
Pregnancy in Congenital Heart Disease:A Review for the General Cardiologist
2018-07-04 06:40KathrynPatrickMDandArwaSaidiMBBChFACCMed2
Kathryn Patrick, MD and Arwa Saidi, MB, BCh, FACC, Med2,3
2Department of Pediatrics, University of Florida, Gainesville, FL 32608, USA
3Department of Internal Medicine, University of Florida, Gainesville, FL 32608, USA
lntroduction
Cardiovascular disease is the leading cause of pregnancy-related deaths in the United States [1].An estimated 4% of all pregnancies in the United States are affected by maternal cardiovascular disease, with 80% of these cases attributed to congenital heart disease (CHD) [2–4].Secondary to improved diagnosis and management of CHD, more women with CHD are reaching reproductive age, and many of these women desire pregnancy.While many pregnant women with CHD will have an uncomplicated pregnancy and delivery, some with more complex cardiac lesions or comorbidities will have an increased risk of maternal and neonatal morbidity and death.Individualized preconception, antepartum, intrapartum, and postpartum management are essential to maximize the potential for a healthy pregnancy with an uncomplicated delivery and postpartum period.
Before Conception
The cardiologist has a unique role in preconception counseling and assessment as many women of reproductive age may receive medical care only from their cardiologist before conception.Counseling women with CHD on the maternal and perinatal risks of pregnancy and the peripartum period should be individualized and occur before conception.Counseling should ideally begin before the onset of sexual activity and focus on either pregnancy planning or safe, reliable contraception.In preparation for pregnancy, maternal risk stratif ication, perinatal risks, genetic assessment, current medications, and potential diagnostic or therapeutic interventions should be addressed.
Maternal Risk Stratification
There is no universally accepted way to classify CHD.However, most classification systems generally describe the anatomic structure or function of the heart.For example, when anatomic structure is being considered, CHD can be described as simple or complex.Simple CHD lesions include uncomplicated atrial septal defects or ventricular septal defects; patent ductus arteriosus; mild pulmonary valve stenosis;or successfully repaired atrial septal defects, ventricular septal defects, patent ductus arteriosus, or total anomalous pulmonary venous connection without recurrent pulmonary vein stenosis or evidence of pulmonary hypertension.Complex CHD lesions include transposition of the great arteries, tetralogy of Fallot,Ebstein anomaly, and Eisenmenger syndrome.
In women of reproductive age, it is important to adopt a more global classification system of CHD that incorporates not only the anatomic structure and function of the heart but also baseline cardiac reserve, the presence of adverse outcome predictors, and comorbid conditions related to CHD.In doing so, one can accomplish more accurate pregnancy risk stratification and maternal and neonatal outcome predictions.This information is essential to counseling women with CHD before and during pregnancy.
Several independent risk factors for adverse cardiovascular outcomes in maternal CHD have been identified (Table 1).However, more useful to patients and clinicians are risk stratification scores incorporating these independent risk factors to predict the risk of adverse cardiovascular events during pregnancy.There are three validated risk stratification systems: the Canadian Cardiac Disease in Pregnancy (CARPREG) risk score,the ZAHARA risk score, and the World Health Organization (WHO) classification of maternal cardiovascular risk.
The CARPREG classification system was fi rst described in 2001, and includes pregnant women with both acquired and CHD (Table 2) [3].The ZAHARA classification system was fi rst described in 2010, and includes only pregnant women with CHD (Table 3) [7].The ZAHARA risk score was validated in subsequent studies and shown to perform better than the CARPREG risk score inmaternal CHD [8].However, both the CARPREG risk score and the ZAHARA risk score have limitations, specifically related to the population of women included in each study.Both studies failed to include adequate numbers of women with severe cardiac disease (i.e., pulmonary hypertension and aortic dilation).Given the low prevalence of these conditions in the study population, these important predictors of adverse maternal outcomes have not always received the attention they deserve.
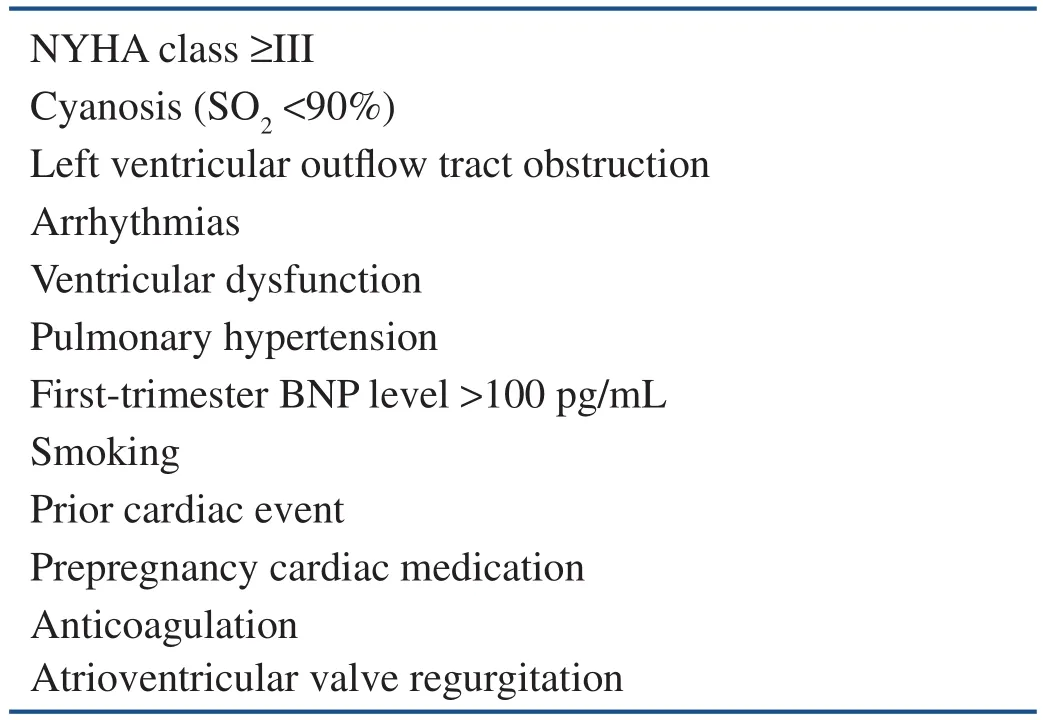
Table 1 Independent Risk Factors for Adverse Cardiac Outcomes in Maternal Congenital Heart Disease [5, 6].
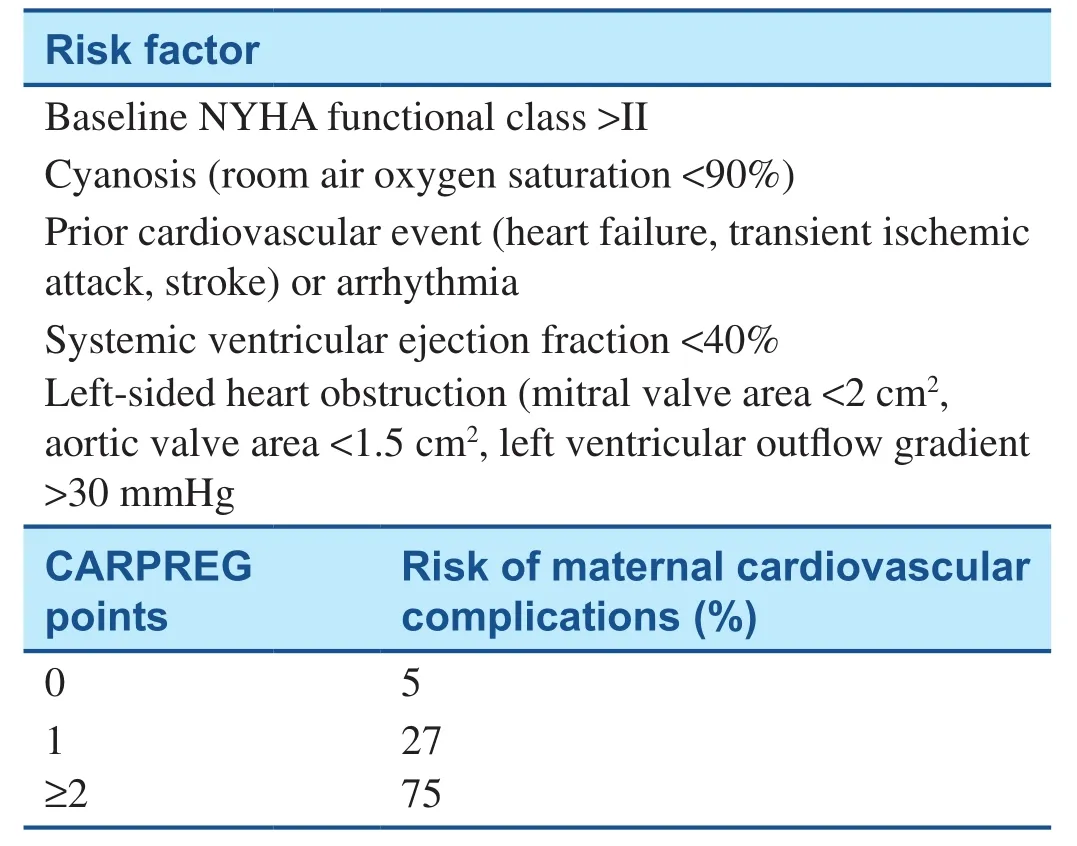
Table 2 Canadian Cardiac Disease in Pregnancy(CARPREG) Risk Score [3].
The complex pregnant population is best addressed by the third classification system.The WHO risk classification system is modified from guidelines on contraception use in heart disease and applies to both acquired CHD and CHD in pregnancy (Table 4) [9].This system describes risk stratification, management recommendations, and pregnancy contraindications, which are all very useful tools when one is counseling women with CHD.Pregnancy contraindications, as defined by the WHO classification system, include pulmonary artery hypertension,severe left ventricular dysfunction, and an aortic root dilatation of greater than 45 mm in patients with Marfan syndrome.In a prospective assessment of the three aforementioned risk classification systems used in maternal CHD, the WHO classification system was found to be the most reliable at predicting adverse maternal cardiovascular events, and is nowrecommended as the preferred risk assessment tool in pregnancy [10].
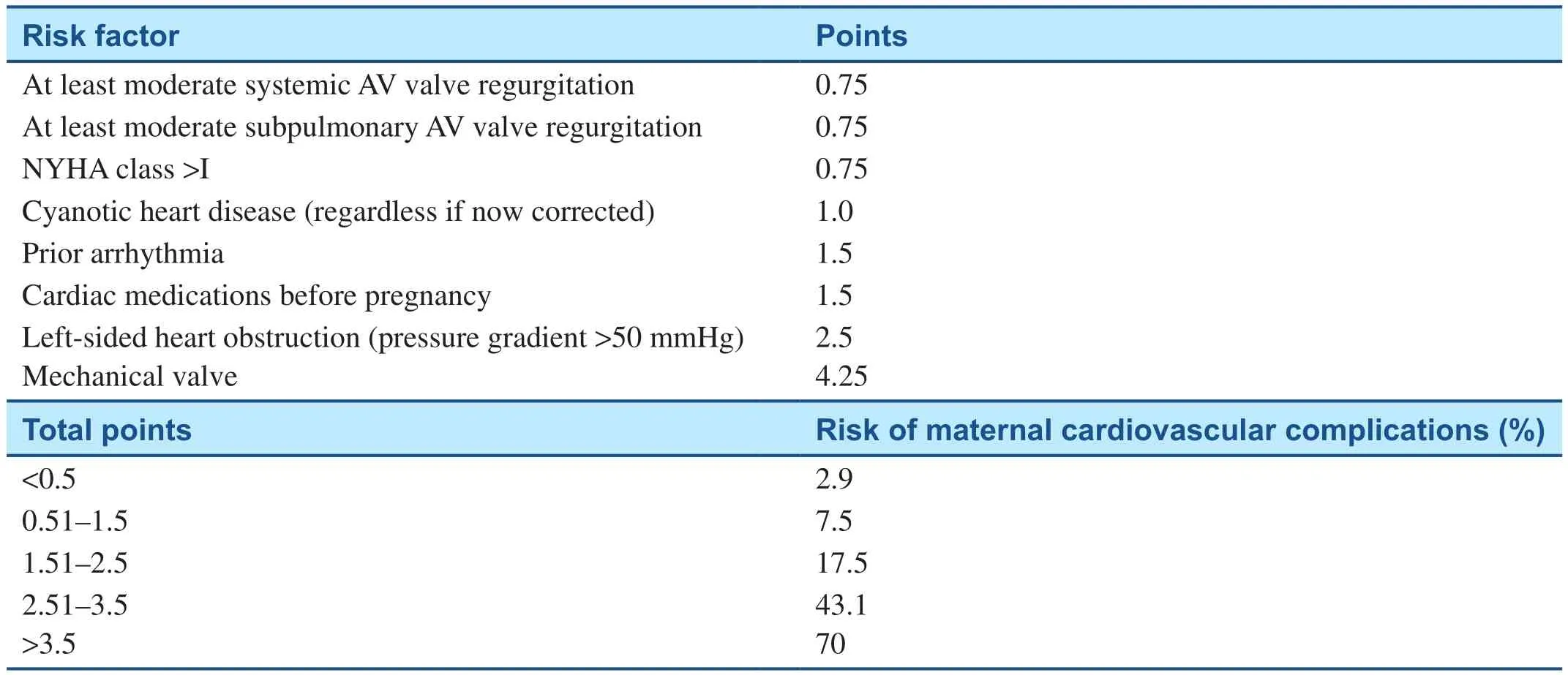
Table 3 ZAHARA Risk Score [7].
Perinatal Risks
Perinatal adverse outcomes are increased in pregnancies complicated by maternal CHD.Fetal adverse outcomes include increased risk of spontaneous miscarriage (15–25%), intrauterine fetal demise (3%),recurrence of CHD, intrauterine growth restriction(4–8%), and preterm birth (10–12% in simple CHD and 22–65% in complex CHD), with 59% of such pregnant women presenting with preterm labor or preterm premature rupture of membranes and up to 41% necessitating a preterm delivery for maternal or neonatal indications [3, 11, 12].Neonatal adverse outcomes include small for gestational age, respiratory distress syndrome, intraventricular hemorrhage,and neonatal death (27.8%).Important maternal predictors of poor neonatal outcomes are subaortic ventricular outflow tract obstruction, cyanosis, and decreased cardiac output (CO).Eisenmenger syndrome portends the highest risk of perinatal death,at 27.7% [11, 13].
Genetic Assessment
A general preconception genetic assessment by the cardiologist is important when women of reproductive age with CHD are being cared for as inheritable causes of CHD can have serious implications on future pregnancy planning.Genetic assessment should include a detailed family history.Familial clustering of CHD and parental features of a syndromic phenotype may suggest an inherited genetic condition.However, an inheritable cause of CHD may also appear de novo in the absence of a significant family history.The recurrence risk of de novo CHD is 3–5% and depends on the type of heart lesion, maternal history, and family history[14].Recurrence risk is increased in the presence of heterotaxy, atrioventricular septal defect, and left ventricular outflow tract obstructions [15].Many inherited genetic conditions associated with CHD are autosomal dominant and have a 50% transmission rate.The most common autosomal dominant syndrome associated with CHD is DiGeorge syndrome,or 22q11.2 deletion syndrome.If an inheritable cause of CHD is suspected, referrals to specialists in genetics and maternal fetal medicine are warranted.
Maternal Cardiac Evaluation
Women with CHD who are planning pregnancy should undergo a thorough cardiac evaluation to determine baseline functional capacity and to assist with risk assessment before conception.Diagnostic evaluation should begin with a complete review ofall maternal medical records, including medical history, surgical history, current and past medications,allergies, recent clinic visits, cardiac imaging procedures, and laboratory studies.Women who are prescribed potentially teratogenic medications or medications with unknown pregnancy safety profiles should be using effective contraception or counseled on discontinuation of these medications before pregnancy.Next, a detailed history of present illness and functional status and a physical examination should be performed.The physical examination should include all vital signs, including oxygen saturation.It is important to not discredit current symptoms or ignore subtle variations in vital signs as both can be important indicators of a change in cardiac status.
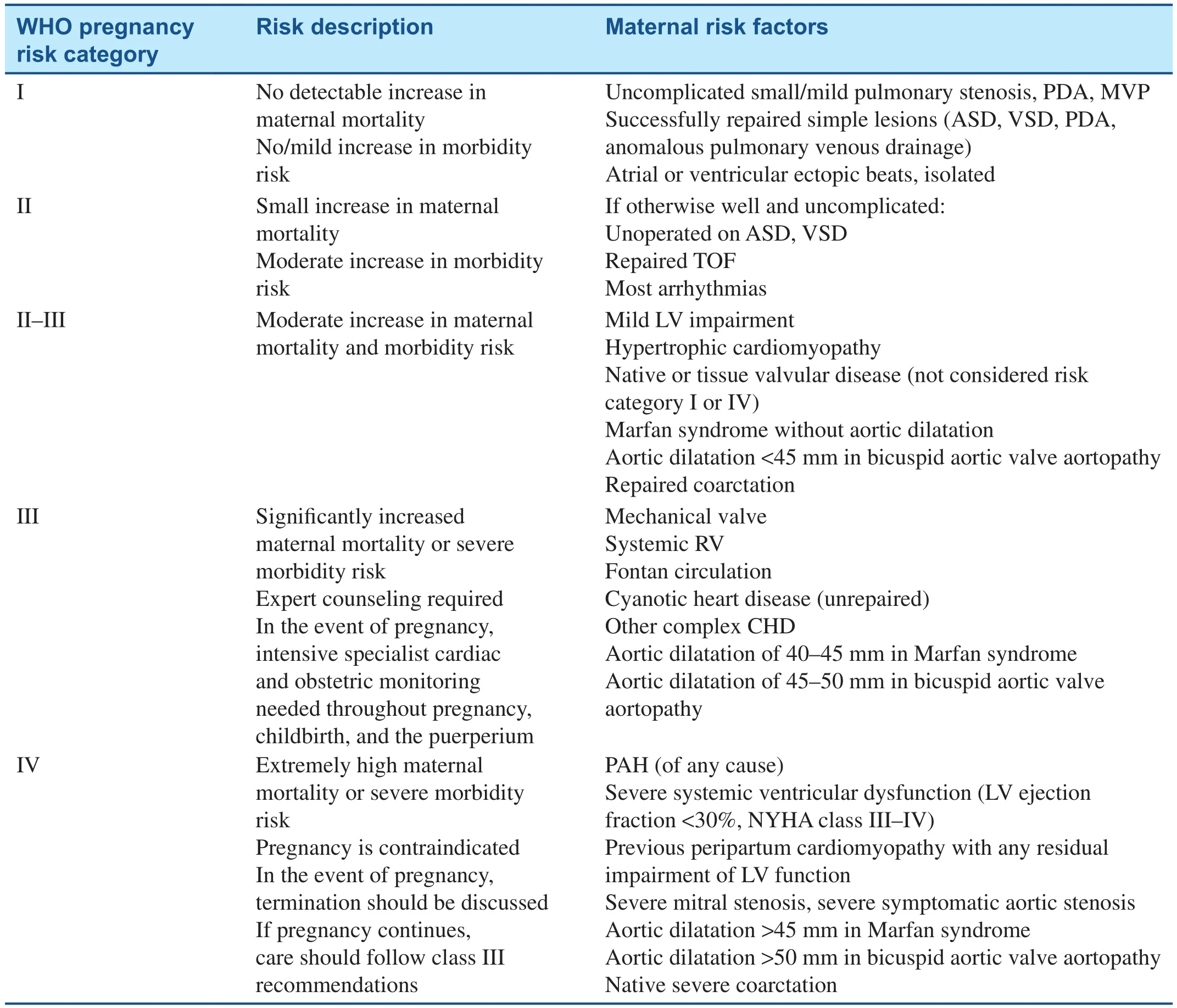
Table 4 Modified WHO Classification of Maternal Cardiovascular Risk [9].
Baseline laboratory testing should include a complete blood count, electrolyte levels, thyroid and liver function tests, and brain natriuretic peptide(BNP) level [5].Baseline ECG and echocardiogram should be performed to identify cardiac arrhythmias and assess baseline cardiac function.To objectively assess exercise capacity and functional capacity,a cardiopulmonary exercise test or exercise stress test can be considered in women with complex congenital cardiac lesions.If there is any concern for pulmonary hypertension as part of a primary process or a sequela of CHD, cardiac catheterization should be performed before pregnancy [14].If there are any significant sequelae of CHD, surgical intervention should also be considered before pregnancy.Although the WHO modified classification is used for risk stratification, the decision is individualized and also based on the woman’s cardiac reserve and cardiac and other medical comorbidities.
Pregnancy
Physiologic Cardiovascular Adaptations in Pregnancy
There are many cardiopulmonary changes that occur in pregnancy to facilitate the growth of the fetus and to prepare the mother for delivery (Figure 1).The hemodynamic changes in pregnancy can be signif icant for women with CHD and may cause symptoms in previously asymptomatic patients.
During pregnancy, maternal blood volume increases by approximately 40%, with peak values occurring at around 32 weeks.The disproportionate increase in plasma volume compared with red cell mass leads to a physiologic dilutional anemia of pregnancy.Hemoglobin concentrations(mean ± standard deviation) in the second and third trimester are 10.9 ± 0.6 g/dL and 12.4 ± 1.0 g/dL,respectively.Maternal colloid oncotic pressure decreases during pregnancy by 12–18% [17].Both a relative decrease in red cell mass and a decrease in colloid oncotic pressure lead to edema and a hypercoagulable state in pregnancy.
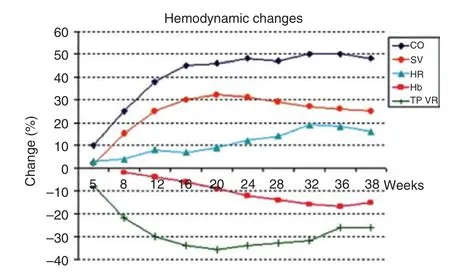
Figure 1 Image copied from Ruys et al.Hemodynamic Changes in Pregnancy [16].
Maternal stroke volume (SV) increases by 30%,and heart rate (HR) increases by 10–20 beats per minute.As such, maternal CO (CO = SV × HR)increases on average by 30–50% and peaks at around 24 weeks.CO is affected by maternal position, with an increase in CO in the left lateral decubitus position when compared with the supine or lithotomy position.Pulmonary vascular resistance and systemic vascular resistance decrease by 30% and 20%, respectively, to accommodate the increased blood volume in pregnancy.The decrease in systemic vascular resistance accounts for the decrease in diastolic blood pressure by 10–15 mmHg, which is most pronounced at the end of the second trimester.After 24–28 weeks’ gestation, the systemic vascular resistance and blood pressure increase slowly,approaching preconception levels by term.Mean arterial pressure (MAP) and central venous pressure are unchanged during the antepartum period.
During labor, blood pressure, HR, SV, CO, and central venous pressure increase.It is important to note that maternal CO during labor can be significantly reduced in the supine position and with epidural anesthesia as both lead to a reduction in preload through compression of the venous system by the gravid uterus and venodilation, respectively.CO is also transiently reduced during the second stage of labor with the Valsalva maneuver and a subsequent decrease in venous return and preload.Although rarely absolutely indicated, operative vaginal delivery and avoidance of the Valsalva maneuver in the second stage of labor can minimize changes in CO in particularly vulnerable patients with critical obstructive lesions.
Immediately following delivery, CO and SV increase by 50% and 60%, respectively, because of decompression of the vena cava and increased venous return.Pulmonary and systemic vascular resistance increase, causing an elevation of MAP.The increase in SV, pulmonary vascular resistance,systemic vascular resistance, and MAP all contribute to the increase in maternal CO from 60% to 80%after delivery to attenuate the effects of a significant decrease in blood volume at the time of delivery.If blood loss is excessive, as with postpartum hemorrhage (i.e.>500 mL for vaginal delivery and>1000 mL for cesarean delivery), SV decreases, with a subsequent increase in HR to maintain adequate CO.The hemodynamic changes characteristic of the postpartum period can persist to some degree for up to 2 weeks after delivery [14].
The physiologic cardiovascular adaptations of pregnancy lead to characteristic signs and symptoms that may complicate the evaluation and monitoring of maternal CHD.Several signs and symptoms of cardiac decompensation can be mistaken for normal, physiologic signs and symptoms in pregnancy.Specifically, weight gain, edema, hyperventilation causing shortness of breath, jugular vein distention,palpable right ventricular impulse, increased fi rst heart sound with persistent splitting of second heart sound, increased cardiac rhythm disturbances such as premature beats and supraventricular tachycardia, and systolic ejection murmurs can all be seen in normal pregnancies.These signs and symptoms can mimic worsening cardiac status in women with CHD and create a clinical conundrum when these patients are being evaluated [14].
Antepartum Management
Ideally, women with CHD should seek prenatal care early in the fi rst trimester or as soon as pregnancy is diagnosed.Depending on the complexity of the lesion, baseline functional status, and presence of comorbidities or sequelae of CHD, many women are advised to receive prenatal care at a tertiary medical center that incorporates maternal fetal medicine, cardiology, anesthesiology, neonatology,genetic counseling, social work, and medical ethics specialties.
Maternal and prenatal care should be coordinated and individualized.A shared decision making model should be used that incorporates patient demographic factors such as social situations and accessibility and proximity to a tertiary medical center for appointments and delivery.In general,low- and moderate-risk patients who live far from a tertiary medical center specializing in CHD in pregnancy may be seen locally by an obstetric specialist for routine prenatal care following consultation with maternal fetal medicine and cardiology subspecialists.If possible, high-risk patients should be seen exclusively at a tertiary medical center specializing in CHD in pregnancy.
The initial obstetric visit with a maternal fetal medicine subspecialist should occur as early as possible and should focus on the timing and location of prenatal visits and ultrasound examinations,genetic counseling and recurrence risk, symptom monitoring and reporting, and delivery planning.The frequency of obstetric visits is individualized and dependent on maternal medical comorbidities,fetal birth defects, and concurrent obstetric complications.Women who are classified as having WHO category IV risk have an unacceptably high risk of maternal death or severe morbidity during pregnancy, and they should be counseled on the option of pregnancy termination and its associated risks.Similarly, patients who have a fetus with a life-threatening anomaly such as a hypoplastic left ventricle should be counseled by a maternal fetal medicine subspecialist and a pediatric fetal cardiologist regarding perinatal surgical options and the option of pregnancy termination.
The initial cardiology visit during pregnancy should include a review of pertinent medical and surgical history, the history of the present illness, a complete cardiovascular examination, and a review of current medications.A comprehensive table of common cardiovascular medications encountered in adult CHD and the risk of these medications during pregnancy and lactation is available in the American Heart Association statement addressing the management of complex CHD in pregnancy[14].Although it is useful to refer to such tables, it is important to take into consideration the individualized risk-to-benef it ratio of a particular medication and use a shared decision making model when one is deciding to continue use of a medication in pregnancy.In general, angiotensin-converting enzyme inhibitors, angiotensin receptor blockers, atenolol,spironolactone, vitamin K antagonists, endothelin receptor antagonists, and statins should be avoided in pregnancy.The need, frequency, and timing of subsequent cardiology clinic visits and diagnostic cardiac evaluation such as ECG and echocardiogram should also be reviewed.The frequency of cardiology visits is individualized and dependent on the specific cardiac lesion, pregnancy risk stratification, presence of cardiac sequelae, and development of symptoms or complications.
Adequate screening and close surveillance of the fetus during pregnancy are essential in pregnancies complicated by maternal CHD.Increasing evidence supports the value of a fi rst-trimester fetal anatomic survey between 11 and 14 weeks,in addition to the conventional second-trimester survey between 18 and 22 weeks [18–20].Early detection of major congenital anomalies allows greater reproductive choice and earlier pregnancy and delivery planning.As 2–18% of pregnancies complicated by maternal CHD are also complicated by fetal CHD, fetal echocardiogram is recommended at around 20–22 weeks [10, 21].Fetal growth assessment may occur as often as every 2 weeks depending on maternal cardiac status and the prior pattern of fetal growth.Routine antenatal testing should always be performed in the setting of fetal growth restriction, maternal CHD associated with increased risk of perinatal death, and other maternal comorbidities.
lntrapartum Management
Most low-risk and clinically stable patients can expect an uncomplicated labor and delivery.With coordinated, thoughtfully planned intrapartum care,many high-risk patients can also expect an uncomplicated labor and delivery.In most situations,vaginal delivery is preferred, and cesarean delivery should be reserved for obstetric reasons.It is often beneficial for high-risk patients to undergo a scheduled induction of labor so as to coordinate care during regular work hours when full staffing is more readily available [22].Regional anesthesia is usually well tolerated in pregnant CHD patients, with appropriate precautions in patients taking aspirin or anticoagulants.With some lesions, such as aortic stenosis and Eisenmenger syndrome, spinal anesthesia is contraindicated secondary to the potential for significant hypotension.In most cases, epidural anesthesia can be used given appropriate precautions to avoid maternal hypotension.Historically, an operative vaginal delivery or “assisted second stage of labor” was recommended in women with CHD to avoid the Valsalva maneuver and the associated increased oxygen consumption, decreased venous return, and decreased CO [23].However, it has become increasingly more common in a clinically stable patient to forego operative vaginal delivery and allow an unassisted second stage of labor unless there are obstetric indications.
Judicious administration of intravenous fl uids to maintain fl uid balance is essential.Extremes of hypovolemia and hypervolemia, as with excessive blood loss and large fl uid boluses, respectively,should be avoided.In patients with right-to-left shunting, continuous pulse oximetry is recommended to monitor hypoxemia.Intravenous bubble fi lters should be used to prevent paradoxical air embolization.Appropriate patients with CHD may benef it from continuous telemetry during labor and delivery, especially those patients with current arrhythmias or reduced ventricular function.An arterial line is rarely needed but may be useful to monitor fl uid shifts in patients with congestive heart failure.Antibiotic prophylaxis against infective endocarditis in pregnant women with CHD before delivery is controversial.However, as neither vaginal nor cesarean deliveries have been directly linked to infective endocarditis, antibiotic prophylaxis is no longer routinely recommended before delivery in pregnant women with CHD [10, 23].
Postpartum Period
The postpartum period is an especially critical time for many women with CHD secondary to extensive fl uid shifts that occur after delivery.Immediately following delivery, an “autotransfusion” of about 500 mL of blood from the contracted uterus to the systemic circulation increases blood volume, SV,and CO.This change in intravascular volume can lead to lethal cardiopulmonary complications in the postpartum period, including arrhythmias, hypoxemia, and thromboembolism.Because of this,postpartum diuresis should be considered in many patients with CHD.Depending on the underlying cardiac lesion and clinical stability, patients may need close invasive hemodynamic monitoring in an intensive care unit setting for 24–48 hours postpartum.It is important to remember that the hemodynamic changes of pregnancy can persist for up to 8 weeks postpartum.During the postpartum evaluation, the risk of future pregnancy and contraception should be discussed with the patient.Furthermore,patients may need continued therapy with vitamins containing iron because iron-deficiency anemia may not be well tolerated in women with sequelae from their cardiac surgical procedures or mild cardiac dysfunction.
Maternal Long-Term Prognosis
The effects of pregnancy on the progression of maternal cardiac disease and long-term prognosis are unclear for many congenital heart lesions.However,the effects of pregnancy on some cardiac lesions have been described.For example, in the setting of maternal tetralogy of Fallot, some investigators suggest no effects of pregnancy on clinical status or biventricular function [24].However, others suggest a persistent dilatation of the subpulmonary ventricle,unfavorable right ventricular remodeling, increase in end-diastolic volume, and preserved right ventricular systolic function following pregnancy in those with repaired tetralogy of Fallot [24, 25].
Conclusion
In general, most women with CHD tolerate pregnancy well.However, it is imperative to identify and appropriately counsel those women with complex cardiac lesions or significant cardiac sequelae, in whom pregnancy is contraindicated, before pregnancy.Even when pregnancy is not contraindicated, preconception contraception counseling and pregnancy planning should be routinely addressed by both the obstetrician and the cardiologist.Furthermore, diagnostic cardiac evaluation and possible surgical interventions should be considered before pregnancy.Following conception,improved maternal and perinatal outcomes can be achieved with a coordinated multidisciplinary team approach, a shared decision making model, adherence to appropriate antepartum and postpartum management principles, and awareness of patientspecific labor and delivery precautions.
Conflict of lnterest
The authors declare no conflict of interest.
REFERENCES
1.Centers for Disease Control and Prevention.Pregnancy mortality surveillance system.Retrieved September 18, 2017, from: https://www.cdc.gov/reproductivehealth/maternalinfanthealth/pmss.html.
2.Gandhi M, Martin SR.Cardiac disease in pregnancy.Obstet Gynecol Clin N Am 2015;42:315–33.
3.Siu SC, Sermer M, Colman JM,Alvarez AN, Mercier LA, Morton BC, et al.Prospective multicenter study of pregnancy outcomes in women with heart disease.Circulation 2001;104(5):515–21.
4.Curtis Sl, Marsden-Williams J,Sullivan C, Sellers SM, Trinder J,Scrutton M, et al.Current trends in the management of heart disease is pregnancy.Int J Cardiol 2009;133:62–9.
5.Pieper PG.Pre-pregnancy risk assessment and counseling of the cardiac patient.Neth Heart J 2011;19:477–81.
6.Song YB, Park SW, Kim JH,Shin DH, Cho SW, Choi JO,et al.Outcomes of pregnancy in women with congenital heart disease: a single center experience in Korea.J Korean Med Sci 2008;23(5):808–13.
7.Drenthen W, Boersma E, Balci A, Moons P, Roos-Hesselink JW,Mulder BJ, et al.Predictors of pregnancy complications in women with congenital heart disease.Eur Heart J 2010;31:2124–32.
8.Balci A, Sollie-Szarynska KM,van der Bijl AG, Ruys TP, Mulder BJ, Roos-Hesselink JW, et al.Prospective assessment of pregnancy risk estimation models in women with congenital heart disease.Eur Heart J 2010;31:615–5.
9.Thorne S, MacGregor A, Nelson-Piercy C.Risks of contraception and pregnancy in heart disease.Heart 2006;92:1520–5.
10.Regitz-Zagrosek V, Blomstrom Lundqvist C, Borghi C, Cifkova R,Ferreira R, Foidart JM, et al.ESC guidelines on the management of cardiovascular diseases during pregnancy: the Task Force on the Management of Cardiovascular Diseases During Pregnancy of the European Society of Cardiology.Eur Heart J 2011;32:3147–97.
11.Khairy P, Ouyang DW, Fernandes SM, Lee-Parritz A, Economy KE,Landzberg MJ.Pregnancy outcomes in women with congenital heart disease.Circulation 2006;113:517–24.
12.Canobbio MM, Mair DD, van der Velde M, Koos BJ.Pregnancy outcomes after the Fontan repair.J Am Coll Cardiol 1996;28:763–7.
13.Drenthen W, Pieper PG, Roos-Hesselink JW, van Lottum WA,Voors AA, Mulder BJ, et al.Outcome of pregnancy in women with congenital heart disease: a literature review.J Am Coll Cardiol 2007;49:2301–11.
14.Canobbio M, Warnes CA, Aboulhosn J, Connolly HM, Khanna A, Koos BJ, et al.Management of pregnancy in patients with complex congenital heart disease.A scientific statement for healthcare professionals from the American Heart Association.Circulation 2017;135:e5–87.
15.Gill HK, Splitt M, Sharland GK,Simpson JM.Patterns of recurrence of congenital heart disease: an analysis of 6640 consecutive pregnancies evaluated by detailed fetal echocardiography.J Am Coll Cardiol 2003;42:923–9.
16.Ruys T, Cornette J, Roos-Hesselink J.Pregnancy and delivery in cardiac disease.J Cardiol 2013;61:107–12.
17.Robertson EG, Cheyne GA.Plasma biochemistry in relation to oedema of pregnancy.J Obstet Gynaecol Br Commonw 1972;79:769–76.
18.D’Ottavio G, Meir YJ, Rustico MA, Pecile V, Fischer-Tamaro L,Conoscenti G, et al.Screening for fetal anomalies by ultrasound at 14 and 21 weeks.Ultrasound Obstet Gynecol 1997;10:375–80.
19.Whitlow BJ, Chatzipapas IK,Lazanakis ML, Kadir RA,Economides DL.The value of sonography in early pregnancy for the detection of fetal abnormalities in an unselected population.Br J Obstet Gynaecol 1999;106:929–36.
20.Iliescu D, Tudorache S, Comanescu A, Antsaklis P, Cotarcea S, Novac L, et al.Improved detection rate of structural abnormalities in the fi rst trimester using an extended examination protocol.Ultrasound Obstet Gynecol 2013;42:300–9.
21.Foley M, Strong TH, Garite TJ.Obstetric intensive care manual.4th ed.New York: McGraw-Hill Education; 2014.
22.American College of Obstetricians and Gynecologists.ACOG committee opinion no 560: medically indicated late-preterm and earlyterm deliveries.Obstet Gynecol 2013;121:908–1010.
23.Waksmonski C, Foley MR.Pregnancy in women with congenital heart disease: general principles.Retrieved November 14, 2016,from UpToDate: https://www.uptodate.com/contents/pregnancyin-women-with-congenital-heartdisease-general principles?source=s e a r c h_r e s u l t&s e a r c h=c o n g e n it a l%2 0 h e a r t%2 0 disease%20in%20pregnancy&.
24.Uebing A, Arvanitis P, Li W, Diller GP, Babu-Narayan SV, Okonko D,et al.Effect of pregnancy on clinical status and ventricular function in women with heart disease.Int J Cardiol 2010;139:50–9.
25.Egidy Assenza G, Cassater D,Landzberg M, Geva T, Schreier J, Graham D, et al.The effects of pregnancy on right ventricular remodeling in women with repaired tetralogy of Fallot.Int J Cardiol 2013;168:1847–52.
 Cardiovascular Innovations and Applications2018年2期
Cardiovascular Innovations and Applications2018年2期
- Cardiovascular Innovations and Applications的其它文章
- Pulmonary Arterial Hypertension Medical Management of the Adult Patient with Congenital Heart Disease
- The Pulmonary Hypertension Story
- The Surgical Management of Ebstein Anomaly
- Evaluation of Left Ventricular Systolic Function after Pulmonary Valve Replacement Using Cardiovascular Magnetic Resonance lmaging
- Atrial Arrhythmias lncluding Atrial Fibrillation in Congenital Heart Disease: Mechanisms,Substrate ldentification and lnterventional Approaches
- Heart Transplantation for Adult Congenital Heart Disease: Overview and Special Considerations