
Using 3D-Printed Models to Advance Clinical Care
2019-05-11 06:02:00MollyPantelicMilanPantelicMDToddPietilaMarianneRolletEricMyersThomasSongMDWilliamNeillMDandDeeDeeWangMDFACCFASEFSCCT
Molly Pantelic , Milan Pantelic, MD , Todd Pietila , Marianne Rollet , Eric Myers ,Thomas Song, MD , William W.O’ Neill, MD and Dee Dee Wang, MD, FACC, FASE, FSCCT ,
1 Center for Structural Heart Disease, Division of Cardiology, Henry Ford Health System, 2799 West Grand Boulevard, Detroit,MI 48202, USA
2 Department of Radiology, Henry Ford Health System, 2799 West Grand Boulevard, Detroit, MI 48202, USA
3 Materialise, 44650 Helm Ct, Plymouth, MI 48170, USA
4 Henry Ford Innovation Institute, Henry Ford Health System, 2799 West Grand Boulevard, Detroit, MI 48202, USA
Abstract
Keywords: 3D printing; Left atrial appendage; transcatheter mitral valve; structural heart; TAVR
Introduction
Since its commercialization in the 1980s, threedimensional (3D) printing has grown to a more than $7 billion industry (in 2018), with much of this growth driven by its applications in medicine [1].Healthcare is one of the largest beneficiaries of 3D printing as the technology’ s ability to cost-effectively manufacture unique and geometrically complex objects makes it an excellent choice for patient-specific products.Examples of 3D printing in the clinical setting include anatomical models for surgical planning and training, patient-matched surgical instruments, and a variety of implantable devices designed to flt a patient’ s unique anatomy.To date, more than 80 3D printed medical devices have been cleared by the US Food and Drug Administration [2].
Defining 3D Printing
3D printing, or additive manufacturing, creates a 3D physical object by building one layer of material upon another until the 3D shape is created.This method allows greater design freedom,higher part complexity, and the ability to manufacture unique objects more rapidly than conventional manufacturing techniques.3D printing is available in several different technologies, with stereolithography, selective laser sintering, material jetting,and fused-deposition modeling being the primary methods used in medicine.Each technology has its advantages, depending on the unique characteristics and material requirements of the 3D printed object.
Medical Applications of 3D Printing
Medical applications of 3D printing have diversifled greatly since the early 1990s.When 3D printing flrst emerged, it was a technology applied for surgical preprocedural visualization and planning,enabling surgeons to hold their patient’ s anatomy in their hands before operation.Once 3D printing became a standard of care in clinical professions such as dentistry and craniomaxillofacial surgery and demonstrated market potential, the industry made investments in more sophisticated software tools to increase the scalability of personalized medicine enabled by 3D printing.The flrst wearable 3D printed products soon emerged with the digitization of hearing aid manufacturing.Nearly all hearing aid shells are now manufactured by 3D printers,and other wearable technologies, such as custom,3D printed eyeglasses, are increasingly popular and widespread ( Figure1 ).

Figure1 : 3D Printed Glasses.
In the last decade, implantable 3D printed devices have also emerged, allowing implants to be designed and manufactured specific to a patient’ s anatomy.These innovations leverage metal materials and are primarily used for orthopedic joint replacement in cases of complex revision surgery or challenging anatomy.Additionally, the development of virtual planning solutions has been instrumental in the rise in popularity of 3D printed surgical tools, enabling the conversion of a software plan to the operating room via a custom instrument or guide made specific to a patients anatomy.
3D Printing in Cardiology
Cardiology has been later in adopting 3D printing primarily due to an absence of physician access to imaging hardware and software capable of acquiring the necessary medical imaging dataset to facilitate this technological advancement.Within the past 5 years, the availability of new-generation electrocardiographic gated multidetector cardiac computed tomography (CT) scanners, the development of advanced 3D transesophageal echocardiographic imaging capabilities, and improvements in biomedical engineering software supporting 3D printing have all contributed to significant growth in the use of the technology in cardiology.3D printing applications have grown rapidly in popularity largely as a tool to aid in procedure visualization and planning.The complex and unique geometry associated with congenital heart conditions has made 3D printing exceptionally well suited to presurgical planning in the fleld, allowing a multidisciplinary team to gain a better understanding of anomalous anatomy and optimal treatment approaches( Figure2 ).Furthermore, interventional cardiologists and pediatric cardiothoracic surgeons have adopted 3D printing as a tool to assist with device selection and approach for challenging structural heart procedures.
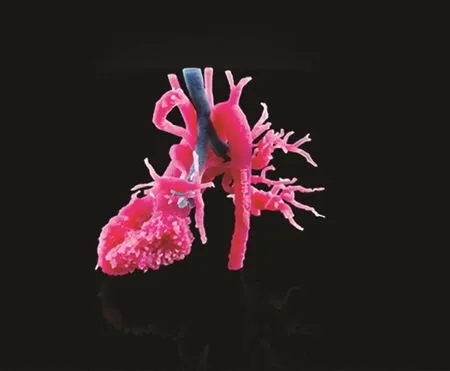
Figure2 : 3D Printed Pediatric Heart used for Congenital Surgical Planning.
How to Get to 3D Prints: The Workflow
High-quality cardiac imaging serves as the input to most medical 3D printing workflows.As described in Figure3 , the 3D printing process starts with a patient and the acquisition of medical images.The image-acquisition step is of utmost importance,and it is essential to ensure that the proper imaging modality is used and that optimal data quality is achieved.The resultant medical images, supported in a Digital Imaging and Communications in Medicine (DICOM) format, are then processed with specialized software to isolate the desired anatomical regions of interest.This process, termedsegmentation, can be accomplished with both automated and manual software algorithms.Once the relevant anatomy has been isolated from the images, a 3D surface model is rendered, most commonly in a format known asStandard Tessellation Language(STL).Before 3D printing, the STL flle is manipulated with 3D software to virtually aid in case planning and to add design requirements based on the intended use and the targeted printing technology.After the 3D-printing process is complete, postprocessing is required to remove residual support material from the object before its use ( Figure3).The robust method outlined here can be applied to planning and device selection in a variety of structural heart procedures, including transcatheter mitral valve replacement (TMVR), transcatheter aortic valve replacement (TAVR), and left atrial appendage(LAA) closure in patients with atrial flbrillation who are at high risk of cerebrovascular events.
3D Printing in Structural Heart Interventions
Application of 3D Printing in LAA Interventions
Traditionally, LAA interventions have been planned with a mixture of transesophageal echocardiography (TEE) and fluoroscopy.However, as has been underappreciated in the past, the LAA is a complex structure with highly variant morphologies that correlate somewhat with patient age and sex [3, 4].Given this anatomical variability and the challenge it poses to procedure planning, 3D printing offers an elegant solution by allowing cardiologists to determine the landing zone and flt the closure device before implantation, thereby ensuring proper sealing and minimizing complications.
3D printing in LAA closure was flrst successfully demonstrated with the WATCHMAN LAA closure device (Boston Scientific, Marlborough, MA,USA) with use of a combination of multidetector CT and stereolithography to generate a 3D print of a patient’ s LAA to flt the WATCHMAN device by hand [5].Subsequent studies demonstrated 3D printing to have reproducibility and feasibility for LAA closure similar to those of various other LAA intervention devices, including the thoracoscopic AtriClip (AtriCure, Mason, OH, USA), LARIAT(SentreHEART, Redwood City, CA, USA),WaveCrest (Coherex Medical, Salt Lake City, UT,USA), and Amplatzer Amulet (St.Jude Medical, St.Paul, MN, USA) devices [6, 7].
Value of 3D Printing in LAA Interventions

Figure3 : Clinical Workflow from Image Acquisition to Making a 3D Print.
In the years since, studies have corroborated the efficacy of 3D printing as a technique to improve patient outcomes in LAA closure.Application of 3D printing in LAA interventions differs depending on institutional specific educational needs.Patient-specific 3D printed models can be used to reduce the early-operator learning curve experienced when new technology is introduced in a health system for the flrst time [8].In preprocedural planning, 3D prints of the LAA and the adjacent anatomy help not only facilitate an understanding of echocardiographic images and landmarks that will be shown intraprocedurally for device guidance but also allow ex vivo bench-test simulation of devices to understand the device landing zone, device flt, and ability to seal the LAA after implantation [8–10].More commonly, 3D prints in LAA interventions have served as a communication tool for implanting physicians, industry clinical fleld specialists, and interventional imaging physicians to discuss procedural and equipment case plans before initiation of the femoral access.
In real-world outcomes comparing 3D-printplanned LAA closure with the standard procedure with the WATCHMAN device, Li et al.found that 3D printing increased procedural success by reducing the occurrence of residual shunts due to incomplete closure; moreover, the 3D-printing group had significantly less radiation exposure as a result of increased planning before the procedure[11].Similarly, Hell et al.[12] found that CT-based 3D-printing modeling was an effective method for accurate LAA sizing in 95% of patients, whereas TEE alone would have undersized the device in 45% of patients.
The value of 3D printing is not limited to device sizing.Liu et al.[13] generated 3D prints of the LAA from 3D-TEE datasets and found the 3D prints were able to predict procedural challenges and select WATCHMAN sizes that were consistent with those used in the actual surgery.Additional studies expanded the role of 3D printing beyond procedural planning and sizing to impacting the investigator learning curve.Preprocedural use of 3D printing was found to correlate with a reduction in the implanter operator learning curve with the Amulet device [14].Long-term value of 3D printing was demonstrated by Conti et al.[15], who demonstrated a significantly higher proportion of patients with postoperative LAA leak secondary to underestimation of prosthesis size in the standard-TEE-approach group as opposed to the CT-based 3D-printing cohort.
Further studies have demonstrated the utility of 3D printing not just for device sizing but also for optimizing additional aspects of the LAA closure procedure.A prospective study by Eng et al.[9] found that use of CT and 3D printing with the WATCHMAN occluder decreased the number of fluoroscopic angles used in the procedure, and reduced both the overall procedure time and the average number of devices used per procedure,again illustrating the advantages of 3D printing over the traditional approach.Similarly, Obasare et al.[16] found CT-based 3D printing to be a rapid, reliable, and intuitive method for determining the best landing zone, and demonstrated its superiority to the standard approach in a wide variety of dimensions.3D printing was correlated with reduced procedure time, reduced anesthesia time, reduced fluoroscopy time, absence of peridevice leak, reduced transseptal puncture to catheter removal time, reduced number of device deployments, and reduced number of devices used.Yet many of these potential suboptimal outcomes arise from the lack of personalized devices for patient-specific anatomy.3D printing may ultimately be only the flrst step toward personalized medicine for effective LAA occlusion.Work is already being performed demonstrating potential outlines for a 3D-printing process to create implants that flt the exact anatomy of each patient’ s unique LAA [17] (Figure4).
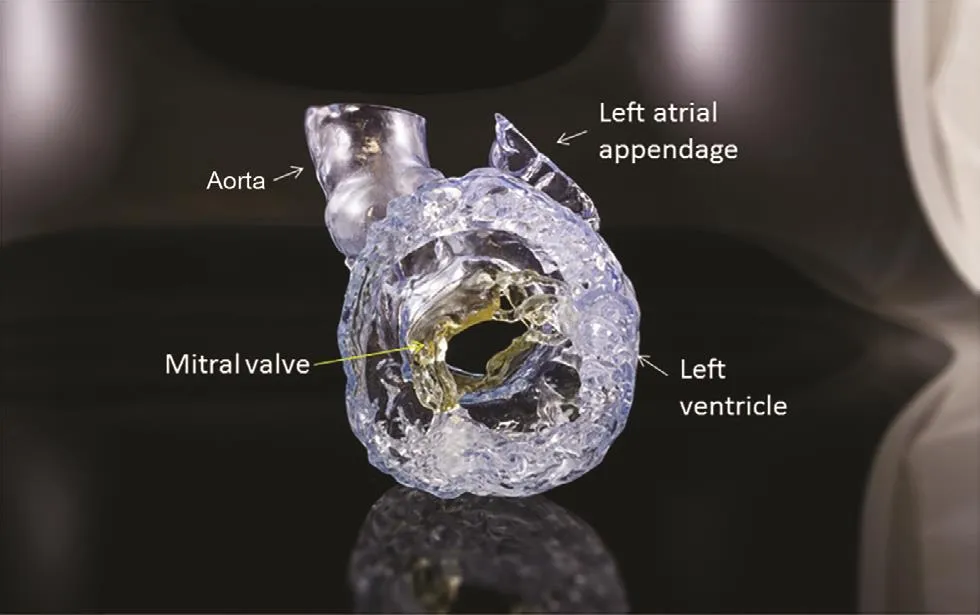
Figure4 : 3D Printed Adult Heart.
Application of 3D Printing in Transcatheter Mitral Valve Interventions
3D printing has also been applied with success in transcatheter mitral valve interventions (TMVR)( Figure3).Transcatheter mitral valve interventions are a relatively new fleld of transcatheter interventions.Patients referred for potential TMVR are evaluated by a multidisciplinary heart team after they have been rejected for traditional open-heart surgery given their underlying frailty or likely inability to recover from surgery.In the absence of surgical bail out for a transcatheter procedure, TMVR interventions are high-risk procedures.Complications such as device embolization, paravalvular leak(PAL), and left ventricular out flow tract (LVOT)obstruction are well documented in the fleld of transcatheter interventions [18, 19].LVOT obstruction is the most feared complication after TMVR as this is associated with catastrophic death in both the near term and the long term [18– 21].
The value of 3D printing and computer simulation in TMVR is dif flcult to quantify.Much like the use of parachutes in the PARACHUTE study, the purpose of the 3D print in preprocedural planning is to prevent a complication [22].In a patient with a large LVOT and minimal risk of LVOT obstruction, there may be little value to 3D printing the anatomy.However, for early operators who are starting to perform TMVR, and early operators who are starting to plan TMVR case plans, the value of the 3D print is in understanding the anatomy that a surgeon can palpate but that a transcatheter-trained implanter and an imager would not comprehend.The value of this in preventing death, and preventing life-threatening LVOT obstruction and hemodynamic collapse, is not quantifiable.Once the earlyoperator learning curve has plateaued, the value of the 3D print may diminish, and dependency on 3D computer-aided design (CAD) simulation is sufflcient for all operators to comprehend.However,until all implanters and operators achieve this level of 3D spatial knowledge, the 3D print serves as a planning, bench-testing, and case communication tool [23].
The ability to 3D print and model a patient’ s anatomy before high-risk TMVR interventions greatly helps in determining a patient’ s eligibility for the procedure.Wang et al.[23] flrst pioneered an approach that combines CAD and 3D printed heart models for transcatheter heart valve testing, allowing physicians to simulate the procedure both virtually and in a 3D model, assessing different angles, depths of deployment, and device flt to measure LVOT surface area and determine the risk of neo-LVOT/LVOT obstruction ( Figure5 ).Later,Wang et al.[24] validated this method in a multicenter trial of patients with severe mitral valve dysfunction, from degenerative surgical mitral ring,bioprosthesis, or severe native mitral stenosis from mitral annular calcification.They performed computer simulations and 3D-printing as part of the analysis using the model as previously described,and then compared predictions with surgical outcome.Of the cases that resulted in neo-LVOT obstruction, they found that the model’ s predicted neo-LVOT surface area had 100% sensitivity and 96.8% specificity for predicting TMVR-induced LVOT obstruction, a compelling result indicative of the need for additional investigation and integration into clinical practice.El Sabbagh et al.[25]retrospectively evaluated a case series of patients who underwent TMVR and found that sizing with a 3D print was consistent with the valve used in the procedure in six of eight patients, and LVOT obstruction and paravalvular gaps that occurred in several of the patients during the actual procedure were predicted by the model.As 3D printing in transcatheter interventions is in its infancy and most TMVR technologies are still in early-feasibility clinical trials, virtual modeling 3D printing will continue to serve a greater role for patient care in and delivery of TMVR therapies.
Application of 3D Printing in TAVR
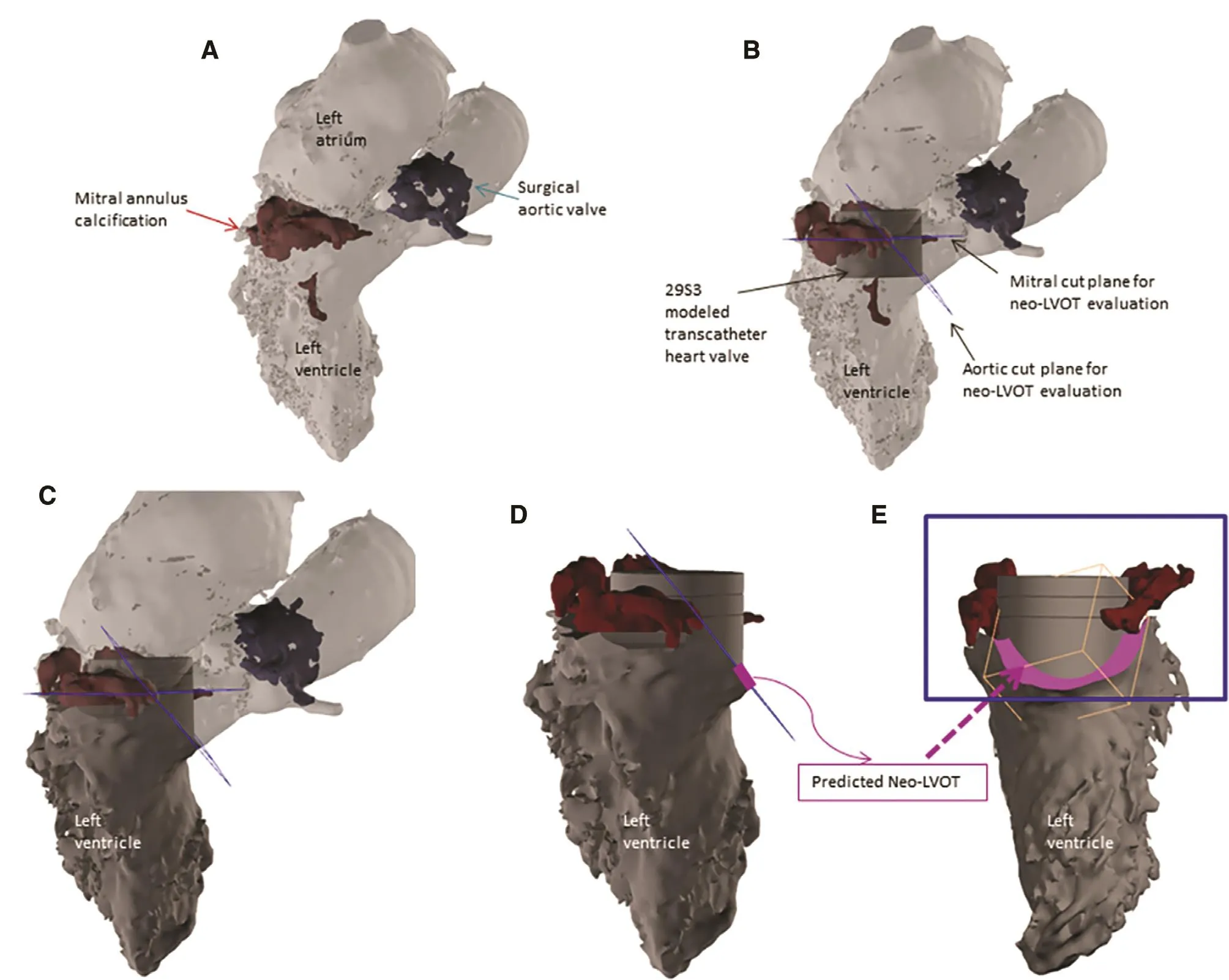
Figure5 : Modeling to Predict Left Ventricular Outflow Tract Obstruction (LVOT) before Transcatheter Mitral Valve Replacement (TMVR).
3D printing has also become a significant area of investigation in TAVR.Physical 3D prints allows investigators to perform modeling of the aortic root ex vivo to flt TAVR devices before the procedure to predict patient risk of PVL.In a retrospective, single-center study by Hosny et al.[26], 30 patients who had undergone TAVR with either a balloon-expandable or a self-expanding valve were selected, 15 of whom had a successful annular seal and 15 of whom had demonstrated PVL.After software analysis of the patients’ preprocedural CT scans, 3D printed models of the aortic root were created to retrospectively size the valves.Incorporation of the 3D prints demonstrated investigator ability to correctly detect the adequateness of annular seal in 73.3% of patients who had received a balloon-expandable valve and in 60%of patients who had received a self-expanding valve.Moreover, regions of the valve with inadequate seal corresponded well with PVL regions detected on postprocedural TEE.Ripley et al.[27]constructed 3D printed aortic root models from 16 patients who had undergone TAVR, and found that their models were highly correlative to predicting PVL in six of nine patients and absence of PVL in flve of seven patients.
Beyond rigid 3D printed models, work has been pioneered on soft-tissue-mimicking models.Qian et al.[28] studied flexible tissue-mimicking 3D prints of the aortic root and found that the annular bulge index, a measurement developed to determine post-TAVR annular strain unevenness in 3D models, was a highly accurate predictor of post-TAVR PAL.The annular bulge index originally derived from 3D prints outperformed other, more established variables investigated.A 3D-printing approach using the annular bulge index has also been investigated in TAVR.In patients with severe aortic stenosis secondary to bicuspid aortic valve disease, the 3D-print annular bulge index has similarly been demonstrated to be an accurate predictor of PVL in this subset patient population [29].
3D Printing in Simulation Training
Given the ability of models to be used in a benchtest environment to predict potential outcomes of transcatheter interventions, multiple 3D printed simulation training tools have been developed to decrease the learning curve for new technology development and implementation.3D printing was studied by Rotman et al.[30] as part of a more complex modeling tool, termed theReplicator,to simulate TAVR devices and train interventional cardiologists.The Replicator starts with 3D printing to construct an accurate model of upperbody vasculature, and also contains an automated Windkessel mechanism to simulate physiological flow.Researchers are able to simulate calcified aortic valves in the Replicator and then model TAVR procedures with an experienced cardiologist, comparing procedure metrics with established clinical data in patients.Early results demonstrate the Replicator is able to produce procedure metrics comparable to clinical data, and its use is thus an effective method for TAVR valve bench testing and physician training.Application of 3D-print-based simulation training may have a role not only in the early-operator learning curve but also in preparation for navigating challenging anatomies and new-device-technology learning curves.
Conclusion
As the emphasis on personalized, patient-centered healthcare continues to grow, it is unsurprising that 3D printing is increasingly being recognized as an indispensable tool for best practices, both in cardiology and in the larger medical fleld.Given the technology’ s demonstrated benefits in risk reduction, decreasing radiation exposure, shortening procedure times, reducing the number of devices used, and improving overall procedural outcomes via modeling and planning, it is clear that 3D printing has significant advantages in cardiology for patients and providers alike.Moving forward,the continued success of structural heart disease therapies will be driven by innovation and improvements in 3D-printing and 3D-modeling methods and by increasing access of this technology to a wider subset of providers.To that end, it will be important to reduce cost, while also engaging in advocacy to guarantee that the laborious and interdisciplinary nature of this work is adequately compensated; notably, Medicare does not have a reimbursement code for 3D printing, and this currently limits the technology’ s feasibility on a national scale.Although the barriers that prevent adoption of 3D printing and 3D modeling as the standard of care are not insignificant, the 3D-printing and 3D-modeling technology as it exists today does not solve every problem inherent to structural heart interventions.The real value of personalized medicine and patient-centric care has not yet been fully discovered.For physicians and patients alike, continued research and refinement of this new clinical workflow is worthy of more investigation in cardiology and in medicine as a whole to ensure that each patient is treated as the anatomically distinct individual they are.
Acknowledgments
The authors thank Dr.Scott Dulchavsky, Mark Coticchia, and Ruth Fisher for their support of 3D printing in healthcare delivery at Henry Ford Health System.
Conflict of Interest
Dee Dee Wang is a consultant to Edwards Lifesciences, Boston Scientific, and Materialise,and receives research grants from Boston Scientific.Todd Pietila is employed by Materialise.William W.O’ Neill is a consultant to Edwards Lifesciences,Medtronic, Boston Scientific, Abbott, and St.Jude Medical, and serves on the board of Neovasc.Marianne Rollet, Eric Myers, Molly Pantelic,Thomas Song, and Milan Pantelic declare they have no conflicts of interest.
 Cardiovascular Innovations and Applications2019年2期
Cardiovascular Innovations and Applications2019年2期
- Cardiovascular Innovations and Applications的其它文章
- A Tale of Two STEMI’ s
- Adult Congenital Heart Disease in the Veteran Population: A Case-Based Report
- Differential Impact of Appropriate Use Criteria on the Association between Age and Abnormal Stress Myocardial Perfusion SPECT
- Evaluation of the Patient with Incidental Left Ventricular Hypertrophy on Echocardiography
- Practical Clinical Application of Cardiac Computed Tomography– Derived Fractional Flow Reserve
- Imaging Beyond the Angiogram in Women with Suspected Myocardial Infarction and No Obstructive Coronary Artery Disease