
Differential Impact of Appropriate Use Criteria on the Association between Age and Abnormal Stress Myocardial Perfusion SPECT
2019-05-11 06:02:02SaurabhMalhotraMDMPHFACCFASNCandRamiDoukkyMDMScFACCFASNCFASE
Saurabh Malhotra, MD, MPH, FACC, FASNC and Rami Doukky, MD, MSc, FACC, FASNC,FASE
1 Division of Cardiology, Cook County Health, Chicago, IL, USA
2 Division of Cardiology, Rush University, 1653 W.Congress Parkway Chicago, IL 60612, USA
Abstract
Keywords: appropriate use criteria; myocardial perfusion imaging; age; coronary artery disease; single-photon emission computed tomography
Introduction
Age is a strong determinant of the risk of coronary artery disease (CAD).According to the Diamond and Forrester classification, the pretest likelihood of CAD is significantly greater among elderly patients,regardless of typicality of symptoms [1].While CAD risk factors, especially diabetes mellitus [2],are strong determinants of CAD risk as well, the value of the burden of CAD risk factors in predicting myocardial ischemia seems limited among the elderly [3].Appropriate use criteria (AUC) guide physicians to refer patients for single-photon emission computed tomography (SPECT) myocardial perfusion imaging (MPI) and are based on the likelihood of the test to provide meaningful diagnostic information [4].We previously reported the diagnostic and prognostic value of appropriate SPECT MPI from a community-based cohort of patients[5].We previously reported that there is no demonstrable sex-based differential impact of AUC on the diagnostic or prognostic utility of SPECT MPI [6].However, the impact of AUC on the diagnostic yield of MPI among elderly patients, who have a high likelihood of CAD, has not been studied.In this study,we sought to investigate the impact of AUC on the diagnostic yield of SPECT MPI among the elderly.
Methods
This report is a subanalysis of a previously published multisite prospective cohort study of 1511 consecutive patients, all of whom were referred for clinically indicated SPECT MPI in the outpatient setting [5].The detailed method of the study, including the study population and MPI testing, was published previously [5].Briefly, 1707 consecutive patients who underwent SPECT MPI between August 15, 2007,and May 15, 2011, were identified.These patients were referred from the offices of 22 physicians (20 primary care physicians and two cardiologists) in 11 private practices.Among these patients, 182 met one or more exclusion criteria and 14 (0.9%) patients were lost to follow-up.The remaining 1511 eligible patients (99.1%) were prospectively followed up for 27 ± 10 months.The study was approved by the Institutional Review Board of Rush University Medical Center (Chicago, IL, USA).
Clinical Data and Appropriate Use Criteria Determination
Patient demographics, referral diagnosis, risk factors, and cardiovascular history were recorded before stress MPI.Known CAD was defined as a history of myocardial infarction (MI), prior percutaneous or surgical revascularization or anatomical stenosis of 50% greater on coronary angiography.Patient medical records, including the referring physician clinical evaluation, preceding MPI were reviewed to determine patient symptoms and indication, and rationale for testing, including type of surgery if MPI was performed for preoperative risk assessment.Among patients with ischemic equivalent symptoms but no prior CAD, the pretest likelihood of CAD was determined with the Diamond and Forrester criteria [1].Since Diamond and Forrester tables do not provided estimates for CAD prevalence beyond the age of 69 years, the pretest likelihood of CAD among symptomatic patients aged 70 years or older was determined with use of the highest age category (60– 69 years) in these tables [1].The 10-year risk of ischemic heart disease among asymptomatic patients was determined by the Framingham Risk Score [7].In the original report, the appropriateness of SPECT MPI was determined according to the 2009 AUC for cardiac radionuclide imaging [8].For the purpose of this report, the appropriateness of MPI use was reclassifled according to the 2013 multimodality AUC for the detection and risk assessment of stable ischemic heart disease with use of initially collected clinical data elements [4].Each MPI study was categorized as appropriate, maybe appropriate, or rarely appropriate.To study the impact of rarely appropriate testing on the diagnostic yield of stress MPI, studies with appropriate and maybe appropriate indications were grouped together as being “ appropriate.”The study cohort was further divided into two subgroups based on age: younger than 60 and 60 years or older.An age of 60 years was selected to classify age subgroups since it de flnes the highest age category in the Diamond and Forrester tables [1].
Stress Myocardial Perfusion Imaging
SPECT MPI was performed with a 1-day, rest/stress technetium-99m sestamibi protocol [9].The stress modality (exercise vs.adenosine vs.adenosine with low-level exercise) was selected as clinically appropriate [10, 11].All MPI studies were acquired with use of a dual-head, cardiac SPECT camera(maiCAM-180, Mid-Atlantic Imaging Services,Columbia, MD, Unites States) without attenuation correction [12, 13].SPECT MPI was interpreted with use of QPS/QGS (Cedars-Sinai Cardiac Suite,Los Angeles, CA, USA) by an expert nuclear cardiologist who was blinded to clinical data.Segmental radiotracer activity was semiquantitatively scored on a 17-segment model of the left ventricle with use of a flve-point scoring system (0 for normal to 4 for absent) [14].The segmental scores within the stress and rest scans were summed to generate summed stress scores and summed rest scores, respectively.The summed difference score was calculated from the sum of the segmental difference scores between stress and rest scans.Abnormal MPI was defined as a summed stress score of 4 greater or a summed difference score of 2 or greater.
Statistical Analysis
Statistical analyses were conducted with STATA version 12 (College Station, TX, USA).Student’ sttest was used to analyze differences in continuous data.The chi-square test was used to compare categorical data.Univariate and multivariate logistic regression analyses were performed to determine the predictors of abnormal SPECT MPI.Multivariate analysis was adjusted for clinical covariates of age (by cutoff of 60 years),sex, CAD risk factors (diabetes mellitus, hypertension, dyslipidemia, tobacco use, and family history), known CAD status, and test appropriateness.The multivariable regression model was tested for collinearity between the variables, and none was observed.P < 0.05 was considered to represent statistical significance.
Results
The age of the study population (n= 1511) was 59 ± 13 years, with 57% being males.A total of 664 patients (44%) were older than 60 years.SPECT MPI was abnormal in 190 patients (12.5%), and 271 patients (18%) had a history of known CAD.Ischemia on SPECT MPI was noted in 122 patients(8%).Six-hundred and ninety-nine studies (54%)were performed for indications that were determined to be appropriate (or maybe appropriate).Demographic and clinical data of the study population, stratified by abnormal SPECT MPI, are provided in Table1.Patients with abnormal MPI were older and more often males.They also had a greater prevalence of known CAD, hypertension, and diabetes, and were more often smokers.Indication for stress testing was more often appropriate or maybe appropriate among patients who had abnormal MPI.On univariate logistic regression analysis, all clinical and demographic variables were significantly associated with abnormal MPI, except a history of smoking and a family history of CAD ( Table2).Appropriate indication for testing was also associated with abnormal MPI on univariate analysis.However, on multivariate regression analysis, age of 60 years or greater, male sex, hypertension, diabetes, and known CAD were the only independent predictors of abnormal MPI.Appropriateness of testing was not an independent predictor of abnormal MPI.When age was analyzed as a continuous variable, there was a significant increased risk of abnormal MPI with every 10-year increment in age (odds ratio [OR] 1.52; 95% confidence interval1.24– 1.85; P < 0.0001) after adjustment for all variables ( Table2), including appropriateness criteria.Similar results were noted for ischemia on SPECT MPI, which was independently predicted by age of 60 year or greater, hypertension, and known CAD( Table3).Again, among patients aged 60 years or older, appropriateness of testing did not predict ischemia on SPECT MPI.
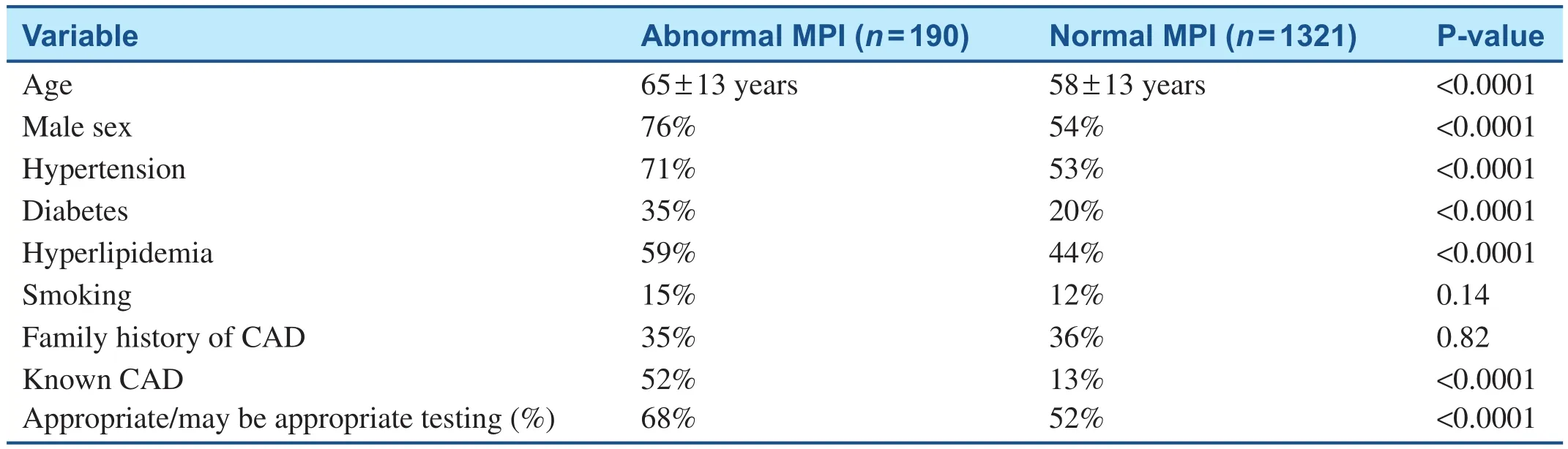
Table1 Distribution of Demographic and Clinical Variables of the Study Population Stratified by Abnormal Single-Photon Emission Computed Tomography Myocardial Perfusion Imaging ( n = 1511).
When the prevalence of abnormal MPI was stratifled by appropriateness of indication and by age,patients older than 60 years of age had a greater prevalence of abnormal MPI regardless of the appropriateness of indication ( Figure1).Among patients tested for a rarely appropriate indication,patients older than 60 years of age had twice the prevalence of abnormal SPECT MPI when compared with patients younger than 60 years of age(14 vs.7%, P = 0.006).The prevalence of abnormal MPI among elderly patients tested for rarely appropriate indications was similar to that among elderly patients tested for appropriate indications (14 vs.19%, respectively, P = 0.14).A similar trend was also noted for ischemia on SPECT MPI ( Figure2 ).Stress-induced myocardial ischemia was more prevalent among the elderly, with no difference in the prevalence of ischemia among the elderly (11%)regardless of appropriateness criteria (P = 1.00).
Discussion
In this study, we report the impact of AUC on the relationship between age and abnormal SPECT MPI.In this broad-based, multisite cohort, application of AUC did not effectively stratify the risk of abnormal MPI or ischemia on MPI among the elderly.We identified a similarly high proportionsof abnormal SPECT MPI and ischemia on SPECT MPI among elderly patients whether testing was performed for an appropriate or a rarely appropriate indication.In contrast, AUC did stratify the risk of abnormal SPECT MPI in patients younger than 60 years of age, as appropriate testing was associated with a greater prevalence of abnormal MPI(12%) when compared with rarely appropriate testing (7%, P = 0.013).However, such a relationship only attained borderline statistical significance for the prevalence of ischemia on SPECT MPI among patients younger than 60 years of age (7.5 vs.5%,P = 0.14).
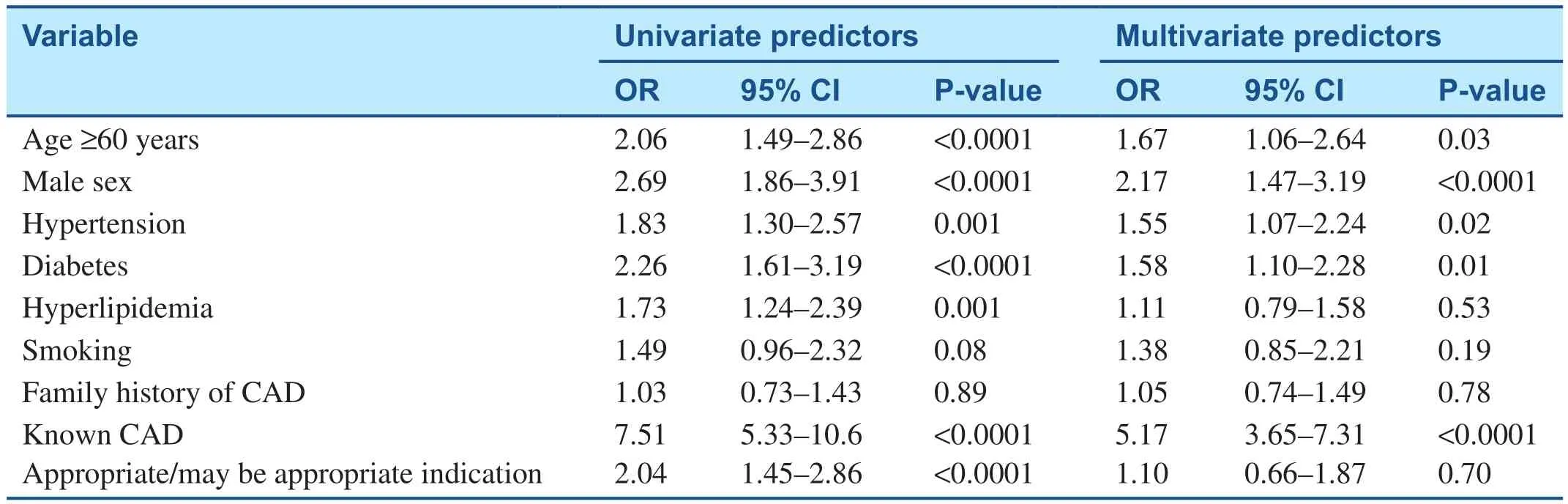
Table2 Predictors of Abnormal Stress Myocardial Perfusion Single-Photon Emission Computed Tomography.
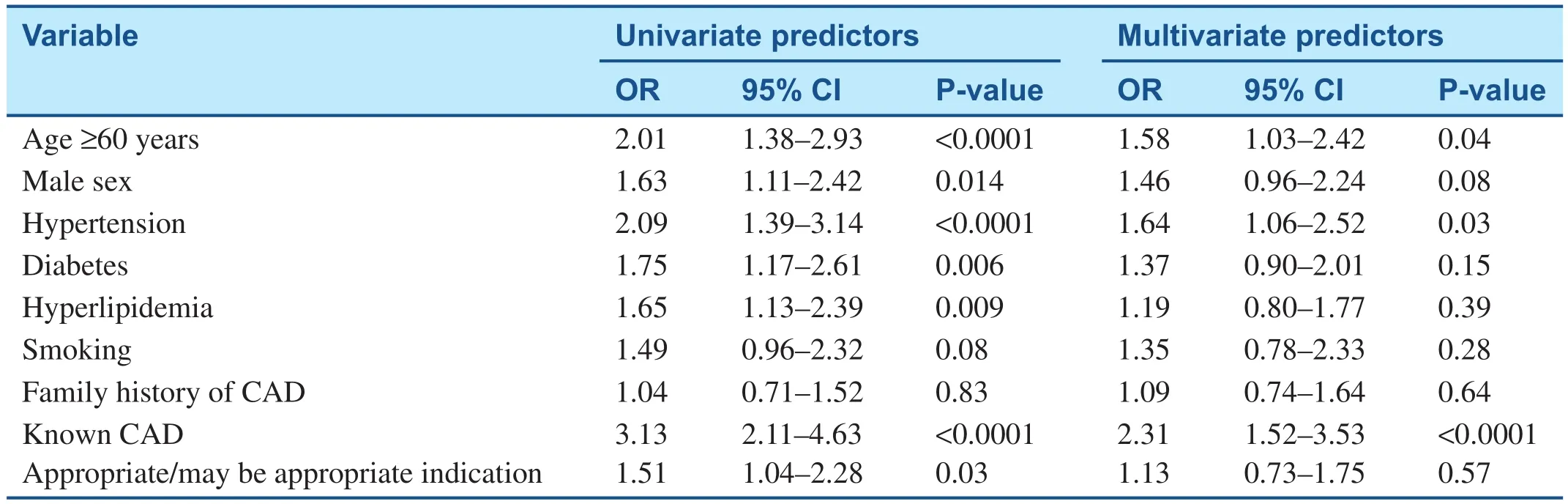
Table3 Predictors of Ischemia on Stress Myocardial Perfusion Single-Photon Emission Computed Tomography.
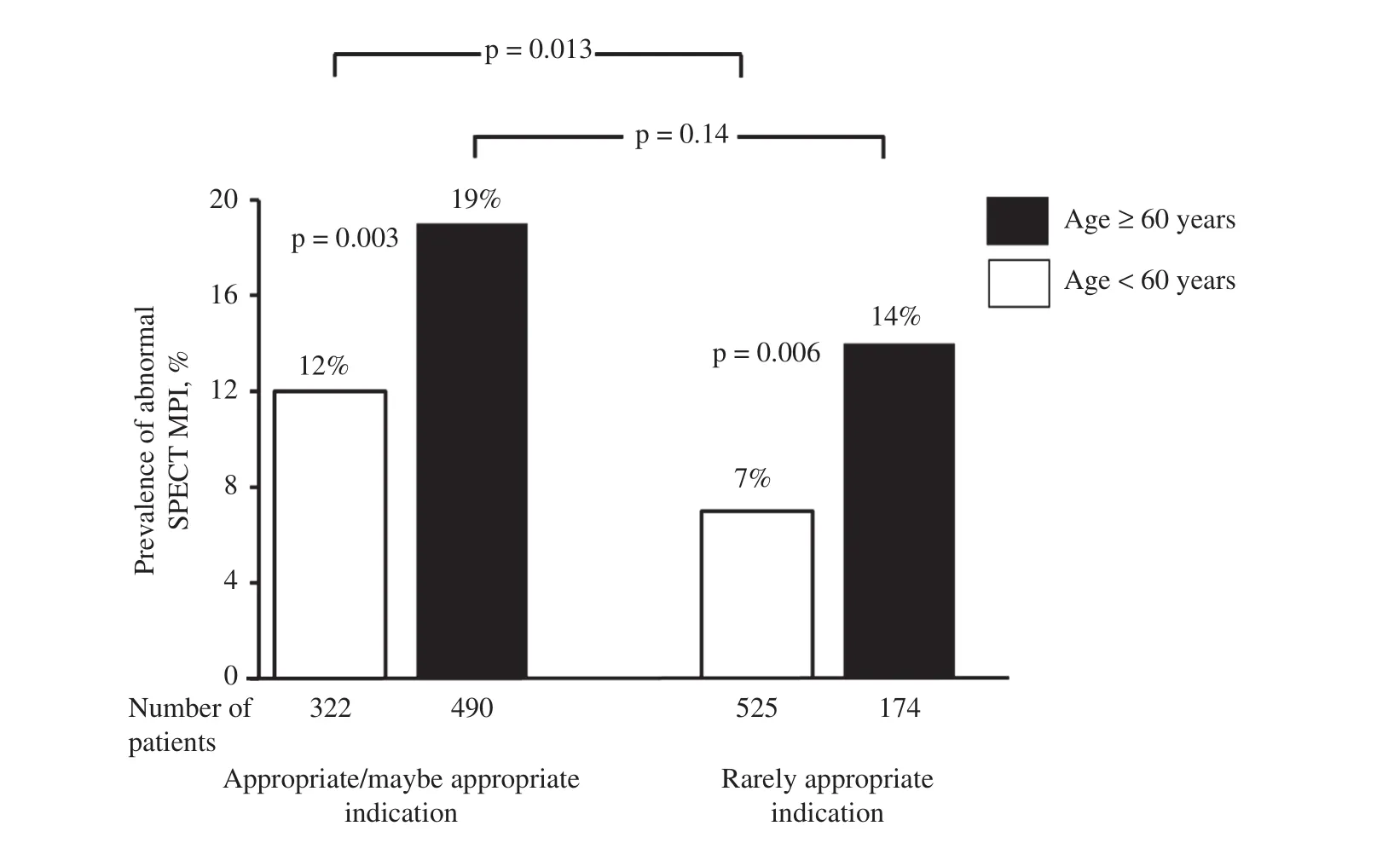
Figure1 Prevalence of Abnormal Stress Myocardial Perfusion Single-Photon Emission Computed Tomography (SPECT)Stratified by Age and Appropriateness of Indication.
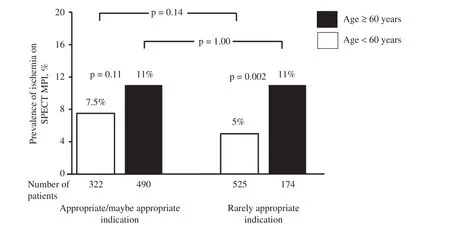
Figure2 Prevalence of Abnormal Stress Myocardial Perfusion Single-Photon Emission Computed Tomography (SPECT)Stratified by Age and Appropriateness of Indication.
AUC are intended to aid in effective application of MPI and improve the value of testing.The yield of testing is an important determinant of value in decision making.AUC suggest the appropriateness of a cardiovascular test for diagnosis of suspected CAD,but do not preferentially recommend one appropriate imaging test over another.Additionally, AUC do not classify the utility of a test by age, which is a strong predictor of CAD.In a study of asymptomatic patients (who would otherwise be rarely appropriate for SPECT MPI) referred for stress testing, increasing age was an independent predictor of ischemia on SPECT MPI [3].Age greater than 74 years was the strongest independent predictor of ischemia(OR 3.65, P = 0.03), in comparison with other independent predictors–smoking (OR 1.72, P = 0.01)and diabetes (OR 1.41, P = 0.001).Although an increasing number of CAD risk factors predicted an increasing prevalence of ischemia, this effect was lost among those aged more than 74 years, suggesting a significantly greater impact of increasing age on myocardial ischemia when compared with other risk factors.Similarly, in a separate study of symptomatic patients undergoing exercise stress MPI, increasing age was an independent predictor of ischemic ECG response, while other CAD risk factors were not predictive [15].
Although AUC do not classify the appropriateness level of an indication for MPI by age, they are likely heavily weighted by age, especially among those with no known CAD.The Diamond and Forrester criteria are often used as a guide for determining the pretest probability of CAD.On the basis of these criteria, the prevalence of CAD increases with age, for both men and women, across typicality of symptoms [1].On the basis of the Diamond and Forrester criteria, the pretest probability of CAD for men and women aged 60 years or older with typical angina is greater than 90%.A similar trend of increasing anatomical CAD on coronary computed tomography angiography with increasing age was reported from the analysis of data from the Coronary CT Angiography Evaluation For Clinical Outcomes: An International Multicenter(CONFIRM) registry [16].A recent pooled analysis of the data from Rule Out Myocardial Infarction/Ischemia Using Computer Assisted Tomography-II(ROMICAT-II) and American College of Radiology Imaging Network-Pennsylvania (ACRIN-PA) studies revealed a significantly greater prevalence of anatomical stenosis among those aged 60 years or older [17].These studies further underscore the fact that the elderly are a high-risk population.Although AUC generally advise against routine testing for rarely appropriate indications, this may not hold true across all age categories, as a substantial proportion of elderly patients tested for rarely appropriate indications in our cohort had abnormal SPECT MPI.Our results do not discount the value of AUC,and among patients younger than 60 years of age application of AUC identifies a significantly higher proportion of abnormal MPI among those tested for an appropriate indication.
Limitations
Our study population represents a relatively low-risk community-based population, and thus is not representative of higher-risk tertiary care center populations.Additionally, the lack of outcome data limits our ability to determine if high prevalence of abnormal SPECT MPI among elderly patients tested for rarely appropriate indications translates into a high rate of cardiovascular outcomes.The prevalence of testing for inappropriate indications is high in our study cohort and is likely not reflective of current practice.However, the study was conducted to investigate the impact of AUC on results of SPECT MPI and not to report adherence rates with AUC.
Conclusions
Age is a strong independent predictor of abnormal SPECT MPI and inducible myocardial ischemia.The value of age in predicting abnormal SPECT MPI is maintained across MPI test appropriateness categories.Appropriate testing identifies a greater prevalence of abnormal MPI in patients younger than 60 years of age, although it does not provide such a diagnostic discrimination among elderly patients.Cautious reliance on AUC is advised when one is considering elderly patients for MPI.
Funding
The original study leading to this cohort was funded by Astellas Pharma Global Development(Northbrook, IL, United States).The present analysis and report was internally funded.
Conflict of Interest
Rami Doukky has received research funding grants from Astellas Pharma (Northbrook, IL, United States).Saurabh Malhotra has no conflicts of interest.
 Cardiovascular Innovations and Applications2019年2期
Cardiovascular Innovations and Applications2019年2期
- Cardiovascular Innovations and Applications的其它文章
- A Tale of Two STEMI’ s
- Adult Congenital Heart Disease in the Veteran Population: A Case-Based Report
- Using 3D-Printed Models to Advance Clinical Care
- Evaluation of the Patient with Incidental Left Ventricular Hypertrophy on Echocardiography
- Practical Clinical Application of Cardiac Computed Tomography– Derived Fractional Flow Reserve
- Imaging Beyond the Angiogram in Women with Suspected Myocardial Infarction and No Obstructive Coronary Artery Disease