
Atrial Arrhythmias lncluding Atrial Fibrillation in Congenital Heart Disease: Mechanisms,Substrate ldentification and lnterventional Approaches
2018-07-04 06:40:04JeroldShinbaneandPhilipChang2DivisionofCardiovascularMedicineKeckSchoolofMedicineoftheUniversityofSouthernCalifornia50SanPabloStreetSuite32290033LosAngelesCAUSA
Jerold S.Shinbane and Philip M.Chang2Division of Cardiovascular Medicine, Keck School of Medicine of the University of Southern California, 50 San Pablo Street,Suite 322, 90033 Los Angeles, CA, USA
2Congenital Heart Center, Departments of Pediatrics and Internal Medicine, University of Florida College of Medicine,1600 SW Archer Road, PO Box 100296, 32610 Gainesville, FL, USA
lntroduction
Long-term survival for patients with congenital heart disease (CHD) has dramatically improved thanks to tremendous advances and improvements in pediatric and young adult care.A significant population of adults with CHD now exists, with adults outnumbering children with CHD, as well as a rising median age of adult survivors with severe forms of CHD [1–3].Pediatric patients with CHD are expected to survive to adulthood, and adult CHD (ACHD) management has even embraced geriatric care issues for older patients with CHD.Arrhythmias remain a significant long-term complication for CHD survivors, impacting both morbidity and mortality.Furthermore, arrhythmias such as atrial fi brillation (AF), which previously were not commonly tied to CHD, are increasing in prevalence among CHD survivors because of the natural epidemiology of the arrhythmia itself as well as the evolving sequelae in an aging ACHD population.
Mechanisms and Substrates for Atrial Arrhythmias in CHD
AF in the setting of CHD is epidemiologically and mechanistically different from that encountered in the general population.The arrhythmia occurs at younger ages in patients with CHD, where it is typically observed in the setting of organized atrial arrhythmias that degenerate to AF, and can progress rapidly to persistent or permanent forms of AF [4–6].More than half of patients with severe CHD who reach the age of 18 years have atrial arrhythmias by the age of 65 years, and have a significant increase in morbidity and mortality compared with those ACHD patients without atrial arrhythmias [7].
A spectrum of CHD substrates exists, contributing to a substantial heterogeneity in the development and presentation of atrial tachyarrhythmias in CHD (Figure 1).Structural disease in ACHD extends from single to multiple anomalies and exists in the native unoperated on or procedurally/surgically palliated or corrected states.Palliated and corrected forms of CHD differ on the basis of the specific cardiovascular substrate and the specific procedural/surgical techniques used in different eras of management.These then contribute to great differences with regard to anatomic and pathophysiologic sequelae following previous interventions.Common sequelae in adults with previous surgery include pulmonary regurgitation in the setting of previous repair of dysfunctional right ventricular outflow tracts, development of cardiomyopathy in the setting of congenitally or surgically corrected transposition of the great arteries, and cardiomyopathy following staged palliation among the spectrum of single-ventricle defects.Valvular and conduit dysfunction, ventricular dysfunction, and hemodynamic abnormalities result in secondary electrophysiologic changes in atrial and ventricular myocardium.Furthermore, incisional scars, suture lines, patch materials, and myocardial fi brosis create substrates that support a host of electrophysiologic abnormalities.
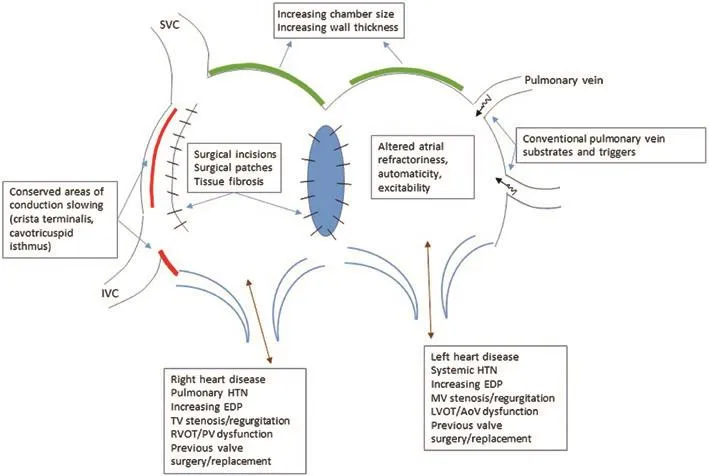
Figure 1 Structural, Anatomic, Electrophysiologic, and Hemodynamic Contributors to the Progressive Risk and Development of Atrial Arrhythmias in Patients with CHD.
The potential substrates and mechanisms of AF initiation and perpetuation are multiple, complex,and incompletely elucidated.The development of a primary atrial myopathic process in CHD has many potential causes, including abnormal atrial morphologic, histologic, pathophysiologic, and electrophysiologic features.The interplay of factors includes atrial myopathic structural changes associated with atrial myocardial hypertrophy,inflammation, and macroscopic and microscopic fi brosis.Histopathologic evidence of atrial fi brosis is typically seen in CHD patients with AF [8].Total atrial conduction time derived from tissue Doppler imaging in ACHD patients is associated with the development of atrial arrhythmias [9].In addition to CHD-specific factors, recognized contributors to AF in the structurally normal heart are also likely to be at play to drive the development of AF in CHD.These include factors such as premature atrial contractions and atrial tachycardia triggers emanating from pulmonary vein and atrial foci, degeneration to AF from stabler supraventricular tachycardias(SVT), atrial anatomy and electrophysiology associated with rotors, vagal and sympathetic autonomic influences, activation of the renin-angiotensinaldosterone system, and significant bradycardia and pauses [10].The contribution of incisional scars in the atria from prior congenital cardiac surgery to the development of macroreentrant atrial tachyarrhythmias is also a recognized concomitant arrhythmia as well as an arrhythmic contributor to AF in CHD.Postoperative incisional intraatrial reentrant tachycardia (IART) circuits develop in viable atrial myocardium with heterogeneous conduction properties surrounding incisional scars and other fi brous structures, which act as conduction barriers [11].Finally,ventricular dysfunction, the complexity of CHD anomalies, and increasing age all augment the risk of supraventricular arrhythmias, including AF and atrial fl utter, in CHD survivors [12].The combined impact of incisional scars, abnormal hemodynamics with volume and pressure loading, atrial chamber dilatation and increases in atrial wall thickness and distribution of fi brosis results in a highly dynamic and continuously changing atrial substrate that is highly predisposed to arrhythmias.
The spectrum of atrial arrhythmias that are commonly associated with and can lead to AF include focal atrial tachycardias, typical cavotricuspid isthmus–dependent atrial fl utter, and atypical and incisional reentrant atrial fl utters [13].Depending on the specific CHD anatomy and pathophysiology, the atrial arrhythmias can involve the right atrium, the left atrium, or both atria and can encompass single or multiple arrhythmia mechanisms, predominantly with macroentrant and microreentrant mechanisms[14].From a simplistic perspective, patients with left-sided defects or who have had palliative surgery for CHD are thought to be more prone to develop AF, while IART occurs more commonly in the right atrium [13, 15].In cases of concomitant AF and IART, ACHD patients with right-sided anomalies had a higher arrhythmia burden over their lifetime than patients with left-sided anomalies, while incidence of stroke, heart failure, and mortality were comparable [16].In the setting of CHD with right atrial overload, atrial myopathy as evidenced by histologic assessment of structural remodeling and fi brosis is associated with the presence of supraventricular arrhythmias [17].
Macroreentrant atrial arrhythmias are seen across a broad spectrum of CHD types, including atrial septal defects (ASDs), single-ventricle defects,transposition of the great arteries, and tetralogy of Fallot [18].Given the frequent involvement of the cavotricuspid isthmus in typical atrial fl utter in the structurally normal heart, it should not be surprising that it is also frequently involved in IART with CHD.Most IART circuits in CHD patients on electrophysiologic study were cavotricuspid isthmus–dependent macroreentrant circuits, followed by circuits involving incisional scars [19].Successful catheter ablation was achieved in both of these settings [20].Furthermore, cavotricuspid isthmus–dependent fl utter and scar-associated macroreentry often occur in the same patient, warranting careful testing and mapping to appropriately differentiate and ablate both substrates [21].In right-sided CHD, there was a higher incidence of cavotricuspid isthmus–dependent circuits, but a higher incidence of postablation recurrence for non-cavotricuspid isthmus–dependent circuits [22].Other mechanisms of IART have been described in specific patient subsets, such as pericaval reentry in Fontan patients [23].Given the high incidence of cavotricuspid isthmus–associated macroreentry, some authors suggest that surgical incisions in the right atrium at the time of repair should be extended to the inferior vena cava as a primary approach to the prevention of IART [24].While most arrhythmias that occur late after surgical repair of CHD are macroreentrant, some are focal atrial tachycardias that require alternative strategies for ablation[25].Automaticity is often the mechanism in these cases; however, nonautomatic and microreentrant varieties exist, and can be differentiated on the basis of features of arrhythmia inducibility and termination properties as well as dense and detailed substrate mapping [26].There are overlapping substrates, which results in both atrial tachycardia and AF.Chronic and persistent atrial tachycardias can cause progressive atrial myopathy that then results in AF development.Primary progressive atrial myopathy manifests itself as IART initially but further progresses to confer increased risk of AF with time.
Given the often compromised hemodynamics in ACHD, the presence of AF can potentially cause symptoms, hemodynamic detriment, or even death.Deleterious hemodynamic effects of atrial arrhythmias during exercise may be significant in ACHD [27].Clinical variables associated with increased mortality in the setting of atrial arrhythmias and ACHD include poor functional class,single-ventricle physiology, pulmonary hypertension, and valvular heart disease [28].The association of AF with lethal ventricular arrhythmias is a rare but well-appreciated complication in the setting of Wolff-Parkinson-White syndrome.Wolff-Parkinson-White syndrome is associated with certain forms of CHD and structural heart disease,including Ebstein anomaly and hypertrophic cardiomyopathy, which is likely related to the structural and myocardial abnormalities in the primary conditions themselves giving rise to abnormal, and sometimes multiple, atrioventricular connections[29, 30].Alternatively, Wolff-Parkinson-White syndrome is rarely an incidental cause of arrhythmias in CHD patients.Among patients with palliated single-ventricle CHD, Correa et al.[31] noted that accessory pathway–mediated SVT occurred in four of 52 patients, with Wolff-Parkinson-White syndrome noted in two patients (3.8%).Neither patient experienced syncope or documented rapidly conducted atrial arrhythmias, and both had pathway refractory periods of 280 ms, which would not be considered to carry concerning risk of ventricular arrhythmia potential in the setting of AF.A recent publication noted no increased risk of death among hypertrophic cardiomyopathy patients with Wolff-Parkinson-White syndrome compared with those without Wolff-Parkinson-White syndrome[32].In the setting of Wolff-Parkinson-White syndrome, ablation of the accessory pathway is often associated with cure of AF, most likely due to the eradication of reentrant SVTs utilizing the pathway that degenerate to AF [33].However, this may not be the same in scenarios of AF in CHD, where the development of AF is complex and multifactorial and likely not linked only to the presence of Wolff-Parkinson-White syndrome.
The epidemiology, incidence, and prevalence of the spectrum of atrial arrhythmias, including AF, differ according to specific CHD types, prior surgical or percutaneous treatment, and residual and ongoing structural and functional sequelae.Certain substrates are recognized to be associated with a higher incidence of atrial arrhythmias, including large and late repaired or unrepaired ASDs, Ebstein anomaly,and single-ventricle CHD following Fontan palliation particularly those with atriopulmonary connections [34].
Atrial Arrhythmias in Specific Forms of CHD
While the risk of AF in CHD involves a complex interplay between CHD type, repaired status,acquired histopathologic and electrophysiologic derangements secondary to past surgery, and hemodynamic abnormalities, as well as increasing age and cumulative time of survivorship with CHD,its development and incidence have been studied in specific CHD types.Traditionally, AF has been associated with primary left-sided defects, and particularly those that result in chronically elevated left atrial or pulmonary venous pressures, leading to chamber dilation and wall thickening and fi brosis, along with common AF triggers involving the pulmonary veins.However, the potential for AF theoretically exists across all types of CHD, owing to recognized and relatively conserved risk factors across a broad spectrum of defect types [5].
In the setting of ASDs, longer times before defect closure appear to be strongly associated with the development of atrial arrhythmias in general, including AF.Age at the time of surgical repair greater than 25 years was a predictor of AF [35].Among adult ASD patients, those with atrial arrhythmias tended to be older and, while the incidence of atrial fl utter decreased after surgery,the incidence of AF did not change [36].The coassociation of atrial fl utter and AF following ASD repair also appears to involve overlapping mechanisms.In IART associated with ASD repair, cavotricuspid isthmus–dependent atrial fl utter was most common, followed by atriotomy-dependent fl utter and double loop atrial fl utter, respectively.Owing to the substantial changes to the atrial myocardium in the setting of a long-standing atrial-level shunt as well as those incurred following surgical repair, the morphology of the fl utter waves on surface ECG may appear atypical even in cavotricuspid isthmus–dependent circuits [37].The mechanism did not depend on whether the repair was performed with a primary suture or a patch repair approach.AF in these settings appears to involve both right and left atrial substrates, with right atrial reentrant and focal activation from the right atrium in patients with paroxysmal AF, and multifocal activation from pulmonary veins and the posterior left atrium as well reentrant left atrial mechanisms in patients with persistent AF [38].
Atrial tachyarrhythmias, including AF, are the most common long-term sequelae among survivors of single-ventricle palliation.The presence of atrial tachyarrhythmias was a strong predictor of morbidity and mortality among Fontan patients[39].Prophylactic atrial arrhythmia surgery to prevent the development of IART in Fontan patients has been proposed along with aggressive arrhythmia surgery at the time of Fontan conversions to reduce the future burden of atrial arrhythmias and their associated impact on long-term morbidity and mortality [40–42].
Cavopulmonary connections culminating in the Fontan operation constitute the current approach to palliation.Since its early development and application in the late 1970s, the Fontan operation has undergone various modifications.Regardless of the form of the Fontan operation, atrial arrhythmias remain a common long-term problem, particularly as patients continue to age and because of a dynamic and progressive atrial myopathic process in these patients [43].While arrhythmia incidence is highest among classic atriopulmonary Fontan patients,this may be less predominantly related to the Fontan operation type, with a larger contribution of longer duration of follow-up and sequelae related to longstanding hemodynamic abnormalities and singleventricle dysfunction [44–46].
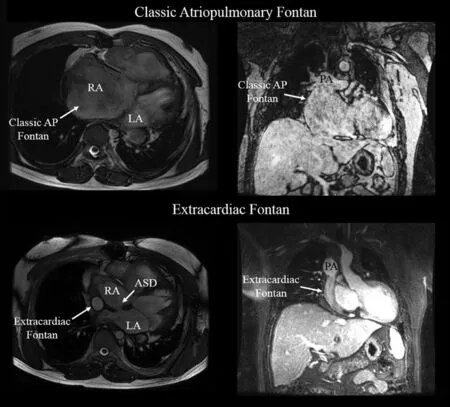
Figure 2 Cardiac MRI Frames Highlighting the Anatomic Differences Between Classic Atriopulmonary and extracardiac Fontan variants.
Lateral tunnel and extracardiac Fontan operation types have a perceived advantage with regard to arrhythmia risk, attributed to less atrial dissection,less long-term atrial chamber enlargement and distortion, and improved mechanical functionality of the Fontan conduit (Figure 2).However, a truly comparable cohort of lateral tunnel or extracardiac conduit variants is lacking in terms of the duration of follow-up in comparison with classic Fontan patients.In adult Fontan patients, IART appears to be the most common atrial arrhythmia, followed by combined IART and AF, and then AF alone,despite the evolution of surgical approaches to the Fontan procedure [47].The onset of arrhythmias also occurs fairly quickly following the Fontan procedure, with 50% of patients developing atrial tachycardia or AF within 10 years, increasing to 100% at 26 years of follow-up [48].In a recent single-center experience, up to 40% of Fontan patients had IART by the age of 25 years [49].Several additional factors also appear to augment arrhythmia risk, including several features that even predate Fontan completion among singleventricle patients.The presence of significant atrioventricular valve regurgitation, even before Fontan completion, was associated with a higher incidence of atrial fl utter [50].Inducibility of IART was greater in female single-ventricle patients and patients who were older at the time of secondstage palliation or pre-Fontan evaluation [51].The presence of atrial isomerism appeared to be associated with an increased risk of atrial arrhythmias following Fontan completion [52].
Sinus node dysfunction and the need for atrioventricular valve repair are frequently present among single-ventricle patients with atrial isomerism, and were predictors of future atrial arrhythmias in these patients as well.Assessment of right atrial histopathologic features 7 years after total cavopulmonary surgery demonstrated atrial intimal thickening,smaller myocardial cell size, and interstitial fi brosis[53].These chronic and progressive changes create atrial substrates with altered electrophysiologic properties with variable conduction times and refractoriness.The finding of significantly prolonged P wave duration Fontan patients with atrial arrhythmias compared with those without them is evidence of this histopathologic-electrophysiologic link [54, 55].
In tetralogy of Fallot, ventricular arrhythmias and sudden death risk are frequently discussed, but atrial arrhythmias, including AF, are more commonly seen.Chronic right ventricular dysfunction related to outflow and pulmonary arterial stenosis and/or pulmonary regurgitation is considered a prominent contributor to right atrial dysfunction.Elevations in right ventricular fi lling pressures and the presence of significant tricuspid insufficiency can contribute to right atrial chamber dilation and histopathologic changes in response to these chronic hemodynamic derangements.In addition,atrial incision and dissection at the time of surgical repair further contributes to a primary atrial myopathic process [56–60].The presence of significant left ventricular diastolic dysfunction is recognized as a risk factor for ventricular arrhythmias and sudden death, and may be a contributor to left atrial dysfunction as well [61, 62].
Among patients with repaired transposition of the great arteries, atrial arrhythmias are most frequently encountered in patients who have undergone atrial switch operations.Extensive atrial dissection,suture lines, and subsequent scarring and fi brosis are considered the dominant contributors to the dysfunctional atrial substrate that is prone to both tachyarrhythmias and bradyarrhythmias.In addition,the chronic hemodynamic perturbations secondary to systemic right ventricular dysfunction result in altered and increased atrial baffle pressures, chamber dilatation, and histopathologic changes.The incidence of atrial tachyarrhythmias following atrial switch operations has been reported to be as high as 34% with long-term follow-up, and even up to nearly 50% in some single-center longitudinal studies [63, 64].The risk of IART appears to differ depending on the type of atrial switch operation,with the risk being 16% in Mustard patients versus 6.1% in Senning patients in published long-term follow-up experience [65].Regardless of the operation type, the development of IART was associated with worse prognosis.Furthermore, the development of IART in this form of repaired CHD is associated with abnormal atrial and ventricular electromechanical function and risk of sudden cardiac death,considered in part to be due to rapid atrioventricular nodal conduction of atrial tachyarrhythmias resulting in ventricular arrhythmias [66–68].
Eisenmenger syndrome highlights a unique combination and culmination of contributors to atrial tachyarrhythmia development.Chronic shunting typically in the setting of unrepaired CHD as well as the development of pulmonary vascular disease and pulmonary hypertension likely results in gross atrial chamber changes along with histopathologic and electrophysiologic changes due to the long-standing and ongoing hemodynamic disarray.A recent review of arrhythmias in this population of patients showed that nearly onefifth of patients experienced atrial and ventricular arrhythmias, with atrial arrhythmias occurring more frequently [69].Of the atrial arrhythmias documented, AF accounted for 50%.The presence of atrioventricular valve regurgitation and QRS prolongation and the absence of Down syndrome were associated with increased arrhythmia risk,and history of arrhythmias and history of antiarrhythmic drug therapy were both predictors of increased mortality.
For all patients with AF, there is no simple or single algorithm for management regarding rate and rhythm control and stroke prophylaxis.This is particularly true for the CHD population because of the great number of factors that need to be taken into consideration, including the specifics of the anatomy and pathophysiology of the specific CHD as well as the sequelae of palliative or reparative therapies and surgical procedures.With complete and specific knowledge about an individual patient’s CHD history, a therapeutic plan can be achieved that is based on symptoms, chronicity (new onset, paroxysmal, persistent, chronic),rhythms involved (atrial tachycardia, atrial fl utter, AF), cardiac structure and function, ventricular rate response in AF, sinus and atrioventricular nodal function, limitations to pharmacologic therapy due to renal and hepatic function, and risk of thromboembolic events.The variety of treatment options is defined through the fi lter of these factors in the individual patient.
Rate and Rhythm Control Strategies for Atrial Arrhythmias in CHD
Pharmacologic Therapy
Given the multiple substrates, mechanisms, and triggers for atrial arrhythmias, including AF, in the CHD population, pharmacologic therapy is still a mainstay of treatment.Guidelines for pharmacologic therapy for AF exist, with exclusion or very cautious use of antiarrhythmic medications on the basis of multiple structural, functional, electrophysiologic, metabolic and genetic factors [10].In the setting of CHD, many pharmacologic agents may be contraindicated because of the increased risk of proarrhythmia in the setting of structural heart disease and reduced ventricular function.Furthermore,these agents may exacerbate concomitant sick sinus syndrome, and dosing may be further limited by coexisting disease processes affecting renal and hepatic function that impact drug metabolism and excretion.The agents used for primary ventricular rate control, such as calcium channel blockers and beta blockers, may be problematic in patients with depressed ventricular function.
Pharmacologic rhythm control strategies in CHD patients with atrial arrhythmias have evaluated the efficacy of class I and class III antiarrhythmic agents with various degrees of success.Owing to their proarrhythmic potential, particularly in the setting of myocardial scar, baseline conduction abnormalities, and systemic ventricular dysfunction, class IC agents are used with great caution given the frequent presence of these features in CHD patients with arrhythmias.Class III agents, including amiodarone,sotalol, and dofetilide, have also been used.Sotalol is effective in children with operated on CHD although it can unmask sick sinus syndrome requiring pacing [70].It was also effective for single-dose pharmacologic cardioversion in adolescents and adults with CHD, but again can unmask coexisting sick sinus syndrome [71].Dofetilide does not appear to precipitate sick sinus syndrome but carries a risk of QT prolongation, ventricular proarrhythmia, and torsade de pointes [72].The agent was recently studied in a multicenter prospective study evaluating its efficacy and side/adverse effects profile in ACHD patients with atrial arrhythmias [73].While it was initially successful for rhythm control in nearly 70%of patients, and partially successful in the remainder, the long-term use rate was only 49% at 3 years,with many patients stopping using the medication because of reduced efficacy and side effects.Finally,amiodarone is widely used and generally accepted as an effective short-term and long-term antiarrhythmic agent for the treatment of atrial arrhythmias with less concern about cardiac-specific adverse effects even in patients with reduced ventricular function.Hypotension and bradycardia were common side effects during short-term intravenous administration among pediatric patients treated for various forms of SVT [74].However, its long-term use can be problematic, particularly in younger patients, because of potential multiorgan toxic effects.
lnvasive Therapies
Definitive treatment of atrial arrhythmias, including AF, in CHD remains limited to mechanical disruption of the tissue substrate responsible for arrhythmia initiation and propagation.This includes catheter-based ablative modification within the atrial chambers or surgical therapies that create physical barriers to electrical conduction (i.e., incisions and suture lines) or resect highly diseased and arrhythmia-prone tissue or portions of the chamber to result in size reduction.The specific interventional approach to treating these arrhythmias depends on a thorough understanding of the complex interactions between specific CHD anatomy and pathophysiology of the CHD, previous surgical operations and percutaneous procedures, resultant histopathologic and electrophysiologic changes over time, and the specific arrhythmias that have been documented.
Advanced Cardiac lmaging for Procedural Planning
Advanced imaging with CT or MRI can provide valuable information for the evaluation, planning,and decision making processes for arrhythmia treatment in the broad spectrum of young and older CHD patients with high-burden or highly symptomatic arrhythmias.Recent advances in CT techniques now permit highly detailed imaging in pediatric and young adult CHD patients, with submillisievert studies achievable in infants and young children.Alternatively, cardiac MRI permits detailed imaging without ionizing radiation exposure, but can be limited in cases involving non–magnetic resonance conditional cardiac rhythm devices and in patients with renal insufficiency, preventing administration of gadolinium-based contrast agents.With both imaging modalities, artifacts due to sternotomy wires, surgical clips, and prosthetic valves can be problematic.
Both CT and MRI provide high-resolution imaging, not only for delineating general anatomy,chamber size and orientation, and proximity of structures to each other, but also for tissue characterization, which can provide an understanding of arrhythmia mechanisms and potential targets for treatment.Of particular relevance in the treatment of atrial arrhythmias in CHD, advanced imaging can characterize the degree of atrial myopathy with regard to atrial size, shape, and function and the degree of macrofibrosis and microfibrosis.Atrial volume and function can be important for decision making to proceed with AF ablation, as larger atria are associated with a higher recurrence rate of AF[75].The distribution and extent of atrial fi brosis based on cardiac MRI delayed contrast enhancement can provide valuable information regarding potential macroreentrant and microreentrant circuits and other substrate that may promote focal tachycardia or AF.The atrial septum can be clearly visualized with regard to the presence of a patent foramen ovale, ASD, or previous ASD patch or device, as well as its orientation and lie, which may influence transseptal puncture for pulmonary venous atrial access [76].The presence, patency,and integrity of interatrial baffles can be characterized.Advanced imaging also clearly defines pulmonary venous anatomy, the relation of the atria to thoracic structures such as the esophagus, bronchi,and aorta, coronary venous anatomy, and systemic venous drainage patterns, including the presence or absence of left-sided superior vena cava and inferior vena cava interruption.These imaging tools can also provide valuable information regarding chamber size, ventricular function, and valve function.Both CT and MRI can also demonstrate other non-cardiac congenital abnormalities in the chest and abdomen [77, 78].Finally, advanced imaging provides clear delineation of baffle and conduit structures, which may be the sites of arrhythmia foci or anatomic complexities that may influence the approach to percutaneous arrhythmia therapeutic interventions (Figure 3, Video 1 [Video 1 is available at the following link https://youtu.be/H16F7zHK4Q4]).

Figure 3 Pre-Ablation Planning Cardiovascular Computed Tomographic Images for an Adult Patient with D-Transposition of the Great Arteries Status Post Mustard Atrial Baffle in Childhood with a History of IART.
Specific to imaging of Fontan circuits, delayed images or simultaneous contrast injections from upper and lower extremity venous sites are often required to fully delineate the baffle location, size,and course.The datasets from advanced cardiac imaging can also be used for three-dimensional printing of models for procedural planning and virtual computer modeling of macroreentrant circuits and prediction of potential lesion sets.On the basis of these findings, decisions can be made as to whether to proceed with invasive treatments, and if so, whether surgical, minimally invasive, percutaneous, or hybrid procedures are most suitable.
Catheter-Based Therapies
Percutaneous catheter ablation has become the mainstay in definitive arrhythmia treatment in patients with CHD.Both radiofrequency ablation and cryotherapy are used with high degrees of success.While the predominant experience in ablation for atrial arrhythmias in CHD has centered on ablative treatment of IART, focal tachycardias,and conventional SVT substrates, contemporary experience in the management of AF with catheter ablation is slowly growing.Furthermore, given the likely substantial overlap in diseased atrial substrate that contributes to both reentrant atrial arrhythmias and AF in CHD, the current approaches to ablative substrate modification in CHD should target and address both arrhythmia types if they occur in the same individual.As such, the authors advocate a comprehensive ablation approach to address both AF and other arrhythmia types during a single procedure in patients with clearly and independently documented atrial arrhythmias and AF.
Preprocedural planning is critical for the safe and successful performance of catheter ablation in patients with CHD.A thorough and complete understanding of the original type of CHD, all previous reparative and palliative procedures, current anatomical and structural configurations, and current quantitative functional statuses, including ventricular function and clinical functional capacity, is of highest priority.Clear understanding of the association between clinical arrhythmias and potential arrhythmia substrates will help to guide the diagnostic and therapeutic aspects of the procedure.Integration of advanced imaging with conventional echocardiographic modalities is now commonly done in CHD patients undergoing ablative treatments.As previously mentioned, advanced imaging provides critical information for procedural planning, but can also be integrated into the ablation procedure itself, providing the ability to merge CT or MRI data with three-dimensional electroanatomic mapping (Figure 4).
Appropriate anesthesia support, anticoagulation management, and pharmacotherapy adjustments are extremely important to ensure patient comfort, risk reduction, and clinical stability both during and after the ablation procedure.The catheter approach, vascular access, and catheter positioning must be carefully planned on the basis of the type of arrhythmias being treated, available venous and arterial connections to the heart, and patient and cardiac chamber sizes.Access to the pulmonary venous atrium or chamber is frequently required,and the approach to transseptal or transbaffle access needs to be carefully planned following thorough discussion regarding risks with the patient.The feasibility and safety of transseptal and transbaffle punctures following CHD repair or palliation have been reasonably demonstrated [79–85].Access to the systemic and pulmonary venous atrial chambers is of significant importance for IART ablation involving macroreentrant circuits using the cavotricuspid isthmus.This area of atrial tissue may span portions of both the systemic venous atrium and the pulmonary venous atrium in patients with transposition of the great arteries following atrial switch operations as well as in patients with atriopulmonary or lateral tunnel Fontan configurations.A retrograde approach through the aortic valve can also be used to position the ablation catheter at the cavotricuspid isthmus in CHD substrates involving a systemic morphologic right ventricle with original atrioventricular concordance [86].For patients where inferior vena cava–atrial continuity is completely absent, as would be the case in extracardiac Fontan completion, pulmonary venous atrial access is dependent entirely on transconduit puncture,catheter entry through a preexisting fenestration,or direct pulmonary venous atrial chamber access through percutaneous transhepatic or transthoracic entry [87, 88].Moore et al.[89] reported on the utility of CT angiography, which can reveal more directly accessible portions of the chamber or sites for access that afford the shortest distance to chamber entry in Fontan patients.
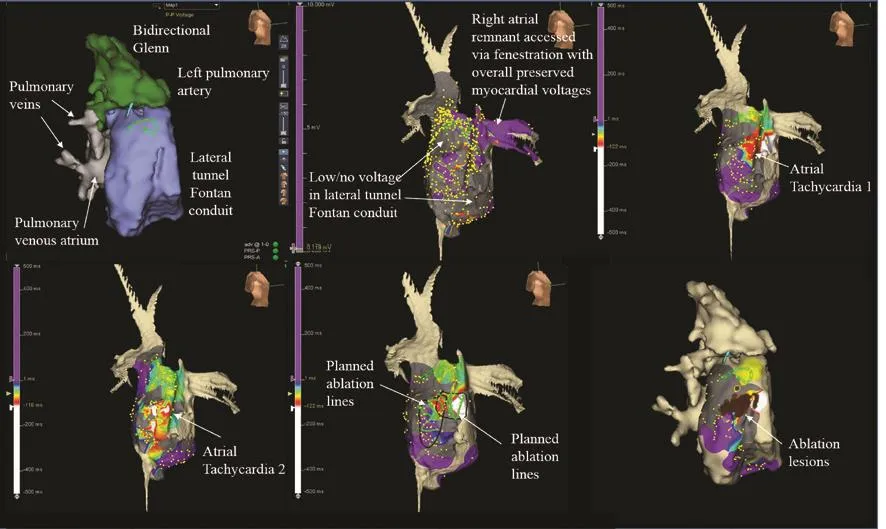
Figure 4 Advanced Cardiac Imaging Integration with Electroanatomic Mapping for Catheter Ablation Planning and Performance in an Adult with a Fenestrated Lateral Tunnel Fontan and Recurrent Atrial Tachyarrhythmias.
Adjunctive imaging with intracardiac echocardiography and CT or MRI merging is evolving as a valuable tool to guide ablation performance, improve procedural safety, and reduce radiation exposure.Intracardiac echocardiography provides direct imaging for the presence of intracardiac thrombi,pulmonary vein stenosis, proximity of structures to the esophagus, and presence or development of pericardial effusion.It also provides real-time visualization during transseptal or transbaffle puncture and during ablation delivery to assess catheter tip contact, ablation lesion depth, and formation of microbubbles during radiofrequency energy delivery [90].Image acquisition, segmentation, landmark registration, and surface registration allow CT or MRI image integration with electroanatomic mapping software, thereby permitting their use during chamber geometrical and arrhythmia mapping.
Targets for ablation are generally determined by a combination of awareness of frequently associated anatomic locations (including the cavotricuspid isthmus and crista terminalis), careful mapping of macroreentrant circuits and focal sites of arrhythmias,and attention to highly suspicious substrate based on anatomic location, tissue characteristics, and distribution of low voltages, signal fractionation, and late potentials [91–95].While advances in technology have continually been introduced, successful ablation outcomes remain driven by fundamental techniques of entrainment mapping coupled with electroanatomic mapping [96].However, recurrence rates of arrhythmias highlight the complex, dynamic,and changing substrate that drives arrhythmia development even after effective ablation therapy in CHD.
The role of the pulmonary veins in CHD-associated AF remains unclear.Because CHD-associated AF is typically not seen in the absence of concomitant atrial myopathy, pulmonary vein isolation alone should not be expected to effectively treat AF even as an initial ablation procedure in the setting of paroxysmal AF.However, it is still important to eliminate the contribution of pulmonary vein triggers, either by direct ablation or by electrical isolation, as part of a comprehensive ablative treatment plan for atrial arrhythmias, including AF, in CHD [97–99].
Novel features in three-dimensional electroanatomic mapping systems are being assessed for their utility in complex arrhythmia ablation, and will require specific investigation in CHD populations[100].The role of rapid mapping technologies is expanding in ablation procedures for CHD patients.Rapid, high-density mapping technologies have provided the ability to collect many points simultaneously, with the information collected at each point including the activation timing, voltage, and comparison with adjacent points.These systems have the potential to shorten the procedural duration while increasing the resolution of electrophysiologic mapping, both of which can contribute to improved procedural safety and ablation success.
Remote magnetic navigation allows catheter manipulation remotely with use of a control console, and has shown utility in catheter navigation within challenging structures such as baffles.The combination of remote magnetic navigation, three-dimensional image integration, and electroanatomic mapping facilitated safe and feasible ablation even in patients with complex anomalies [101].For patients with complex disease, remote magnetic navigation also has led to a decrease in fl uoroscopy time [102].The development of real-time MRI during catheter ablation procedures permits magnetic resonance–based visualization of transmurality of ablation lesions with gadolinium and identification of gaps in long linear lesions, both of which can result in arrhythmia recurrences following short-term ablation success [103].
Surgical Therapies
Surgical therapies for atrial arrhythmias, including AF, are typically performed concomitantly with other recommended or indicated surgical interventions in CHD patients.The Maze procedure has evolved significantly, with expansion and modification of lesion sets in both atria as well as the adoption of ablative as opposed to incisional lesions.Furthermore, arrhythmia surgery in CHD frequently involves direct tissue excision for removal of arrhythmia-prone substrate and chamber size reduction.Perhaps the best examples of integrated arrhythmia surgery with other CHD surgery are in Fontan conversion surgery for patients with failing Fontan physiology and high arrhythmia burden[104, 105].When surgical ablative treatments are considered, decisions regarding intervention in the left or right atrium only, biatrial ablation, or surgical left atrial ablation with either presurgical or postsurgical right-sided percutaneous catheter ablation need to be made.Furthermore, given the high incidence of atrial arrhythmias associated with the resultant substrate after congenital heart surgery,some authors have suggested prophylactic lesion sets be performed at the time of surgery to prevent arrhythmia problems such as incisional reentry [42].
Device Therapies
Cardiac implantable electronic devices are an important adjunctive treatment in CHD patients with atrial arrhythmias.Bradyarrhythmias and tachyarrhythmias frequently coexist in patients with previously repaired or palliated CHD, and many CHD patients will develop primary pacing indications over time[106–108].Severe bradycardia and pauses related to primary sinus node dysfunction can trigger AF and other atrial arrhythmias.Alternatively, CHD patients can have both sinus node dysfunction and separate atrial myopathic substrate–related arrhythmias, owing to prior CHD surgical interventions.In these instances, pacing therapies either are necessary or can be very helpful in addition to pharmacologic therapy or ablation.
Atrioventricular junction ablation and pacing for AF ventricular rate control is useful in scenarios where pharmacologic therapy is either ineffective in achieving ventricular rate control or limited in use by the substrate or pathophysiology.While a transvenous approach can technically be used across a broad range of CHD defects, nodal ablation can be more challenging in patients with complex atrial baffle structures or Fontan circuits [109].
The choice of the type of cardiac implantable electronic device and the route of implantation must be tailored on the basis of specific anatomy,concomitant arrhythmias, native conduction system status, and ventricular functional status.Singlechamber ventricular pacing can be used in patients in persistent or permanent AF.Preservation of atrioventricular synchrony would be desirable in patients with paroxysmal AF.Primary atrial pacing with minimization of ventricular pacing in patients with intact atrioventricular nodal function is preferable in patients with sinus node dysfunction.Consistent atrial pacing may also reduce atrial arrhythmia burden.The integration of atrial arrhythmia preventive treatments or antitachycardia pacing for termination of arrhythmias should be considered if there is sufficient evidence demonstrating their effectiveness or highly suggesting their utility in individual CHD patients with atrial arrhythmias [110, 111].
While transvenous leads have demonstrated better longevity and function compared with epicardial leads, the choice of lead type in CHD patients depends on patient size, venous continuity with atrial and ventricular chambers, and the presence or absence of intracardiac shunts.The risk of thromboembolic events and complications in the setting of transvenous leads and intracardiac shunt lesions is elevated and is not eliminated with concomitant anticoagulative therapies [112].Among singleventricle CHD patients lacking typical venoatrial connections, epicardial leads are most commonly placed when pacing is indicated.However, transvenous leads have been implanted in certain unique scenarios.Transvenous lead implantation within the atrial portion of the lateral tunnel Fontan and ventricular pacing lead implantation via the coronary sinus through the Fontan when coronary sinus-to-Fontan atrium continuity is present have been described [113–116].Finally, transmural(epicardial to endocardial) atrial lead implantation has been described, with the expectant goal of achieving lead functionality and longevity similar to those of standard transvenous endocardial leads in patients lacking standard venoatrial continuity[117].
Stroke Prophylaxis in CHD Patients with Atrial Arrhythmias
The risk of thromboembolic complications and stroke in the setting of CHD and AF is well recognized but incompletely understood from mechanistic and risk-stratification standpoints.In children and adults with CHD, ischemic and hemorrhagic stroke risk is significantly higher than in the general population [118, 119].Imaging with three- dimensional transesophageal echocardiography has demonstrated a higher incidence of intracardiac thrombi in atrial fl utter/AF patients with CHD compared with patients without CHD[120].
In ACHD with atrial arrhythmias, CHA2DS2-VASc scoring predicted thromboembolic events when applied retrospectively [121].However, the CHA2DS2-VASc scoring system does not specif ically account for CHD and is not directly applicable to all CHD patients, particularly those of much younger age and with AF that is technically nonvalvular but still occurring in an atrial substrate with probable elevated risk of thrombus formation.Additional research is required to devise new approaches to stroke risk stratification and to see whether advances in the long-term management of CHD, including the timing of surgery and interventions to minimize the development of arrhythmias, may reduce this thromboembolic risk [119].
Presently, most CHD practitioners would advocate anticoagulation in CHD patients with documented sustained or recurrent atrial arrhythmias, including AF.Additional considerations include the concomitant presence of erythrocytosis, Eisenmenger syndrome, mechanical valves, and conduits with altered or sluggish blood fl ow.Warfarin is most frequently used, although prospective data on the use of novel oral anticoagulant agents in CHD is growing.
The applicability and indications for percutaneous atrial appendage occlusion or surgical appendectomy in CHD is an area of interest and future research.Concomitant surgical ligation of the appendage at the time of reoperation for other indications in CHD likely has a valuable role for consideration, and it is unclear if appendage occlusion can have a benef it in stroke risk reduction and anticoagulation measures in patients with CHD and atrial arrhythmias, including AF.In regard to the atrial appendages, congenital anomalies exist, including juxtaposition of the atrial appendages, giant congenital left atrial appendage aneurysm, congenital left atrial appendage herniation,and congenital absence of the left atrial appendage [122–126].These unique morphologic patterns may affect the risk of appendage-associated thrombus formation, and are not currently amenable to percutaneous appendage occlusion strategies.Certainly in CHD conditions with otherwise normal atrioventricular and ventriculoarterial concordance, the role of the left atrial appendage in AF-associated stroke risk is likely similar to that in structurally normal hearts with AF.The possible role of the right atrial appendage or the appendage structures or remnants in morphologically abnormal or surgically altered atria is not entirely clear,nor are percutaneous occlusion devices indicated at present.
Conclusions
Atrial arrhythmias, including AF, in CHD remain a prominent and growing contributor to morbidity and mortality.The mechanisms and substrates for arrhythmia development and progression to varying degrees of AF involve a highly complex and dynamic combination of numerous factors related to the original CHD type, past treatments, continually evolving procedures, and aging of the ACHD population.Application of pharmacologic and invasive therapeutic options for primary atrial arrhythmia and AF treatment as well as stroke prevention necessitates special considerations when applied to the CHD population and requires greater study in specific subsets of CHD patients.
Conflict of lnterest
The authors declare that they have no conflicts of interest.
REFERENCES
1.Warnes CA, Williams RG, Bashore TM, Child JS, Connolly HM,Dearani JA, et al.ACC/AHA 2008 guidelines for the management of adults with congenital heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Develop Guidelines on the Management of Adults with Congenital Heart Disease).Circulation 2008;118:e714–833.
2.Marelli AJ, Mackie AS, Ionescu-Ittu R, Rahme E, Pilote L.Congenital heart disease in the general population: changing prevalence and age distribution.Circulation 2007;115:163–72.
3.Marelli AJ, Ionescu-Ittu R, Mackie AS, Guo L, Dendukuri N, Kaouache M.Lifetime prevalence of congenital heart disease in the general population from 2000 to 2010.Circulation 2014;130:749–56.
4.Teuwen CP, Ramdjan TT, Gotte M,Brundel BJ, Evertz R, Vriend JW,et al.Time course of atrial fi brillation in patients with congenital heart defects.Circ Arrhythm Electrophysiol 2015;8:1065–72.
5.Labombarda F, Hamilton R,Shohoudi A, Aboulhosn J, Broberg CS, Chaix MA, et al.Increasing prevalence of atrial fi brillation and permanent atrial arrhythmias in congenital heart disease.J Am Coll Cardiol 2017;70:857–65.
6.Mandalenakis Z, Rosengren A,Lappas G, Eriksson P, Gilljam T,Hansson PO, et al.Atrial fi brillation burden in young patients with congenital heart disease.Circulation 2018;137(9):928–37.
7.Bouchardy J, Therrien J, Pilote L, Ionescu-Ittu R, Martucci G,Bottega N, et al.Atrial arrhythmias in adults with congenital heart disease.Circulation 2009;120:1679–86.
8.Kwak JG, Seo JW, Oh SS, Lee SY, Ham EK, Kim WH, et al.Histopathologic analysis of atrial tissue in patients with atrial fi brillation: comparison between patients with atrial septal defect and patients with mitral valvular heart disease.Cardiovasc Pathol 2014;23:185–92.
9.van der Hulst AE, Roest AA,Holman ER, Vliegen HW,Hazekamp MG, Bax JJ, et al.Relation of prolonged tissue Doppler imaging-derived atrial conduction time to atrial arrhythmia in adult patients with congenital heart disease.Am J Cardiol 2012;109:1792–6.
10.January CT, Wann LS, Alpert JS,Calkins H, Cigarroa JE, Cleveland JC Jr, et al.2014 AHA/ACC/HRS guideline for the management of patients with atrial fi brillation: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the Heart Rhythm Society.Circulation 2014;130:e199–267.
11.Gandhi SK, Bromberg BI, Rodefeld MD, Schuessler RB, Boineau JP, Cox JL, et al.Lateral tunnel suture line variation reduces atrial fl utter after the modified Fontan operation.Ann Thorac Surg 1996;61:1299–309.
12.Trojnarska O, Grajek S, Kramer L, Gwizdala A.Risk factors of supraventricular arrhythmia in adults with congenital heart disease.Cardiol J 2009;16:218–26.
13.Kirsh JA, Walsh EP, Triedman JK.Prevalence of and risk factors for atrial fi brillation and intraatrial reentrant tachycardia among patients with congenital heart disease.Am J Cardiol 2002;90:338–40.
14.Triedman JK.Atypical atrial tachycardias in patients with congenital heart disease.Heart Rhythm 2008;5:315–7.
15.Walsh EP, Cecchin F.Arrhythmias in adult patients with congenital heart disease.Circulation 2007;115:534–45.
16.Bernier M, Marelli AJ, Pilote L,Bouchardy J, Bottega N, Martucci G, et al.Atrial arrhythmias in adult patients with right- versus left-sided congenital heart disease anomalies.Am J Cardiol 2010;106:547–51.
17.Ueda A, Adachi I, McCarthy KP, Li W, Ho SY, Uemura H.Substrates of atrial arrhythmias: histological insights from patients with congenital heart disease.Int J Cardiol 2013;168:2481–6.
18.Li W, Somerville J.Atrial fl utter in grown-up congenital heart (GUCH)patients.Clinical characteristics of affected population.Int J Cardiol 2000;75:129–37; discussion 138–9.
19.Lukac P, Pedersen AK, Mortensen PT, Jensen HK, Hjortdal V, Hansen PS.Ablation of atrial tachycardia after surgery for congenital and acquired heart disease using an electroanatomic mapping system: which circuits to expect in which substrate?Heart Rhythm 2005;2:64–72.
20.Uhm JS, Mun HS, Wi J, Shim J, Hwang HJ, Sung JH, et al.Importance of tachycardia cycle length for differentiating typical atrial fl utter from scar-related in adult congenital heart disease.Pacing Clin Electrophysiol 2012;35:1338–47.
21.Akar JG, Kok LC, Haines DE, DiMarco JP, Mounsey JP.Coexistence of type I atrial fl utter and intra-atrial re-entrant tachycardia in patients with surgically corrected congenital heart disease.J Am Coll Cardiol 2001;38:377–84.
22.Anguera I, Dallaglio P, Macias R, Jiménez-Candil J, Peinado R,García-Seara J, et al.Long-term outcome after ablation of right atrial tachyarrhythmias after the surgical repair of congenital and acquired heart disease.Am J Cardiol 2015;115:1705–13.
23.Mandapati R, Walsh EP, Triedman JK.Pericaval and periannular intraatrial reentrant tachycardias in patients with congenital heart disease.J Cardiovasc Electrophysiol 2003;14:119–25.
24.de Groot NM, Lukac P, Schalij MJ, Makowski K, Szili-Torok T,Jordaens L, et al.Long-term outcome of ablative therapy of postoperative atrial tachyarrhythmias in patients with tetralogy of Fallot:a European multi-centre study.Europace 2012;14:522–7.
25.de Groot NM, Zeppenfeld K,Wijffels MC, Chan WK, Blom NA,Van der Wall EE, et al.Ablation of focal atrial arrhythmia in patients with congenital heart defects after surgery: role of circumscribed areas with heterogeneous conduction.Heart Rhythm 2006;3:526–35.
26.Seslar SP, Alexander ME, Berul CI, Cecchin F, Walsh EP, Triedman JK.Ablation of nonautomatic focal atrial tachycardia in children and adults with congenital heart disease.J Cardiovasc Electrophysiol 2006;17:359–65.
27.Li W, Somerville J, Gibson DG,Henein MY.Effect of atrial fl utter on exercise tolerance in patients with grown-up congenital heart (GUCH).Am Heart J 2002;144:173–9.
28.Yap SC, Harris L, Chauhan VS,Oechslin EN, Silversides CK.Identifying high risk in adults with congenital heart disease and atrial arrhythmias.Am J Cardiol 2011;108:723–8.
29.Reich JD, Auld D, Hulse E, Sullivan K, Campbell R.The Pediatric Radiofrequency Ablation Registry’s experience with Ebstein’s anomaly.J Cardiovasc Electrophysiol 1998;9:1370–7.
30.Perosio AM, Suarez LD, Bunster AM,Locreille A, Apkarian OA, Vallazza MA, et al.Pre-excitation syndrome and hypertrophic cardiomyopathy.J Electrocardiol 1983;16:29–40.
31.Correa R, Sherwin ED, Kovach J,Mah DY, Alexander ME, Cecchin F, et al.Mechanism and ablation of arrhythmia following total cavopulmonary connection.Circ Arrhythm Electrophysiol 2015;8(2):318–25.
32.Rowin EJ, Hausvater A, Link MS,Abt P, Gionfriddo W, Wang W,et al.Clinical profile and consequences of atrial fi brillation in hypertrophic cardiomyopathy.Circulation 2017;136(25):2420–36.
33.Oddsson H, Edvardsson N,Walfridsson H.Episodes of atrial fi brillation and atrial vulnerability after successful radiofrequency catheter ablation in patients with Wolff-Parkinson-White syndrome.Europace 2002;4:201–6.
34.Loomba RS, Chandrasekar S, Sanan P, Shah PH, Arora RR.Association of atrial tachyarrhythmias with atrial septal defect, Ebstein’s anomaly and Fontan patients.Expert Rev Cardiovasc Ther 2011;9:887–93.
35.Oliver JM, Gallego P, Gonzalez A,Benito F, Mesa JM, Sobrino JA.Predisposing conditions for atrial fi brillation in atrial septal defect with and without operative closure.Am J Cardiol 2002;89:39–43.
36.Berger F, Vogel M, Kramer A, Alexi-Meskishvili V, Weng Y, Lange PE,et al.Incidence of atrial fl utter/fibrillation in adults with atrial septal defect before and after surgery.Ann Thorac Surg 1999;68:75–8.
37.Wasmer K, Kobe J, Dechering DG,Bittner A, Mönnig G, Milberg P,et al.Isthmus-dependent right atrial fl utter as the leading cause of atrial tachycardias after surgical atrial septal defect repair.Int J Cardiol 2013;168:2447–52.
38.Nitta T, Sakamoto S, Miyagi Y,Fujii M, Ishii Y, Ochi M.Reentrant and focal activations during atrial fi brillation in patients with atrial septal defect.Ann Thorac Surg 2013;96:1266–72.
39.Giannakoulas G, Dimopoulos K, Yuksel S, Inuzuka R, Pijuan-Domenech A, Hussain W, et al.Atrial tachyarrhythmias late after Fontan operation are related to increase in mortality and hospitalization.Int J Cardiol 2012;157:221–6.
40.Collins KK, Rhee EK, Delucca JM, Alexander ME, Bevilacqua LM, Berul CI, et al.Modification to the Fontan procedure for the prophylaxis of intra-atrial reentrant tachycardia: short-term results of a prospective randomized blinded trial.J Thorac Cardiovasc Surg 2004;127:721–9.
41.Atallah J, Collins KK, Jonas RA, Mayer JE Jr, Triedman JK.Follow-up of a modified Fontan randomized trial for intraatrial reentrant tachycardia prophylaxis.Congenit Heart Dis 2012;7:219–25.
42.Mavroudis C, Stulak JM, Ad N,Siegel A, Giamberti A, Harris L,et al.Prophylactic atrial arrhythmia surgical procedures with congenital heart operations: review and recommendations.Ann Thorac Surg 2015;99:352–9.
43.De Groot NM, Blom N, Vd Wall EE, Schalij MJ.Different mechanisms underlying consecutive, postoperative atrial tachyarrhythmias in a Fontan patient.Pacing Clin Electrophysiol 2009;32:e18–20.
44.Gelatt M, Hamilton RM, McCrindle BW, Gow RM, Williams WG,Trusler GA, et al.Risk factors for atrial tachyarrhythmias after the Fontan operation.J Am Coll Cardiol 1994;24:1735–41.
45.Li SJ, Wong SJ, Cheung YF.Atrial and ventricular mechanics in patients after Fontan-type procedures: atriopulmonary connection versus extracardiac conduit.J Am Soc Echocardiogr 2014;27:666–74.
46.Yap SC, Harris L, Downar E,Nanthakumar K, Silversides CK,Chauhan VS.Evolving electroanatomic substrate and intra-atrial reentrant tachycardia late after Fontan surgery.J Cardiovasc Electrophysiol 2012;23:339–45.
47.Quinton E, Nightingale P, Hudsmith L, Thorne S, Marshall H, Clift P,et al.Prevalence of atrial tachyarrhythmia in adults after Fontan operation.Heart 2015;101:1672–7.
48.Mouws E, de Groot NMS.Atrial Tachyarrhythmia in congenital heart disease: beyond the suture lines.Circ Arrhythm Electrophysiol 2017;10(9):e005697.
49.Song MK, Bae EJ, Kwon BS, Kim GB, Noh CI, Choi JY, et al.Intraatrial reentrant tachycardia in adult patients after Fontan operation.Int J Cardiol 2015;187:157–63.
50.Li W, Sarubbi B, Sutton R,Somerville J, Gibson D, Henein MY.Atrial and ventricular electromechanical function in 1-ventricle hearts: influence of atrial fl utter and Fontan procedure.J Am Soc Echocardiogr 2001;14:186–93.
51.Law IH, Fischbach PS, Goldberg C, Mosca RS, Bove EL, Lloyd TR,et al.Inducibility of intra-atrial reentrant tachycardia after the fi rst two stages of the Fontan sequence.J Am Coll Cardiol 2001;37:231–7.
52.Miyazaki A, Sakaguchi H, Ohuchi H, Yamada O, Kitano M, Yazaki S, et al.The clinical course and incidence of supraventricular tachyarrhythmias after extra-cardiac conduit Fontan procedures in relation to an atrial situs.Circ J 2011;75:413–20.
53.Yoshikawa Y, Ishibashi-Ueda H,Uemura H, Kawahira Y, Yagihara T.Pathologic findings in atrial musculature seven years after the intraatrial tunnel Fontan.Ann Thorac Surg 2002;73:663–4.
54.Tuzcu V, Ozkan B, Sullivan N,Karpawich P, Epstein ML.P wave signal-averaged electrocardiogram as a new marker for atrial tachyarrhythmias in postoperative Fontan patients.J Am Coll Cardiol 2000;36:602–7.
55.Wong T, Davlouros PA, Li W,Millington-Sanders C, Francis DP,Gatzoulis MA.Mechano-electrical interaction late after Fontan operation: relation between P-wave duration and dispersion, right atrial size,and atrial arrhythmias.Circulation 2004;109:2319–25.
56.Hui W, Abd El Rahman MY,Dsebissowa F, Rentzsch A,Gutberlet M, Alexi-Meskishvili V,et al.Quantitative analysis of right atrial performance after surgical repair of tetralogy of Fallot.Cardiol Young 2004;14:520–6.
57.Harrison DA, Siu SC, Hussain F,MacLoghlin CJ, Webb GD, Harris L.Sustained atrial arrhythmias in adults late after repair of tetralogy of Fallot.Am J Cardiol 2001;87:584–8.
58.Luijnenburg SE, Peters RE, van der Geest RJ, Moelker A, Roos-Hesselink JW, de Rijke YB, et al.Abnormal right atrial and right ventricular diastolic function relate to impaired clinical condition in patients operated for tetralogy of Fallot.Int J Cardiol 2013;167:833–9.
59.Sohns JM, Rosenberg C, Zapf A,Unterberg-Buchwald C, Staab W,Schuster A, et al.Right atrial volume is increased in corrected tetralogy of Fallot and correlates with the incidence of supraventricular arrhythmia: a CMR study.Pediatr Cardiol 2015;36:1239–47.
60.Riesenkampff E, Al-Wakeel N, Kropf S, Stamm C, Alexi-Meskishvili V, Berger F, et al.Surgery impacts right atrial function in tetralogy of Fallot.J Thorac Cardiovasc Surg 2014;147:1306–11.
61.Khairy P, Aboulhosn J, Gurvitz MZ,Opotowsky AR, Mongeon FP, Kay J, et al.Arrhythmia burden in adults with surgically repaired tetralogy of Fallot: a multi-institutional study.Circulation 2010;122:868–75.
62.Hou J, Yu HK, Wong SJ, Cheung YF.Atrial mechanics after surgical repair of tetralogy of Fallot.Echocardiography 2015;32:126–34.
63.Dos L, Teruel L, Ferreira IJ,Rodriguez-Larrea J, Miro L, Girona J, et al.Late outcome of Senning and Mustard procedures for correction of transposition of the great arteries.Heart 2005;91:652–6.
64.Puley G, Siu S, Connelly M,Harrison D, Webb G, Williams WG,et al.Arrhythmia and survival in patients >18 years of age after the mustard procedure for complete transposition of the great arteries.Am J Cardiol 1999;83:1080–4.
65.Sarkar D, Bull C, Yates R, Wright D, Cullen S, Gewillig M, et al.Comparison of long-term outcomes of atrial repair of simple transposition with implications for a late arterial switch strategy.Circulation 1999;100:II176–81.
66.Li W, Somerville J, Gibson DG,Henein MY.Disturbed atrioventricular electromechanical function long after Mustard operation for transposition of great arteries:a potential contributing factor to atrial fl utter.J Am Soc Echocardiogr 2001;14:1088–93.
67.Chinen S, Miura M, Tamame T,Matsuoka M, Ohki H, Sumitomo N.Life-threatening atrial tachycardia after the Senning operation in a patient with transposition of the great arteries.Heart Vessels 2012;27:424–7.
68.Khairy P, Harris L, Landzberg MJ,Fernandes SM, Barlow A, Mercier LA, et al.Sudden death and defibrillators in transposition of the great arteries with intra-atrial baffles: a multicenter study.Circ Arrhythm Electrophysiol 2008;1:250–7.
69.Baskar S, Horne P, Fitzsimmons S, Khoury PR, Vettukattill J, Niwa K, et al.Arrhythmia burden and related outcomes in Eisenmenger syndrome.Congenit Heart Dis 2017;12:512–9.
70.Beaufort-Krol GC, Bink-Boelkens MT.Sotalol for atrial tachycardias after surgery for congenital heart disease.Pacing Clin Electrophysiol 1997;20:2125–9.
71.Rao SO, Boramanand NK,Burton DA, Perry JC.Atrial tachycardias in young adults and adolescents with congenital heart disease: conversion using single dose oral sotalol.Int J Cardiol 2009;136:253–7.
72.Banchs JE, Baquero GA, Nickolaus MJ, Wolbrette DL, Kelleman JJ,Samii S, et al.Clinical efficacy of dofetilide for the treatment of atrial tachyarrhythmias in adults with congenital heart disease.Congenit Heart Dis 2014;9:221–7.
73.El-Assaad I, Al-Kindi SG, Abraham J, Sanatani S, Bradley DJ, Halsey C, et al.Use of dofetilide in adult patients with atrial arrhythmias and congenital heart disease: a PACES collaborative study.Heart Rhythm 2016;13:2034–9.
74.Chang PM, Silka MJ, Moromisato DY, Bar-Cohen Y.Amiodarone versus procainamide for the acute treatment of recurrent supraventricular tachycardia in pediatric patients.Circ Arrhythm Electrophysiol 2010;3:134–40.
75.Helms AS, West JJ, Patel A, Lipinski MJ, Mangrum JM, Mounsey JP,et al.Relation of left atrial volume from three-dimensional computed tomography to atrial fi brillation recurrence following ablation.Am J Cardiol 2009;103:989–93.
76.Juneja R, Rowland E, Ho SY.Atrial morphology in hearts with congenitally corrected transposition of the great arteries: implications for the interventionist.J Cardiovasc Electrophysiol 2002;13:158–63.
77.Troxclair D, Ross KF, Newman WP 3rd.Cor triatriatum sinistrum: a rare congenital cardiac anomaly presenting in an adult with chronic atrial fi brillation.Am J Forensic Med Pathol 2005;26:282–4.
78.Gengsakul A, Sett SS, Hosking MC.Congenital right atrial diverticulum, atrial septal defect within the oval fossa, and complex pulmonary valvar obstruction in an infant with chromosome 8(p23.1) deletion.Cardiol Young 2005;15:306–8.
79.Li X, Wissner E, Kamioka M,Makimoto H, Rausch P, Metzner A,et al.Safety and feasibility of transseptal puncture for atrial fi brillation ablation in patients with atrial septal defect closure devices.Heart Rhythm 2014;11:330–5.
80.Yamada T, McElderry HT, Muto M,Murakami Y, Kay GN.Pulmonary vein isolation in patients with paroxysmal atrial fi brillation after direct suture closure of congenital atrial septal defect.Circ J 2007;71:1989–92.
81.Lakkireddy D, Rangisetty U, Prasad S, Verma A, Biria M, Berenbom L, et al.Intracardiac echo-guided radiofrequency catheter ablation of atrial fi brillation in patients with atrial septal defect or patent foramen ovale repair: a feasibility, safety,and efficacy study.J Cardiovasc Electrophysiol 2008;19:1137–42.
82.Dave AS, Aboulhosn J, Child JS,Shivkumar K.Transconduit puncture for catheter ablation of atrial tachycardia in a patient with extracardiac Fontan palliation.Heart Rhythm 2010;7:413–6.
83.Correa R, Walsh EP, Alexander ME, Mah DY, Cecchin F, Abrams DJ, et al.Transbaffle mapping and ablation for atrial tachycardias after Mustard, Senning, or Fontan operations.J Am Heart Assoc 2013;2:e000325.
84.Krause U, Backhoff D, Klehs S,Schneider HE, Paul T.Transbaffle catheter ablation of atrial re-entrant tachycardia within the pulmonary venous atrium in adult patients with congenital heart disease.Europace 2016;18(7):1055–60.
85.Perry JC, Boramanand NK, Ing FF.“Transseptal” technique through atrial baffles for 3-dimensional mapping and ablation of atrial tachycardia in patients with d-transposition of the great arteries.J Interv Card Electrophysiol 2003;9:365–9.
86.El Yaman MM, Asirvatham SJ,Kapa S, Barrett RA, Packer DL,Porter CB.Methods to access the surgically excluded cavotricuspid isthmus for complete ablation of typical atrial fl utter in patients with congenital heart defects.Heart Rhythm 2009;6:949–56.
87.Knecht S, Laureys M, Castro-Rodriguez J, Dessy H, Wright M,Verbeet T.Percutaneous transhepatic access for ablation of atypical atrial fl utter in complex congenital heart disease.J Cardiovasc Electrophysiol 2013;24:589–90.
88.Nehgme RA, Carboni MP, Care J,Murphy JD.Transthoracic percutaneous access for electroanatomic mapping and catheter ablation of atrial tachycardia in patients with a lateral tunnel Fontan.Heart Rhythm 2006;3:37–43.
89.Moore JP, Hendrickson B,Brunengraber DZ, Shannon KM.Transcaval puncture for access to the pulmonary venous atrium after the extracardiac total cavopulmonary connection operation.Circ Arrhythm Electrophysiol 2015;8:824–8.
90.Peichl P, Kautzner J, Gebauer R.Ablation of atrial tachycardias after correction of complex congenital heart diseases: utility of intracardiac echocardiography.Europace 2009;11:48–53.
91.De Groot NM, Kuijper AF, Blom NA, Bootsma M, Schalij MJ.Three-dimensional distribution of bipolar atrial electrogram voltages in patients with congenital heart disease.Pacing Clin Electrophysiol 2001;24:1334–42.
92.Akca F, Bauernfeind T, De Groot NM, Shalganov T, Schwagten B,Szili-Torok T.The presence of extensive atrial scars hinders the differential diagnosis of focal or macroreentrant atrial tachycardias in patients with complex congenital heart disease.Europace 2014;16:893–8.
93.Triedman JK, Alexander ME,Berul CI, Bevilacqua LM, Walsh EP.Electroanatomic mapping of entrained and exit zones in patients with repaired congenital heart disease and intra-atrial reentrant tachycardia.Circulation 2001;103:2060–5.
94.Nakagawa H, Shah N, Matsudaira K, Overholt E, Chandrasekaran K, Beckman KJ, et al.Characterization of reentrant circuit in macroreentrant right atrial tachycardia after surgical repair of congenital heart disease: isolated channels between scars allow “focal” ablation.Circulation 2001;103:699–709.
95.Love BA, Collins KK, Walsh EP,Triedman JK.Electroanatomic characterization of conduction barriers in sinus/atrially paced rhythm and association with intra-atrial reentrant tachycardia circuits following congenital heart disease surgery.J Cardiovasc Electrophysiol 2001;12:17–25.
96.Delacretaz E, Ganz LI, Soejima K,Friedman PL, Walsh EP, Triedman JK, et al.Multi atrial maco-re-entry circuits in adults with repaired congenital heart disease: entrainment mapping combined with three-dimensional electroanatomic mapping.J Am Coll Cardiol 2001;37:1665–76.
97.Frankel DS, Shah MJ, Aziz PF,Hutchinson MD.Catheter ablation of atrial fi brillation in transposition of the great arteries treated with mustard atrial baffle.Circ Arrhythm Electrophysiol 2012;5:e41–3.
98.Philip F, Muhammad KI, Agarwal S,Natale A, Krasuski RA.Pulmonary vein isolation for the treatment of drug-refractory atrial fi brillation in adults with congenital heart disease.Congenit Heart Dis 2012;7:392–9.
99.Acena M, Anguera I, Dallaglio PD, Rodriguez M, Sabate X.Atrial Fibrillation ablation in adults with repaired congenital heart disease.J Atr Fibrillation 2016;8:1363.
100.Huo Y, Christoph M, Forkmann M,Pohl M, Mayer J, Salmas J, et al.Reduction of radiation exposure during atrial fi brillation ablation using a novel fl uoroscopy image integrated 3-dimensional electroanatomic mapping system: a prospective, randomized, single-blind,and controlled study.Heart Rhythm 2015;12:1945–55.
101.Ueda A, Suman-Horduna I,Mantziari L, Gujic M, Marchese P, Ho SY, et al.Contemporary outcomes of supraventricular tachycardia ablation in congenital heart disease: a single-center experience in 116 patients.Circ Arrhythm Electrophysiol 2013;6:606–13.
102.Wu J, Pflaumer A, Deisenhofer I, Hoppmann P, Hess J, Hessling G.Mapping of atrial tachycardia by remote magnetic navigation in postoperative patients with congenital heart disease.J Cardiovasc Electrophysiol 2010;21:751–9.
103.Ranjan R, Kholmovski EG, Blauer J, Vijayakumar S, Volland NA,Salama ME, et al.Identification and acute targeting of gaps in atrial ablation lesion sets using a real-time magnetic resonance imaging system.Circ Arrhythm Electrophysiol 2012;5:1130–5.
104.Mavroudis C, Backer CL, Deal BJ, Johnsrude C, Strasburger J.Total cavopulmonary conversion and maze procedure for patients with failure of the Fontan operation.J Thorac Cardiovasc Surg 2001;122:863–71.
105.Deal BJ, Costello JM, Webster G,Tsao S, Backer CL, Mavroudis C.intermediate-term outcome of 140 consecutive Fontan conversions with arrhythmia operations.Ann Thorac Surg 2016;101:717–24.
106.Carlson SK, Patel AR, Chang PM.Bradyarrhythmias in congenital heart disease.Card Electrophysiol Clin 2017;9:177–87.
107.Villain E.Indications for pacing in patients with congenital heart disease.Pacing Clin Electrophysiol 2008;31 Suppl 1:S17–20.
108.Wall K, Oddsson H, Ternestedt BM,Jonzon A, Nylander E, Schollin J.Thirty-year electrocardiographic follow-up after repair of tetralogy of Fallot or atrial septal defect.J Electrocardiol 2007;40:214–7.
109.Friedman RA, Will JC, Fenrich AL,Kertesz NJ.Atrioventricular junction ablation and pacemaker therapy in patients with drug-resistant atrial tachyarrhythmias after the Fontan operation.J Cardiovasc Electrophysiol 2005;16:24–9.
110.Stephenson EA, Casavant D, Tuzi J, Alexander ME, Law I, Serwer G,et al.Efficacy of atrial antitachycardia pacing using the Medtronic AT500 pacemaker in patients with congenital heart disease.Am J Cardiol 2003;92:871–6.
111.Drago F, Silvetti MS, Grutter G,De Santis A.Long term management of atrial arrhythmias in young patients with sick sinus syndrome undergoing early operation to correct congenital heart disease.Europace 2006;8:488–94.
112.Khairy P, Landzberg MJ, Gatzoulis MA, Mercier LA, Fernandes SM,Côté JM, et al.Transvenous pacing leads and systemic thromboemboli in patients with intracardiac shunts:a multicenter study.Circulation 2006;113:2391–7.
113.Shah MJ, Nehgme R, Carboni M,Murphy JD.Endocardial atrial pacing lead implantation and midterm follow-up in young patients with sinus node dysfunction after the Fontan procedure.Pacing Clin Electrophysiol 2004;27:949–54.
114.Takahashi K, Cecchin F, Fortescue E, Berul CI, Alexander ME,Walsh EP, et al.Permanent atrial pacing lead implant route after Fontan operation.Pacing Clin Electrophysiol 2009;32:779–85.
115.Newcombe J, Gordon B, Razzouk A, Bailey L, Mandapati R.Extracardiac autologous pericardial tunnel Fontan allows implantation of an endocardial atrial lead for sinus node dysfunction.Ann Thorac Surg 2014;98:1094–6.
116.Moore JP, Shannon KM.Transpulmonary atrial pacing: an approach to transvenous pacemaker implantation after extracardiac conduit Fontan surgery.J Cardiovasc Electrophysiol 2014;25:1028–31.
117.Williams MR, Shepard SM,Boramanand NK, Lamberti JJ,Perry JC.Long-term follow-up shows excellent transmural atrial lead performance in patients with complex congenital heart disease.Circ Arrhythm Electrophysiol 2014;7:652–7.
118.Fox CK, Sidney S, Fullerton HJ.Community-based case-control study of childhood stroke risk associated with congenital heart disease.Stroke 2015;46:336–40.
119.Lanz J, Brophy JM, Therrien J,Kaouache M, Guo L, Marelli AJ.Stroke in adults with congenital heart disease: incidence,cumulative risk, and predictors.Circulation 2015;132:2385–94.
120.Yousef N, Philips M, Shetty I, Cui VW, Zimmerman F, Roberson DA.Transesophageal echocardiography of intracardiac thrombus in congenital heart disease and atrial fl utter: the importance of thorough examination of the Fontan.Pediatr Cardiol 2014;35:1099–107.
121.Heidendael JF, Bokma JP, de Groot JR, Koolbergen DR, Mulder BJ, Bouma BJ.Weighing the risks:thrombotic and bleeding events in adults with atrial arrhythmias and congenital heart disease.Int J Cardiol 2015;186:315–20.
122.Tidake A, Gangurde P, Mahajan A.Congenital left atrial appendage aneurysm associated with a systemic embolism.Cardiol Young 2015;25:597–9.
123.van der Weijde E, van Putte B.Congenital left atrial appendage herniation.Eur J Cardiothorac Surg 2016;49(4):1293.
124.Rosso R, Vexler D, Viskin S,Aviram G.Congenital absence of left atrial appendage.J Cardiovasc Electrophysiol 2014;25:795.
125.Saleh M, Balakrishnan R,Castillo Kontak L, Benenstein R, Chinitz LA, Donnino R, et al.Congenital absence of the left atrial appendage visualized by 3D echocardiography in two adult patients.Echocardiography 2015;32:1206–10.
126.Zeng H, Yu J, Xu Z, Luo Y, Chen H, Zhu H.Giant congenital left atrial appendage aneurysm.J Card Surg 2015;30:646–7.
 Cardiovascular Innovations and Applications2018年2期
Cardiovascular Innovations and Applications2018年2期
- Cardiovascular Innovations and Applications的其它文章
- His Bundle Pacing: Rebirth of an lmportant Technique for Pacing the lntrinsic Conduction System
- Depression in Adults with Congenital Heart Disease: Prevalence, Prognosis,and lntervention
- Traditional Chinese Medicine ls Widely Used for Cardiovascular Disease
- The Fontan Circulation: Contemporary Review of Ongoing Challenges and Management Strategies
- D-Transposition of the Great Arteries: A New Era in Cardiology
- Heart Transplantation for Adult Congenital Heart Disease: Overview and Special Considerations