
Imaging Beyond the Angiogram in Women with Suspected Myocardial Infarction and No Obstructive Coronary Artery Disease
2019-05-11 06:01:58SohahIqbalMDFACCFSCAI
Sohah N.Iqbal, MD, FACC, FSCAI
1 NYU Langone Medical Center, New York, NY, USA
Abstract
Keywords: women; myocardial infarction; imaging; angiogram; intracoronary imaging; cardiac MRI
Introduction
Women presenting with suspected myocardial infarction (MI) found to have no obstructive coronary artery disease (CAD) make up a significant minority of patients referred for coronary angiography, up to 30% [1–4].Historically, after the angiogram these women had no definitive diagnosis for their presenting event and no tailored treatment.Registry data suggest that the prognosis of these patients is not good, with a 12-month mortality rate possibly as high as 4.7% [5] and a mortality rate comparable to that of MI patients with obstructive CAD at 12 months [3] as well as 36 months after reinfarction [6].It has become apparent that further assessment of these patients is warranted, and multimodality imaging may help clarify diagnoses and guide treatment.
The clinical term MINOCA (MI with nonobstructive coronary arteries) has been coined to tailor the conversation to a specific group of patients who present with clinically diagnosed MI (as defined by the universal definition of MI [7]), have no obstructive CAD, and in whom clinically apparent diagnoses such as demand ischemia, pulmonary embolism, myocarditis, and vasospasm caused by sympathomimetic agents have been ruled out [8].Women are much more likely than men to present with MINOCA [1–4].The causes of MINOCA are thought to include plaque disruption with possible atherothrombotic emboli and/or transient thrombosis, macrovascular or microvascular vasospasm, and spontaneous coronary artery dissection (SCAD),and need to be differentiated from possible noncoronary causes such as takotsubo cardiomyopathy and unrecognized myocarditis.Once MINOCA is suspected, further imaging plays a necessary role in teasing out the underlying mechanism.
Cardiac Magnetic Resonance Imaging to Further Characterize the Mechanism of Myocardial Injury
Cardiac magnetic resonance imaging (cMRI) is the noninvasive modality of choice in patients with suspected MINOCA.It has the potential to identify and distinguish between MI, myocarditis, and takotsubo cardiomyopathy.The protocols used to further characterize the causes of disease in patients with suspected MINOCA include cine imaging for wall motion, late gadolinium enhancement (LGE)to identify areas of scar, and T2-weighted protocols to also assess patients for edema.
In a recent quantitative assessment using a metaanalysis approach of 16 cMRI studies performed within 6 weeks of the index MI (1966– 2013), features consistent with an MI (subendocardial infarct)were reported in 24% of 1167 MINOCA patients,features consistent myocarditis were reported in 38% of 1066 patients, features consistent with takotsubo cardiomyopathy were reported in 16% of 1083 patents, and no abnormality was reported in 21% of 1066 patients [5].This frequency of approximately a quarter of all patients with suspected MINOCA having ischemic LGE on cMRI is consistent in three more recent studies (21– 23%) [9–11].
Findings of no abnormalities on cMRI in patients with suspected MINOCA are reported in multiple cMRI studies [5, 9, 10].No LGE on MRI suggests no scar or focal area of infarct.Although cMRI has a reported sensitivity of as little as 1 g of myocardial necrosis [12], factors such as the timing of cMRI from the presenting event need to be considered as well as causes that may cause a “ broader spatial distribution of myonecrosis” [8].It is important to note that patients with normal cMRI flndings have lower troponin levels [5, 13].Earlier studies did not always include T2-weighted imaging, and more recent protocols have increased sensitivity as compared with protocols used in the early cMRI studies of MINOCA[14, 15].Normal cMRI flndings likely represent a subset of patients with suspected MINOCA that warrants further research moving forward.
The level of agreement between initial cardiologist diagnosis and cMRI flndings was shown to be poor in one study, with the lowest level of agreement seen for acute MI, with cMRI assisting in a flnal consensus diagnosis [9].In clinical practice, a cMRI study with LGE and T2-weighted imaging in patients with suspected MINOCA and unclear flnal diagnosis may be very helpful in charactering noncoronary and coronary causes of injury and could guide further testing as well as management.
Invasive coronary intravascular imaging, such as intravascular ultrasonography (IVUS) and optical coherence tomography (OCT), at the time of cardiac catheterization can identify coronary disease missed on angiography.These modalities can also help better define SCAD when angiographic flndings are suggestive but not definitive.Coronary causes of MI such as atherosclerotic plaque disruption (including plaque rupture and erosion) not seen on routine angiography have been identified in studies involving intravascular imaging in patients with MINOCA [11, 13].Plaque disruption of nonobstructive atherosclerotic disease can lead to MI by a variety of mechanisms, including transient thrombotic occlusion with lysis before angiography, associated vasospasm, and distal embolization of plaque ( Figure1 ).
OCT has higher spatial resolution than IVUS and has been shown to be able to identify relatively more plaque disruption and thrombus [16].However, as IVUS has historically been the more widely available technology and preceded the routine use of OCT, initial MINOCA studies were performed with IVUS.In a prospective cohort of 42 women who underwent IVUS of at least two epicardial vessels, including the suspected infarctrelated artery, plaque disruption was seen in 38%of patients (median troponin level 1.6 mg/dL), with no thrombus identified ( Figure2 ).In a cohort of 38 MINOCA patients (55% women) who underwent OCT, there was evidence of plaque disruption in nine patients (24%) and thrombus was identified in flve patients with plaque disruption and two patients without plaque disruption [11].These flndings were correlated with cMRI flndings and an LGE pattern suggesting MI was more common in patients with plaque disruption and/or thrombus than in patients without these intravascular flndings [11].
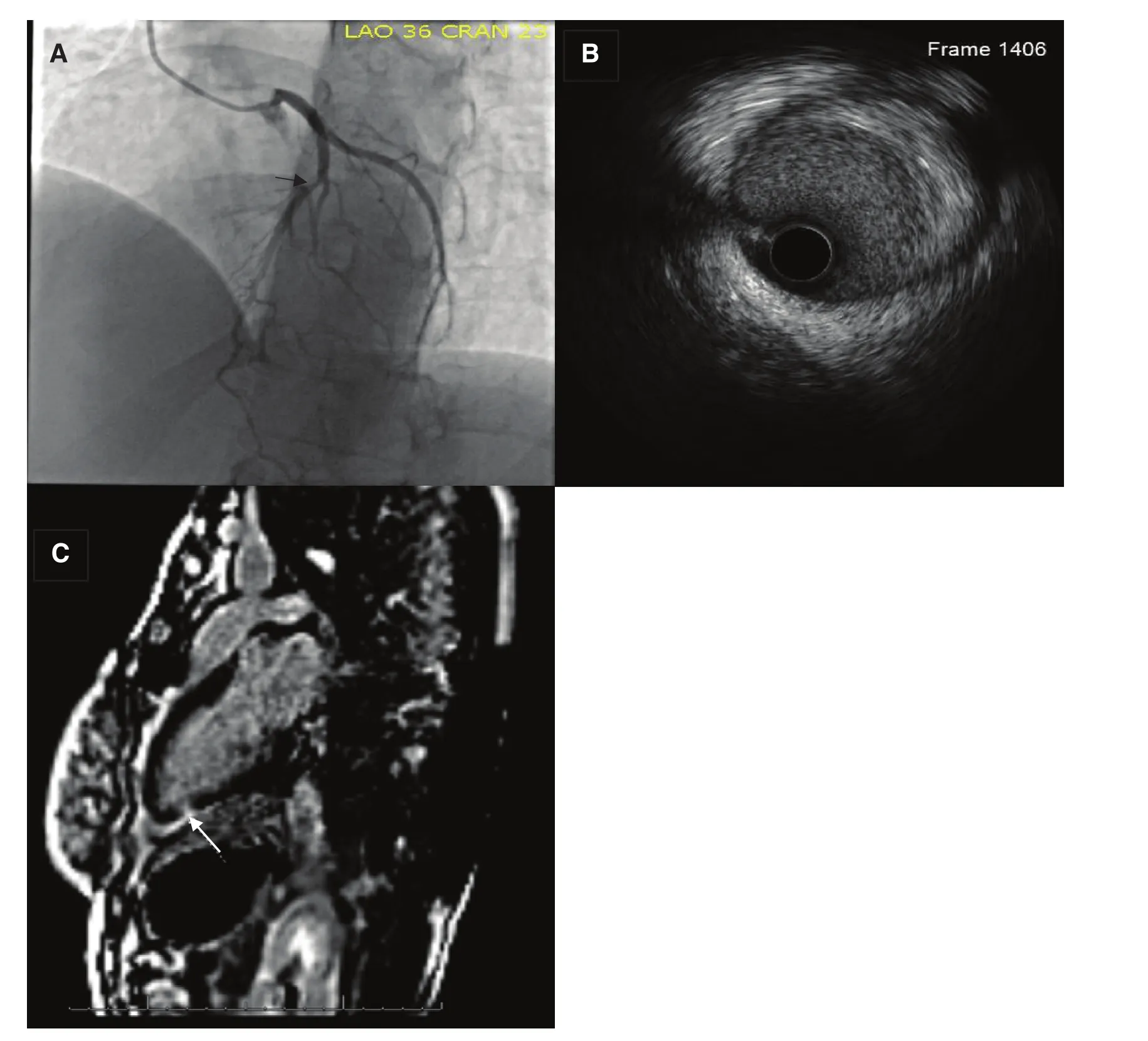
Figure1 Angiogram (A) and Corresponding IVUS (B) and cMRI with LGE (C) of a 40 Year Old Woman Who Presented with Chest Pain after a Recent Miscarriage and a Mildly Elevated Troponin.
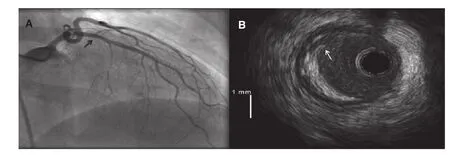
Figure2 Angiogram (A) Demonstrates Mild Coronary Artery Disease in a Middle Aged Woman Who Presented with Suspected MI and Only Mild CAD on Angiography.
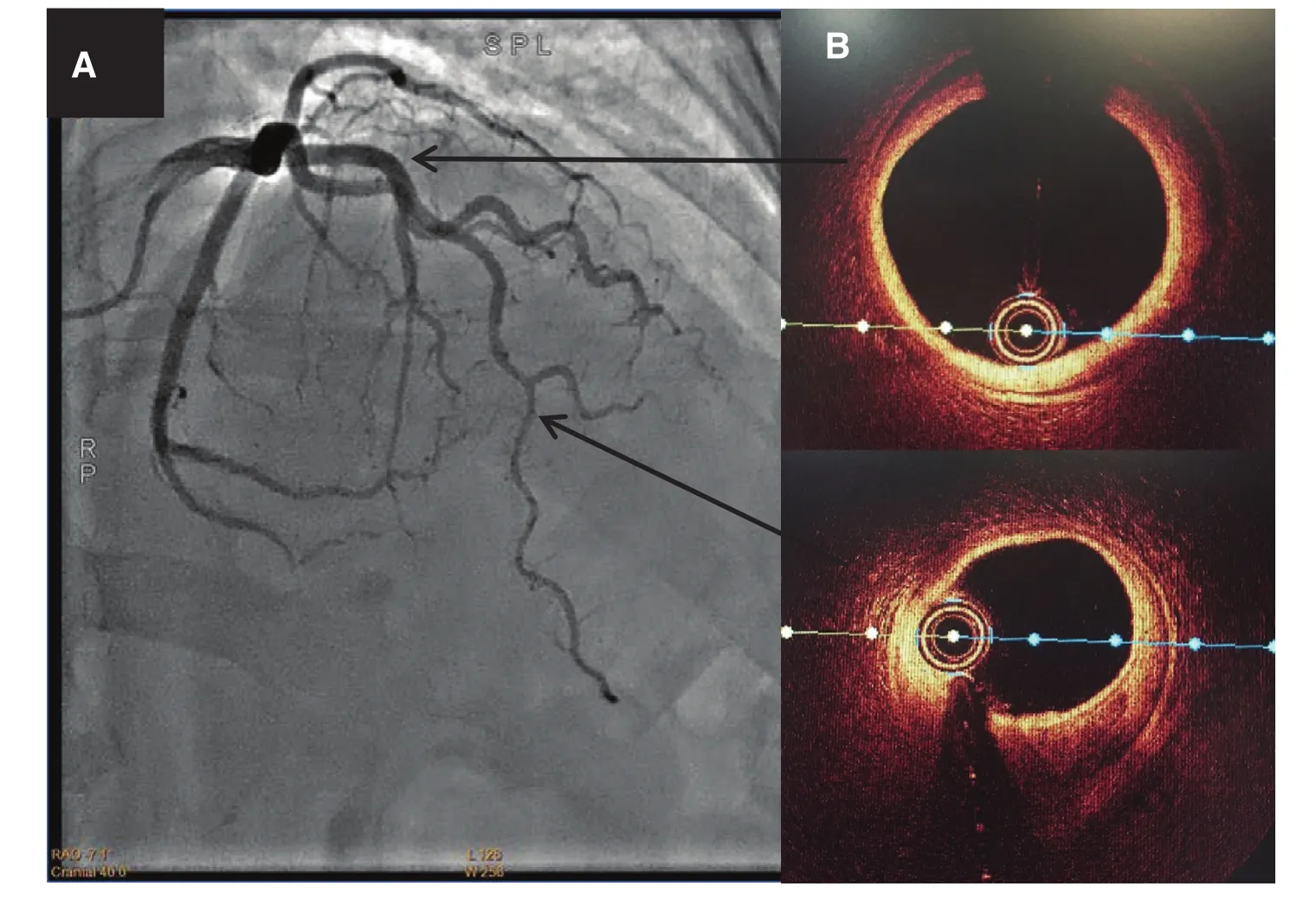
Figure3 Angiogram (A) and Corresponding OCT (B) of a 61 Yo Women Who Presented with an NSTEMI.
The multicenter Women’ s Heart Attack Research Program (HARP) imaging study is currently in progress with the aim to recruit 500 women with MINOCA who will undergo complete three-vessel OCT and cMRI with both T2-weighted imaging and LGE [17].This will be the largest advanced imaging study to date in women with suspected MINOCA.
SCAD is a clinical entity, predominantly in women, that can be identified by coronary angiography; however, it has been increasingly recognized that the diagnosis can be missed if the angiographic pattern is nondiagnostic [18].IVUS and OCT can help distinguish SCAD in such cases, specifically type 3 SCAD, which is defined as angiographically mimicking atherosclerosis [19].Given that the treatment options in patients with plaque disruptions are thought to be different from those in patients with SCAD,specifically statin use as well as possible antiplatelet use, distinguishing between these two entities should be a priority in caring for women with MINOCA.Intravascular imaging can also be useful in defining the extent of SCAD, and is particularly helpful in the case of type 2 SCAD,which is defined as smooth narrowing, where the diagnosis is unclear and the extent of the dissection can be missed ( Figure3 ).
Intravascular imaging in patients with MINOCA has helped describe coronary disease that was not identified in the past.Through these studies we have been able to identify patterns previously unrecognized that should allow us to go one step further and study treatment options in the subsets of MINOCA patients.The role of routine intravascular imaging in clinical practice needs to be better defined.Although we know that angiographically normal coronary arteries can have mild, predominantly eccentric atheroma on IVUS [20], at present no plaque disruption has been reported by IVUS or OCT in MINOCA patients with angiographically normal coronary arteries [11, 13].The use of intravascular imaging in clinical practice should be considered on an individual patient basis and can help when the cause remains unclear.
Conclusions
Imaging beyond routine angiography in women presenting with suspected MI and nonobstructive CAD on angiography is essential to define the underlying mechanism.Complete cMRI with cine wall motion,LGE, and T2-weighted imaging can help distinguish MI from myocarditis and takotsubo cardiomyopathy.Intravascular imaging at the time of coronary angiography can help in identifying plaque burden,plaque disruption, and the presence of thrombus,and in distinguishing SCAD from mild CAD.The ongoing HARP study may provide further insight into the use of OCT and cMRI in women with suspected MINOCA.
Conflict of Interest
The authors declare no conflict of interest.
 Cardiovascular Innovations and Applications2019年2期
Cardiovascular Innovations and Applications2019年2期
- Cardiovascular Innovations and Applications的其它文章
- A Tale of Two STEMI’ s
- Adult Congenital Heart Disease in the Veteran Population: A Case-Based Report
- Differential Impact of Appropriate Use Criteria on the Association between Age and Abnormal Stress Myocardial Perfusion SPECT
- Using 3D-Printed Models to Advance Clinical Care
- Evaluation of the Patient with Incidental Left Ventricular Hypertrophy on Echocardiography
- Practical Clinical Application of Cardiac Computed Tomography– Derived Fractional Flow Reserve