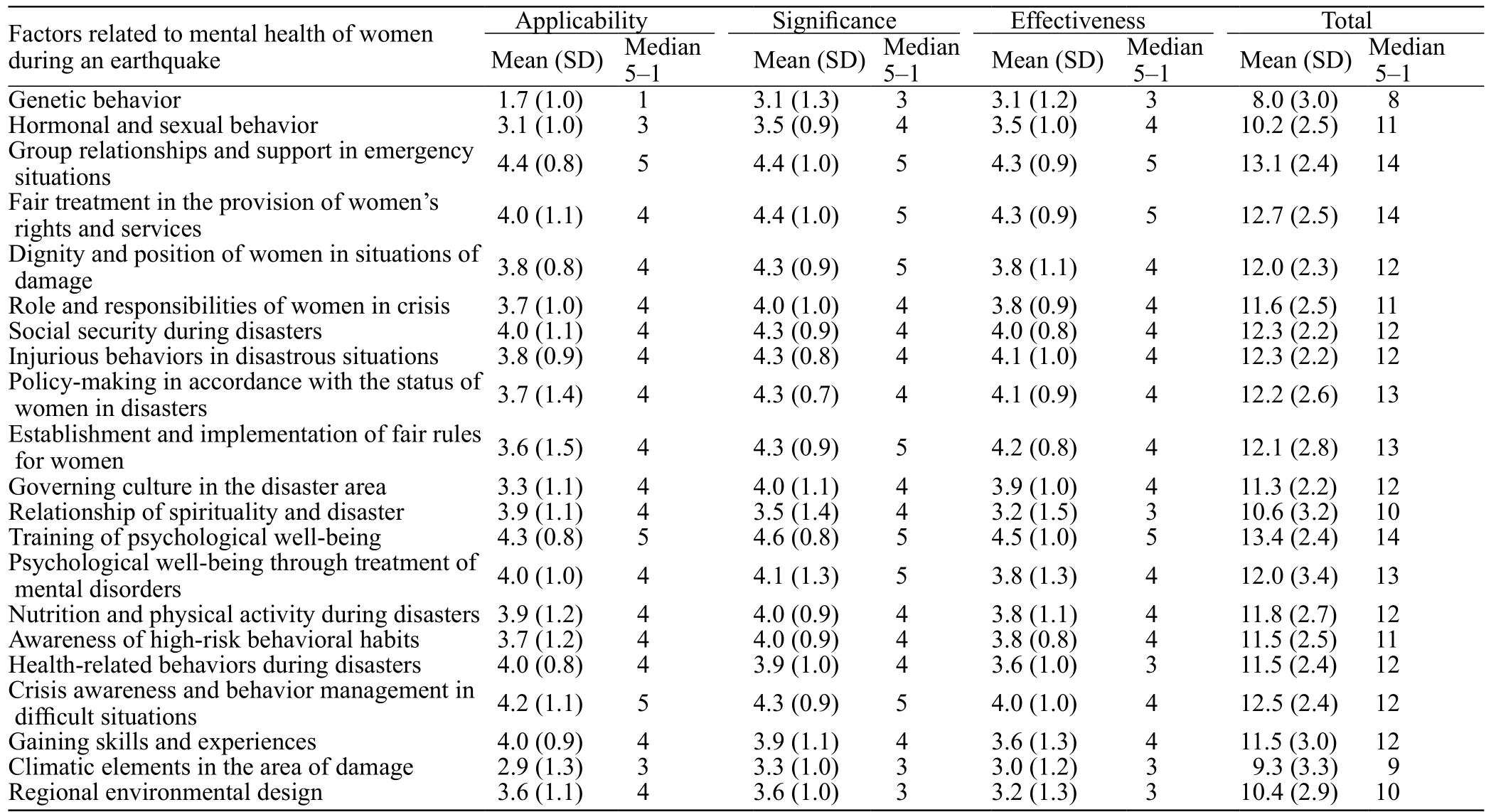
Table 2. Prioritizing factors related to mental health of women during an earthquake in terms of the views of experts based on descriptive statistics in the Delphi method (n=19)
The results presented in Table 3 indicate that in the second stage of the Delphi method, two groups of factors, including genetic behavior and climatic elements in the damage region, could not achieve the minimum conditions for obtaining the criteria of above 75%agreement of the experts. Therefore, they were not taken into account in the present study. Moreover, the highest percentage of agreement was related to factors like psychological well-being training.
DISCUSSION
In the process of prioritizing factors related to the mental health of women in disasters, it was revealed that experts did not achieve consensus on two categories of factors in terms of the priority in planning regarding women. These factors included genetic behavior, and climatic elements in the damage region. Some subsets of genetic behaviors included genetic potential for stress and disorder, shorter neural connections, and the more vulnerable physiology of women. In addition, in the issue of the climatic elements in the damage region,some cases like sunlight, humidity, temperature, healthy weather, use of shade in the temporary accommodation area, water stream in the area, impact of climate on neuroscience, and stench of dead bodies were reported.
According to the views of experts, the 3 most important factors in terms of mean scores were psychological wellbeing training (stress management in crisis, decisionmaking skills in urgent circumstances, empathy toward other survivors, adaptation to disaster, resilience, ability to communicate, and management of emotions), group relationships and support in emergencies (helping groups,friendly communication, access to social networks,engagement with authorities, communication with close relatives and families who have survived the incident,and women’s organization), and fair treatment in the provision of women’s rights and services (the second sex look at women in aid situations, fair distribution of goods during the incident, allocation of private goods to women, special care, the need for rescuers and female physicians).
Psychological well-being training lies in the field of psychology. This training empowers individuals both individually and mentally, and helps them manage their emotions, feelings, thoughts, and behaviors. In addition, as a result of this training they can present the best response in emergencies. The experts agreed that the empowerment of women itself is the foremost necessity. The results of some studies in this regard have been consistent with the results of the present study. For instance, it has been declared in a study that empowering women psychologically leads to better coping with disasters and less vulnerability.[21]Furthermore, studies have shown that paying attention to women’s mental health improvement is one of their most important requirements during disasters.[14,15,24]The experts then prioritized some social dimensions that were specific to and suitable for women and recommended for them;the fact that women naturally need more social groupsupport and show a more suitable performance in friendly and familiar relationships and groups. It has been illustrated in studies that social relationships protect women’s mental health from earthquake damage.[15,16]From the psychological point of view, the presence of women in the community and formations leads to a better discharge of negative emotions, a better understanding of positive excitement, and sympathy and gaining support and empathy, which can have a positive effect on improving mental health. Moreover, as a result of stating the importance of attending the community, these studies highlighted the need for the establishment of social justice. Furthermore, given the fact that the factors related to the mental health of women were different due to their specific gender characteristics, they had to be considered in a specific, non-discriminatory, and nonbelittling manner. The experiences of many rescuers and women themselves involved in the disaster indicate gender supremacy, neglect, lack of attention to specific needs, and lack of support and attention. The results of a study conf irmed that at times of disasters women were not treated fairly and that the distribution of goods was not fair. In addition, women rescuers must be considered for women.[10,11]
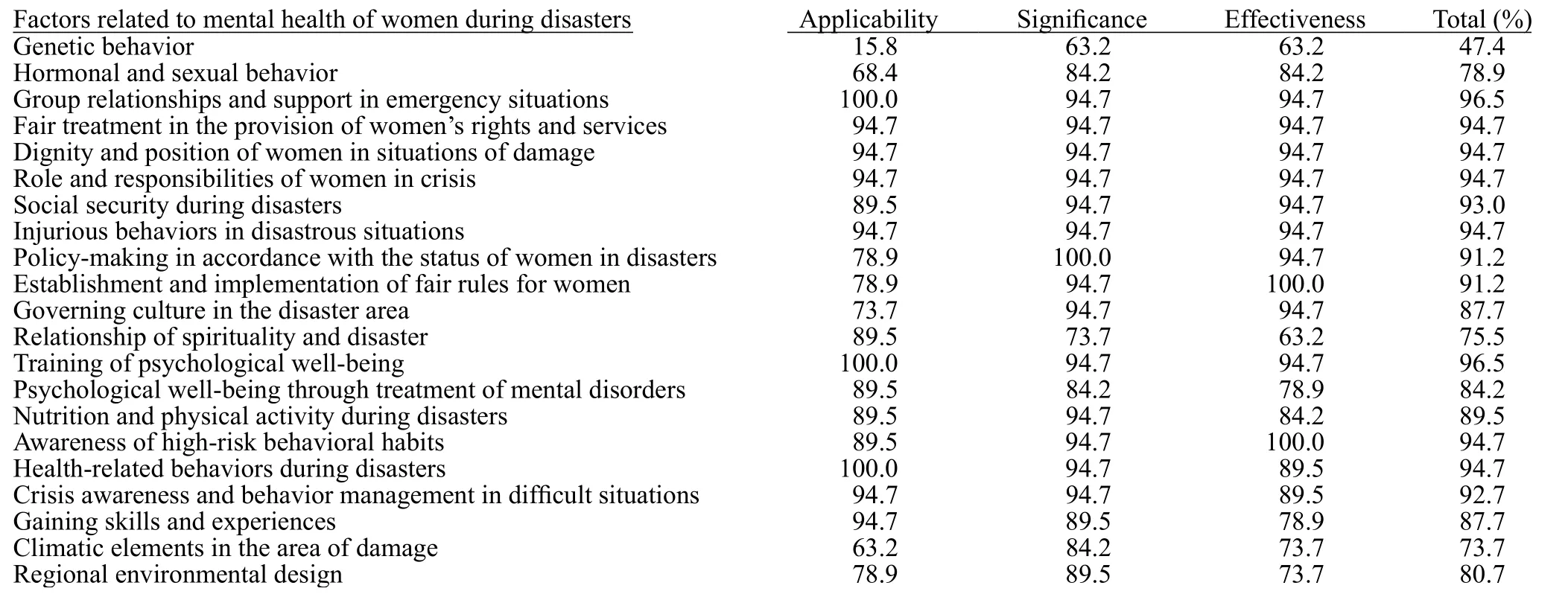
Table 3. Percentage of agreement of experts to prioritize factors related to mental health of women during an earthquake in the Delphi method(n=19)
After the first 3 priorities, the next 5 factors were identif ied as important priorities in identifying the factors related to mental health of women during disasters,which included awareness of crisis and management of adverse behavior and circumstances (identification of safe places, awareness of observance of safety tips,dealing with emergency conditions, self-management in crisis, emergency decision-making, petition for help during disasters, logical behavioral stability during disasters, and getting help), social security during disasters (privacy, safe environment [bath, toilet, and temporary accommodation], secure relationships,integrity of family and relatives, sending reliable individuals into the women’s population, monitoring the behavior of the individuals sent into the women’s population), harmful behaviors during disastrous situations (violence against women, social stigma,exploitation of unprotected or single women, helping women with expectations, and threats against protest),policy-making appropriate to the status of women during disasters (development of mental health policies for injured women, transparent policies in relation to women, accepting women’s participation in policies,and policymakers’ awareness of the requirements of injured women), and establishment and implementation of fair rules for women (correct implementation of rules, women’s participation in legislation, presence of women in disaster-related organizations, provision of supportive laws for injured women, insurance specific to women before the events). One of the important factors stressed in this section was the preservation of security in various psychological, behavioral, spatial,and situational aspects. During disasters, the situation is generally disorderly and unstable; so that, compared to other conditions, there is a higher possibility of abuse,violence, helping and expecting something in return,threats, and etc. In this regard, some studies have pointed out that security in housing and privacy for women are very urgent during disaster situations,[8,10,11,25]and that women are more vulnerable to violence and harmful behaviors under these circumstances.[7,11,13]Accordingly,women who have not acquired suff icient skills to respond to these conditions or who live in societies where they are seen as the second sex and have no supportive laws and a system of follow-up of their rights, are basically in a weak position and surrender to the undesirable conditions. In this regard, the importance of the establishment of specif ic policies and laws for preserving the mental health of women has been emphasized in studies.[5,9,14,26]
Other factors that were in the next degree of importance, however with very little degree of difference to the previous ones, included psychological well-being through treatment of mental disorders (treatment of mental disorders including anxiety, depression, PTSD,fear of injury, shock, imagination of death and disaster,tendency toward self-harm, suicidal thoughts), dignity and position of women in situations of harm (social value of women in disasters, key role of women in the damaged family, role of women as levers in events,maternity role, the spouse role, women’s participation in society), nutrition and physical activities during disasters (healthy nutrition, nutritional problems in crisis, preservation of food for emergencies, women’s nutrition in certain physical conditions, suitable activities in less-equipped places, exercising in limited conditions, appropriate physical activities for physical damages), role and responsibilities of women in crisis(lack of abuse of women in multiple responsibilities,suitable attention to the simultaneous spouse-mother role of women, inconsistency between women’s efforts and the outcomes, suitable participation of women in constructional development, overburden in difficult conditions), health-seeking behaviors during disasters(body care under damage conditions, making health claims, awareness of observance of health issues, feeling responsible for their own health and that of others, access to health services in special circumstances), awareness of high-risk behavioral habits (smoking, alcohol use under stress, risky sexual behaviors, drug abuse, coping with unsuitable behavioral habits in crisis), learning skills and gaining experiences (familiarity with incomegenerating jobs, training applied skills like tailoring,driving, building, swimming, carpet weaving, making handicrafts, dairying, and etc., self-help, learning how to provide for the family as a householder), and governing culture in the disaster area (respect for the culture of the region, cultural adaptation of the injured and helpers, cultural constraints of women, consideration of cultural indicators of women of the area when providing assistance, lack of priority of rescuing women due to the governing culture).
Treatment of mental disorders was considered when expressing some of the factors, which, despite its necessity and importance, was considered after training and acquisition of skills due to the higher importance of prevention relative to treatment. In this regard,researchers[4,15]emphasized that the management of stress, anxiety, and depression should be the priority of preventative programs for women during disasters.Moreover, observance of a healthy lifestyle like nutrition, sleep, exercise, health information search behavior, hygiene, and many similar cases can result in the improved mental health and physical ability.This result was consistent with studies on women who had experienced an earthquake.[21,24]In general, since a significant disturbance occurs in all social, cultural,and family systems in a disaster, self-empowerment,self-mastery, and experiences can be useful at least at one stage or time to be timely exploited by the women themselves or be offered in a coherent cultural context. This case was confirmed in other studies.[11,21,24]Furthermore, the experiences of various rescuers,especially in the area of mental health, indicated that the lack awareness of the culture of the damaged region complicated the relief efforts and sometimes caused misunderstandings with irreparable consequences. In this regard, in a crisis situation in which the region is out of equilibrium and balance, the lack of attention to cultural differences and cultural considerations can create special sensitivity and serious problems. Cultural attributes including the need to respect women’s culture,considerations about their clothing, observance of restrictions in any culture, and the later rescue of women compared to men in cultural views were shown in some studies.[11,24]
Finally, the respondents achieved agreement on 3 groups, however, with a lower priority, which included relationship between spirituality and disasters (attention to the religious context of the injured women, religious superstitions governing the region, training of the clergy for disasters, feeling of being punished in disasters,hindering of support for women due to discrimination),regional-environmental design (use of color variety in the environment, green space, flowers and plants,suitable temporary accommodation, and determination of places suitable for the distribution of food, baths, and toilets), and hormonal and sexual behavior (hormonal problems in emergencies, menopause, menstruation,anemia, women’s specif ic physiological needs, women’s illnesses, and higher probability of incidence of sexually transmitted diseases [STDs]).
In the area of spiritual and religious dimensions,considering the components which have been mixed with a sense of punishment and prejudice and could inf luence mental health in case of being unduly used, these factors were placed in the next rank. Some respondents declared that the regional-environmental design played an effective role in improving mental health. However,since the objective of the present study was to prioritize the requirements, other issues directly related to psychological and mental health were considered as the more prominent priorities. According to the search performed, very few studies have addressed these factors.In two studies, the importance of the design and layout of temporary accommodation and the need for taking into account the required locations have been pointed out.[11,24]Hormonal and sexual behaviors play a significant role in women’s mental status. However, due to the fact that these behaviors were related to the physical condition and the mechanism of the natural physiology of women,they were not largely highlighted by the respondents.Hormonal issues including pregnancy, lactation, iron deficiency, bleeding, and etc. have been mentioned in some studies.[11-13,17,24]According to the findings of the present study, there have been some advantages and restrictions regarding the implementation of the study including, respectively, the relatively comprehensive look at the factors related to mental health of women during disasters and limited number of experts in the subject who agreed to cooperate; as a signif icant number of experts (43 participants) were interviewed during the first part of the study to determine the factors related to women mental health, and we decided that the expert participated in Delphi stage be different and affected by the information of previous stage.
CONCLUSION
According to the findings of this study, the most important factors related to women’s mental health were psychological training and social support in terms of solidarity and communication, and in particular, the fair and equitable consideration of women in the community,which accounted for the highest priorities according to the viewpoints of the experts. The results of this study can be applied by the policy-makers in the mental health of women, legislators for the rights of women, health care authorities, therapists and service providers in this area, managers, specialists and rescuers during the disasters and incidents, and women themselves and the society which they interact with.
Suggestions
According to the type of factors related to the mental health of women, which were prioritized by the respondents, the need to empower women through practical training and skill training is emphasized in the f irst level. In addition, the recommendations went beyond the psychological dimension and spread to the sociocultural dimensions. Accordingly, a society requires the reviewing of women’s social rights for a progressive and successful improvement of the mental health of women.Hence, this society can efficiently handle women’s mental health needs, especially in situations of injury and disaster, considering the supports provided.
ACKNOWLEDGEMENT
We would like to thank all participants whose opinions helped us reach the goals of our study.
Funding: The study was not supported.
Ethical approval:The study was cleared and approved by the research ethics committee at Isfahan University of Medical Sciences.
Conflicts of interest:The authors declared no conflicts of interests.
Contributors:All authors contributed in designing the study,analyzing the results and editing the paper.
 World journal of emergency medicine2019年3期
World journal of emergency medicine2019年3期
- World journal of emergency medicine的其它文章
- Instructions for Authors
- Retroperitoneal hematoma following common iliac artery injury in a child
- Benef its of using an endotracheal tube introducer as an adjunct to a Macintosh laryngoscope for endotracheal intubation performed by inexperienced doctors during mechanical CPR: A randomized prospective crossover study
- Are radiological modalities really necessary for the long-term follow-up of patients having blunt solid organ injuries? A single center study
- A comparison of simulation versus didactics for teaching ultrasound to Swiss medical students
- Clinical characteristics of patients with Haff disease after eating crayf ish