
Adult Congenital Heart Disease in the Veteran Population: A Case-Based Report
2019-05-11 06:02:02RobertHamburgerDOMPHFACC
Robert F.Hamburger, DO, MPH, FACC
1 Division of Cardiovascular Medicine, University of Florida College of Medicine, Gainesville, FL 32608, USA
2 Malcom Randall VA Medical Center, Gainesville, FL 32608, USA
Abstract
Keywords: congenital heart disease; atrial septal defect; anomalous venous return; sinus venosus defect; cor triatriatum; transposition of great arteries
Introduction
Simple forms of congenital heart disease such as small ventricular septal defects and secundum atrial septal defects (ASDs) often go undiagnosed in the pediatric population and appear later in life, many times found incidentally on imaging studies.However,because of advancements in the care of patients with congenital heart disease, even those with complex anatomy are living well into adulthood.It is estimated that 90% of children with severe congenital heart disease will survive to the age of 18 years [1].For this reason, it is important for all cardiologists to have a solid foundation of the basic pathophysiology and management of congenital heart disease and to understand when referral to an adult congenital heart disease (ACHD) center is necessary.Furthermore,as many forms of simple and moderate-complexity congenital heart disease can be asymptomatic at younger than 18 years, many such individuals will be able to serve in the military and will eventually fall under the care of Veterans Administration (VA)providers.Therefore it is important for cardiologists at VA medical centers (VAMC) to be familiar with the management of ACHD.The following provides a case-based example of multiple forms of ACHD experienced at a single VAMC and reviews the management of each form.
Case 1: Persistent Left Superior Vena Cava, Sinus Venosus Defect,and Partial Anomalous Right Superior Pulmonary Vein
A 73-year-old man with no significant medical history was found to be in atrial flutter before cataract surgery.A transthoracic echocardiogram (TTE)was performed and revealed severe right-sided chamber enlargement and a dilated coronary sinus.Estimated right ventricular (RV) systolic pressure was within normal limits.A left-arm injection of agitated saline revealed early fllling of the coronary sinus before fllling of the right ventricle, suggesting a persistent left superior vena cava.However, bubbles were also shown to flll the left ventricle despite no obvious ASD being visualized on color flow Doppler echocardiography.The patient underwent a transesophageal echocardiogram (TEE), which showed a large sinus venosus ASD, partial anomalous pulmonary venous return of the right superior pulmonary vein, moderate tricuspid regurgitation,and a severely enlarged coronary sinus ( Figure1 ).The presence of an anomalous right superior pulmonary vein was confirmed by MRI.Because of significant right-sided chamber enlargement and the absence of pulmonary hypertension as revealed by right-sided heart catheterization, the patient was referred for surgical repair.A pericardial patch was used to close the ASD and baffle the anomalous right superior pulmonary vein to the left atrium.The postoperative course was uneventful, and the patient was discharged home in a stable condition.
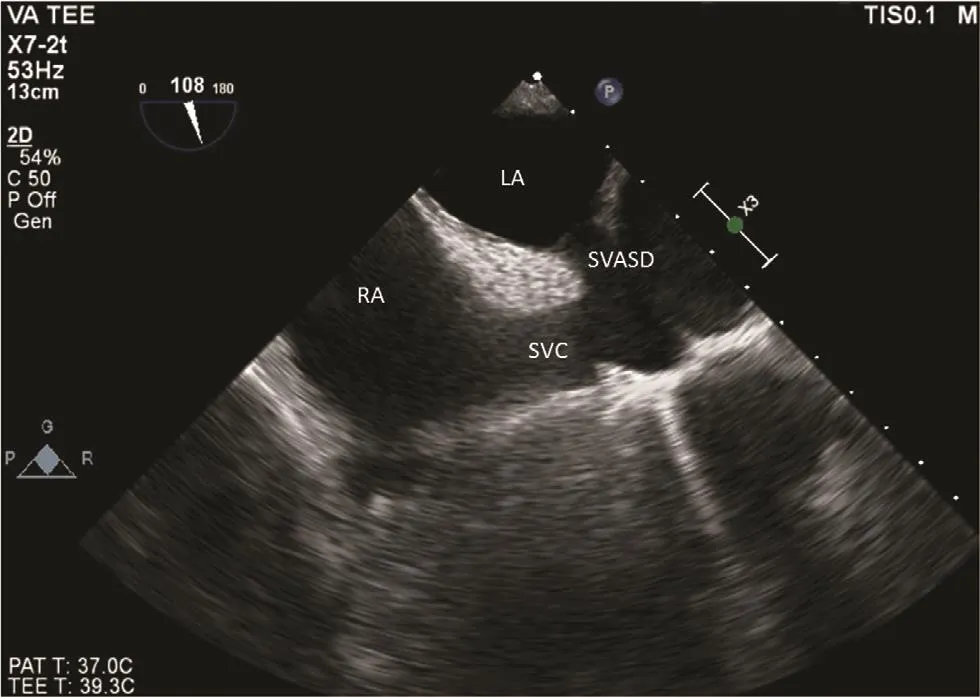
Figure1 A Sinus Venosus Atrial Septal Defect (SVASD)Coming from the Superior Vena Cava (SVC) Visualized on a Modified Bicaval View on Transesophageal Echocardiogram(TEE).
The most important lesson from this case is that the patient had isolated right-sided chamber enlargement despite no obvious presence of pulmonary hypertension, as well as positive bubble study flndings despite no obvious ostium secundum ASD.In this instance, a sinus venosus ASD should be high on the differential diagnosis as it is often difficult to flnd on TTE and usually requires a TEE.A sinus venosus ASD is usually associated with anomalous pulmonary venous return, which has been noted in as many as 97% of patients at the time of surgery[2].For technical reasons, sinus venosus ASDs should be closed surgically as opposed to percutaneously.Right-sided chamber enlargement and a net left-to-right shunt (Qp/Qs ≥ 1.5) in the absence of significant pulmonary hypertension are among the reasons to repair the defect [1].
Case 2: Right-Sided Anomalous Venous Return to the Coronary Sinus
A 64-year-old man with a medical history of type 2 diabetes mellitus and tobacco use presented with a chief concern of progressively worsening dyspnea and lower extremity edema.He underwent a TTE, which showed a severely dilated coronary sinus and moderate RV dilation.A bubble study was performed but did not show any evidence of rightto-left shunt.Cardiac computed tomography conflrmed anomalous pulmonary venous return of the entire right-sided pulmonary venous system, which emptied into an enlarged coronary sinus ( Figure2 ).The patient was referred for invasive hemodynamics, which showed a Qp/Qs ratio of 2.6.He was then referred for surgery, and underwent correction of the anomalous right-sided pulmonary venous return, creation of a fenestration from the coronary sinus to the left atrium, and bovine pericardial patch of the ostium of the coronary sinus.The operation was complicated by hemopericardium requiring a pericardial window, after which the patient was eventually stabilized and discharged home.
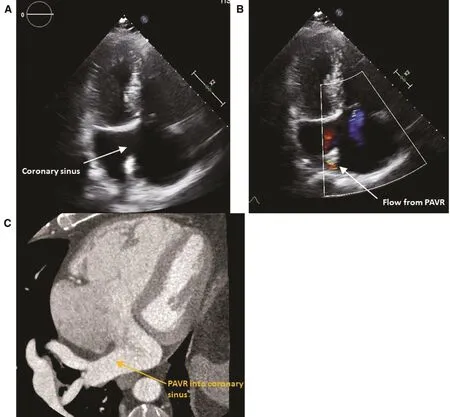
Figure2 Complete Anomalous Pulmonary Venous Return of the Right-Sided Pulmonary Veins.
In patients with right- or left-sided anomalous pulmonary venous return, there is a class I recommendation for surgical repair if functional impairment is present as well as RV enlargement and a net leftto-right shunt (Qp/Qs ≥ 1.5) in the absence of significant pulmonary hypertension.There is a class IIa recommendation to repair anomalous pulmonary venous return in the absence of symptoms if RV enlargement and net left-to-right shunt are present [1].
Case 3: Cor Triatriatum
A 39-year-old man presented to the VAMC to establish care.He had a history of a stroke a few years after being discharged from the marines.He was told his stroke was due to a congenital heart defect.He underwent a TTE, which revealed a membrane across the left atrium and the Doppler profile shown in Figure3 .The flndings were suggestive of the presence of a cor triatriatum.The patient was also incidentally noted to have a bicuspid aortic valve.A TEE was performed, which showed multiple small fenestrations in the membrane, one of which is depicted in Figure3.
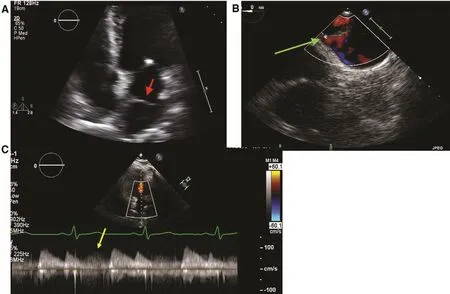
Figure3 Cor Triatriatum.
Cor triatriatum sinister is a rare congenital heart defect found in only approximately 0.4% of patients with congenital heart disease on autopsy [3].It is associated with other forms of congenital heart disease, such as ostium secundum ASDs, ventricular septal defects, anomalous pulmonary venous return,and bicuspid aortic valves in up to 80% of cases [3].The membrane of a cor triatriatum usually divides the left atrium into two chambers: one that receives pulmonary venous drainage and the other that contains the left atrial appendage and mitral valve[1, 3].There are three classifications, one in which there is no connection between the two chambers,the second in which there are multiple small fenestrations, and the third in which there is a single large fenestration [3].
The clinical presentation can mimic symptoms of mitral stenosis if the gradient across the membrane is substantial, and can include dyspnea, pulmonary edema, hemoptysis, atrial arrhythmias, and embolic phenomena [3].The goals of TTE and TEE should be to identify the membrane and the fenestrations,and to measure the continuous-wave Doppler gradient, which has a unique profile, such that in addition to the typical characteristic E and A waves from diastolic flow across the mitral valve, there is a gradient in systole representing the continuous gradient faced by pulmonary venous drainage across the membrane.Furthermore, guidelines recommend additional imaging (TEE, CT, or MRI) to search for associated congenital defects [1].Our institution typically performs a TEE to better assess the fenestrations and to search for common associated congenital anomalies, such as ASD and bicuspid aortic valves, if they are not obvious from the TTE.We typically also perform cardiac MRI, which can also better delineate the membrane, fenestrations,and turbulent flow, and identify further congenital anomalies, such as anomalous pulmonary venous return.
Case 4: Congenitally Corrected Transposition of the Great Arteries
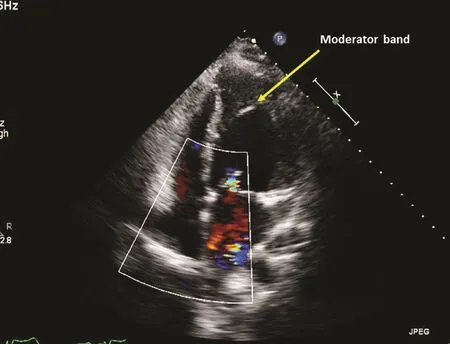
Figure4 Congenitally Corrected Transposition of the Great Arteries where the Systemic Ventricle is a Morphologic Right Ventricle as can be seen by the Presence of a Moderator Band.
A 24-year-old man presented to establish care with cardiology at the VAMC.While in the US Navy he was hospitalized for pneumonia and had a chest X-ray with an abnormal cardiac silhouette and underwent a TTE and TEE and was told he had a congenital heart defect.He was reasonably active, working outdoors with little restriction.His examination was noteworthy of a 2/6 early, midfrequency systolic murmur loudest at the apex.He underwent a TTE, which revealed atrioventricular (AV) and ventricular-arterial discordance(ventricular inversion) consistent with congenitally corrected transposition of the great arteries(ccTGA).There was mild dysfunction of the systemic ventricle (morphologic right ventricle), with mild to moderate left-sided AV valve regurgitation(morphologic tricuspid valve–the valves follow the ventricles) ( Figure4 ).Despite the patient feeling relatively asymptomatic, he was referred to an ACHD center because of the presence of early left ventricular (anatomic RV) dysfunction and AV (tricuspid) valve regurgitation.
In ccTGA there is AV and ventricular-arterial discordance, and as opposed to classic transposition of the great arteries, there is normal oxygenation of pulmonary blood flow, and thus patients are not cyanotic.The right atrium empties via a mitral valve into the morphologic left ventricle and then empties into the pulmonary artery.The left atrium empties via the tricuspid valve into the morphologic right ventricle, which empties into the aorta.There are several problems that arise later in life in patients with ccTGA.Close to 70% of patients will eventually develop systolic dysfunction of the systemic ventricle (morphologic right ventricle)[4].Most patients have a structurally abnormal tricuspid valve and develop tricuspid regurgitation[1, 5].Finally, an anatomically abnormal AV node leads to a high frequency of complete heart block,and many patients will eventually require permanent pacemaker implantation [5].Early referral to an experienced ACHD center is recommended.
Conclusion
Congenital heart disease can remain asymptomatic into adulthood, often allowing military service members to go undiagnosed.For this reason,VAMC providers need to maintain at least a fundamental understanding of ACHD.
Conflict of Interest
The author declares that he has no conflicts of interest.
 Cardiovascular Innovations and Applications2019年2期
Cardiovascular Innovations and Applications2019年2期
- Cardiovascular Innovations and Applications的其它文章
- A Tale of Two STEMI’ s
- Differential Impact of Appropriate Use Criteria on the Association between Age and Abnormal Stress Myocardial Perfusion SPECT
- Using 3D-Printed Models to Advance Clinical Care
- Evaluation of the Patient with Incidental Left Ventricular Hypertrophy on Echocardiography
- Practical Clinical Application of Cardiac Computed Tomography– Derived Fractional Flow Reserve
- Imaging Beyond the Angiogram in Women with Suspected Myocardial Infarction and No Obstructive Coronary Artery Disease