
Depression in Adults with Congenital Heart Disease: Prevalence, Prognosis,and lntervention
2018-07-04 06:42:56JongMiKoMAandAriCedarsMD2
Jong Mi Ko, MA and Ari M.Cedars, MD2
2Department of Cardiology, Baylor Scott and White Health Care, Dallas, TX, USA
lntroduction
Depression is commonly unrecognized and untreated[1, 2].In the United States, its lifetime prevalence in the general population is 17%.Among those who have major depression, 9% commit suicide and only 50% seek treatment [3].The prevalence of depression in patients with chronic illness is even higher,ranging from 20 to 42% [4–6].In this setting, its insidious impact on health and association with adverse clinical outcomes in patients with chronic illness have been well documented.Depression has been demonstrated to be associated with the development of coronary artery disease, increased somatic symptoms leading to frequent clinic or emergency department visits, increasing frequency and duration of hospitalization, nonadherence to care recommendations, and increased mortality [7–10].Depression thus produces physical, emotional, and financial burdens on patients, their families, and society.Given the known risk of depression in patients with chronic illness, clinicians and researchers in the adult congenital heart disease (ACHD) community have found it critical to assess psychological health status in their patients.With advances in medicine,more than 95% of infants with congenital heart disease (CHD) currently survive to adulthood, in contrast to only 25% in 1950 [11].The number of adults with CHD now exceeds the pediatric CHD population in the Western world [12].As ACHD prevalence increases, there is an ever-increasing emphasis on improving overall health – physical and psychological.As a result, numerous studies have investigated psychological conditions in ACHD patients and their associations with clinical variables, albeit with differing results [13–15].In this review, we summarize existing data on the prevalence of depression, clinical features associated with depression, its prognostic impact, and psychological interventions to treat depression in ACHD patients.
Data on Depression in ACHD
As our goal was to systematically review all published data on depression in ACHD, we searched PubMed, Google Scholar, and Journal/Author Name Estimator for publications using the search terms“depression,” “ACHD,” “adult,” “congenital heart disease,” “review,” “single ventricle,” “Fontan,”“psychosocial,” “intervention,” “mental health,”and “psychopathology.” References in relevant articles were also reviewed to identify publications.Studies including patients aged 18 years or older or with a mean/median age older than 18 years were included.We targeted studies in which depression was clearly differentiated from anxiety or other psychological distress using an independent depression scale.Publications involving a large ACHD database review or a postoperative psychiatric evaluation of ACHD patients were excluded.Non-English publications were also excluded.Searching for all articles up to October 17, 2017, we identified 20 publications meeting these criteria; summaries of the findings are presented in Table 1 [16–35].
Prevalence
ACHD patients have unique characteristics and concerns that might lead to an increased prevalence of depression.These include parental overprotection, disability at early age limiting social functioning, developmental challenges,care transitioning, and chronic medical conditions requiring specialized care, all of which might be anticipated to increase psychological vulnerability[36, 37].This predisposition has been suggested to be a consequence of accumulated, undealt difficulties throughout various developmental stages[37].The reported prevalence of depression in ACHD, however, is highly variable, ranging from 6 to 69% in the studies included here.A significant component of this variability is likely attributable to multiple variables potentially affecting detected versus true prevalence in any given sample.A closer investigation of these variables is informative in defining the nature of depression in the ACHD population.
Some of the variability in reported depression prevalence is undoubtedly due to the setting in which a given study took place.The present review summarizes data from 13 countries on four continents (two countries in North America, two countries in Asia, eight countries in Europe, and Australia) with widely disparate rates of prevalent depression in the general population [17, 24, 25, 38].Furthermore, the samples were drawn exclusively from ACHD-specialized clinics, the populations of which will more or less accurately reflect the actual total ACHD population depending on the nature of the health care system in the country from which the study originated.In the Netherlands, a nationalized health care system increases the probability of care continuity, and the relatively small land area of the country makes specialized care reasonably geographically accessible for the entire population.As such, studies from ACHD-specialized clinics in the Netherlands have a much greater probability of providing a representative sample of the overall ACHD population than those drawn from ACHD-specialized clinics in the United States, where the great majority of ACHD patients either receive no care or are seen in non-ACHD clinics.It should not be surprising then that the reported prevalence of depression might differ widely between and within continents (e.g., Asia, 9–42%; North America,13–33%; Europe, 9–69%).Studies from the United States generally find a higher prevalence compared with normative data, while those from European
countries demonstrate similar or lower rates [24,25, 27, 28, 32, 35].
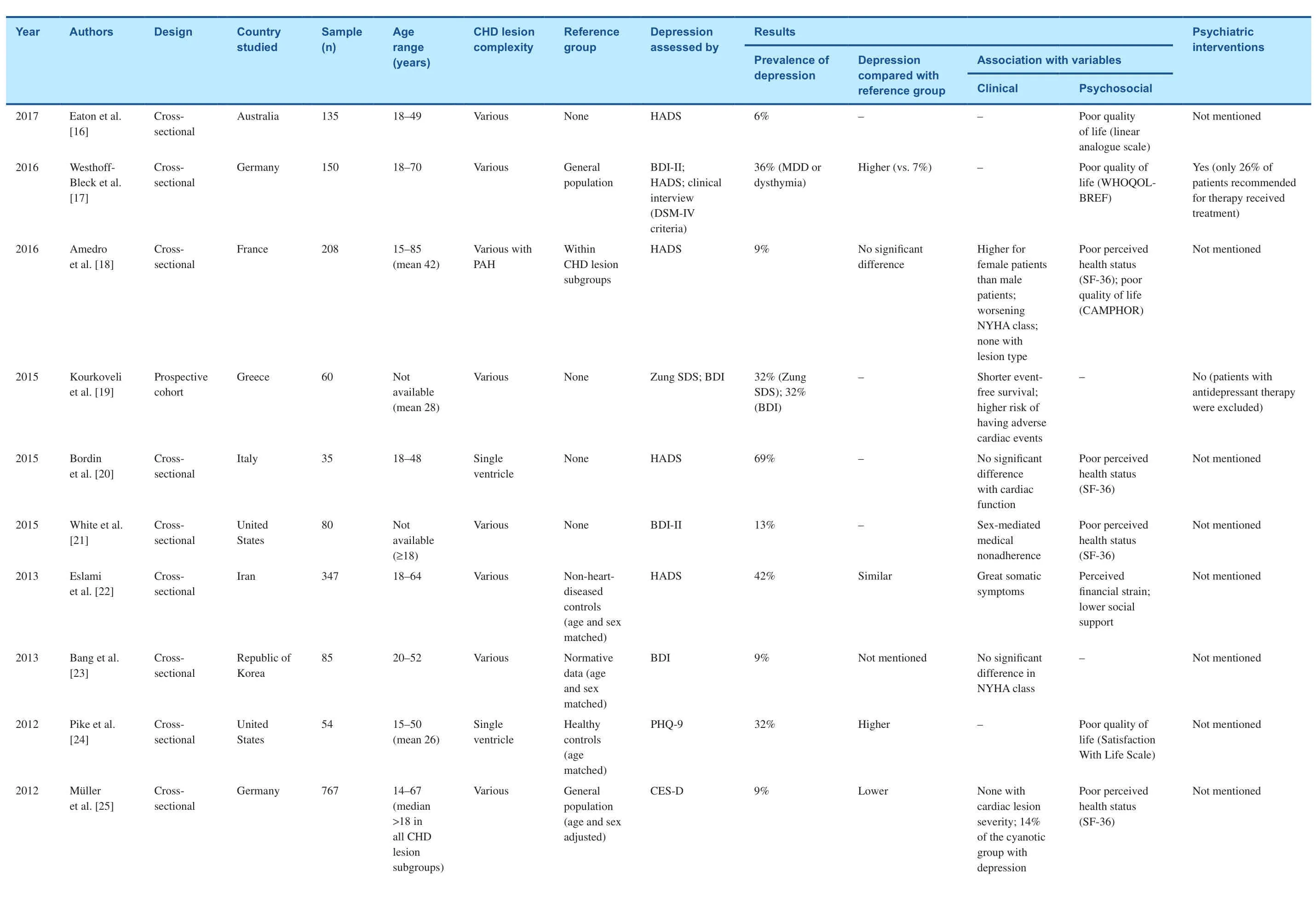
Table 1 Summary of Studies on Depression in Adults with Congenital Heart Disease
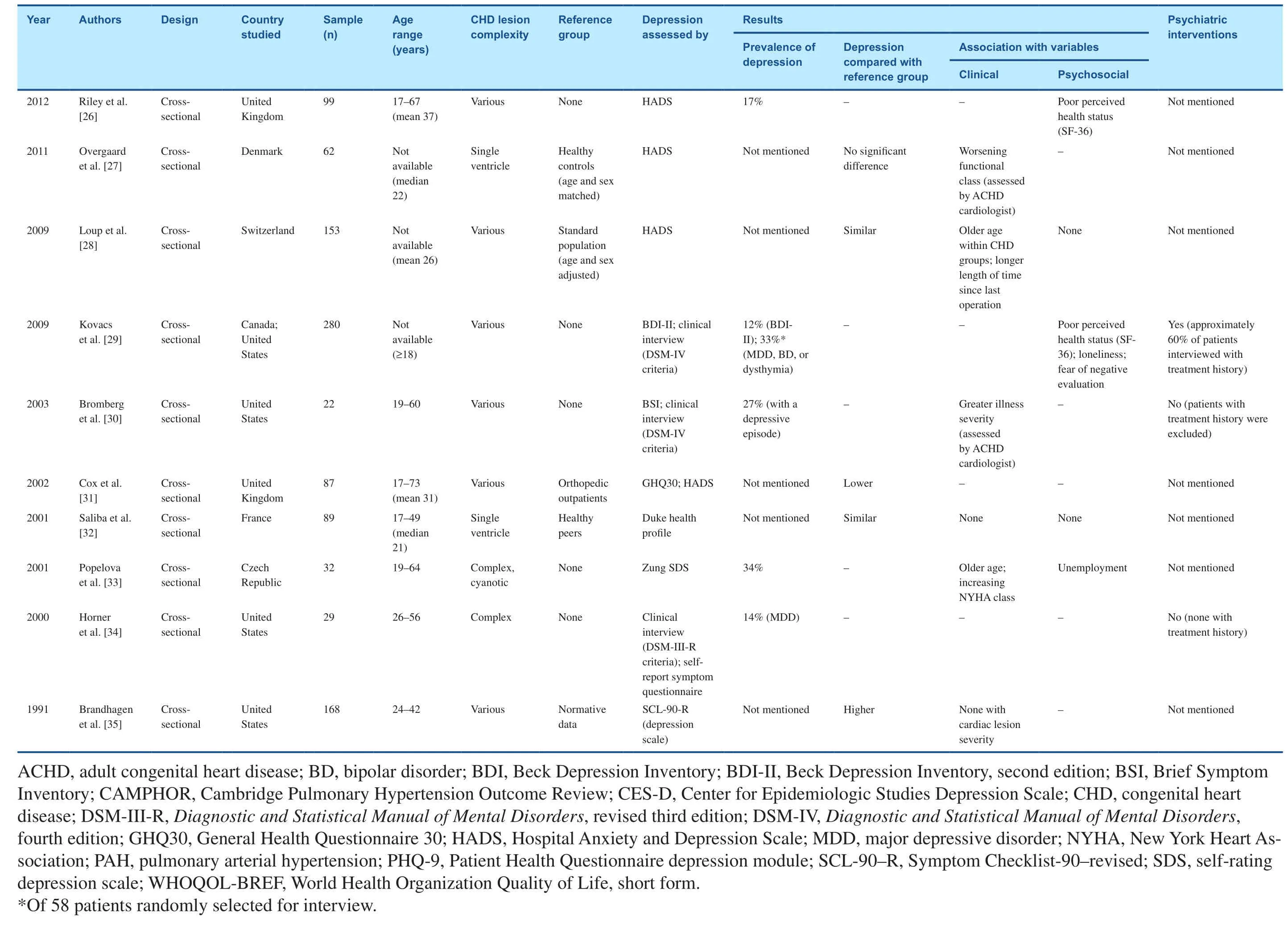
Table 1 (continued)
An additional layer of variability is contributed by differences in the methodology and execution of a particular study.These included differing response rates (lowest, 36%; highest, 100%), type of assessment tools (e.g., self-reported surveys versus a structured psychiatric interview), and sample size, which ranged from 22 to 787 participants (f i ve studies with fewer than 50 participants and eight studies with more than 100 participants).Of particular relevance in this arena was the manner in which depression was identified.Although most of the studies we reviewed used self-reported surveys to screen patients for depression probably for practicality (e.g., shorter time required for assessment,mode of administration convenient for participants and investigators, simple and fast scoring, low costs), on review it appears that structured psychiatric interviews yield more reliable results [17, 29, 30,39].Psychiatric interview is the gold standard for the diagnosis of depression and is used to validate self-administered depression scales, which themselves appear to perform unreliably in this population as well as in heart failure patients [29, 40, 41].Across studies, when a structured psychiatric interview was used for assessment, more patients were found to be depressed as compared with when selfreporting questionnaires were used [17, 29, 30].When Kovacs et al.[29] assessed depression in a population using both psychiatric interview and the Beck Depression Inventory, psychiatric interview found 33% of patients with depression, while the Beck Depression Inventory, second edition, identified only 12% of patients with depression.Further,psychiatric interview has the additional ability to re fine the diagnosis of clinical depression (i.e.,major depressive disorder, bipolar disorder, dysthymia, and other types) and to thereby suggest speci fi c interventions.Studies using a structured psychiatric interview may therefore more accurately re fl ect the actual prevalence of clinical depression, including differential diagnoses in ACHD patients.
With these caveats, ACHD patients as a whole likely have an incidence of depression similar to that of the general population.Among the studies reviewed, nine compared the prevalence of depression with that of a reference group and reported con fl icting results from one another (three higher,four similar, and two lower prevalence in ACHD).Seven studies used the general population as a reference, while two used a sick patient group as a control for comparison.In these latter two studies,when compared with patients who had non-ACHD-related illness, ACHD patients were similarly or less depressed [22, 31].The ACHD population is not monolithic however, and there is signi fi cant variability in the prevalence of depression identified depending on both functional class and lesion.Studies including patients with a lower functional class or lower disease complexity yielded a much lower prevalence of depression.Among the studies we reviewed, in the two with the lowest reported prevalence of depression (6 and 9%), almost all patients (≥98%) had New York Heart Association functional class I or II [16, 23].This may not be surprising as the association of worsening functional status with depression has been well recognized in heart failure patients with normal cardiac anatomy in whom increased New York Heart Association functional class was linked with higher prevalence of depression (11 for class I vs.42% for class IV)[41].
In addition, although depression was not associated with CHD lesion complexity or cardiac function, patients with either chronic cyanosis or a univentricular heart appear to have a higher depression prevalence compared with ACHD patients in other anatomical groups.In three of fi ve studies including exclusively patients with a single ventricle or cyanotic CHD lesions, depression prevalence was consistently higher (32–69%) than in those studies with mixed CHD lesions [20, 24, 33].Given these limited data, we suggest that depression among patients with a univentricular heart or chronic cyanosis requires unique investigation.Intuitively, these patients may be more vulnerable to psychological problems than those with other CHD lesions.In adulthood, these patients experience frequent complications even after successful palliation, including arrhythmia, thromboembolic events, protein-losing enteropathy, hepatic dysfunction, progressive cyanosis with associated complications of hyperviscosity and gout, and abnormal cardiorespiratory response to exercise [42].These clinical symptoms would be anticipated to lead to restrictions in physical, emotional, and social functioning that may result in increased risk of depression [13, 29].Future studies investigating the prevalence of depression specifically in ACHD patients with cyanosis or a single ventricle may therefore be of uniquely high yield.
The studies reviewed revealed several other clinical and psychological variables associated with prevalent depression in ACHD patients.Clinical variables associated with increased depression prevalence included older age, female sex, increased somatic symptoms, nonadherence to care, and longer length of time since the last operation [18,21, 22, 25, 27, 28, 30, 33].The psychosocial variables most frequently associated with depression were poor perceived health status and low quality of life (lower social support, loneliness, fear of negative evaluation, and unemployment were also found to be linked.) [16–18, 20–22, 24–26, 29, 33].
Association with Prognosis
Far from being of only esoteric interest, depression in ACHD appears to predict outcomes.Of 20 reviewed studies, only one was a prospective study and followed up patients for about 5 years to investigate the impact of depression on prognosis.In this study, Kourkoveli et al.[19] found that depression was independently associated with adverse clinical outcomes.They demonstrated that patients with depression had a shorter event-free survival and a two-fold higher risk of death or hospitalization due to heart problems than those without depression.These findings are supported by a retrospective study in which depression was associated with a shorter survival and increased risk of death [43].The possibility of a link between depression and prognosis should not be surprising as it has been consistently demonstrated in other cardiac disease states.An association between depression and increased cardiac events specifically has been demonstrated both among patients with known coronary artery disease and in the general population [44].Furthermore, in patients with heart failure, elevated rates of death and hospitalization have been linked to depression [41].Depression was also associated with poor perceived health status and low quality of life in ACHD.Among the data included in this review, multiple cross-sectional studies identified a correlation between poor perceived health status or quality of life and depression [16–18, 20, 21, 24–26,29].Furthermore, one longitudinal study suggested that persistent depressive symptoms were responsible for poor quality of life and unfavorable perceived health status in young ACHD patients [45].
The causal relationship between depression and prognosis in ACHD is unclear.As ACHD patients age, chronic disease–related complications become more common, and heart failure specifically is a major driver of morbidity and mortality [46].Among patients with heart failure with normal cardiac anatomy, self-assessed health measures are excellent predictors of adverse prognosis, reflecting a link between self-reported health status, depression, and prognosis [47].The data we reviewed suggest a similar association between depression, poor functional class, and poor perceived health status, and a high risk of adverse clinical outcomes is likely to be present as well in ACHD patients.Furthermore,accumulating evidence hints at a possible causal relationship between depression and adverse outcomes.Among depressed male ACHD patients,nonadherence to care as defined by poor follow-up in a specialized ACHD clinic has been reported [21,43].It is possible that depression, by producing negative health behavior, may increase the probability of adverse outcomes given that ACHD-specialized care has been demonstrated to be associated with improved clinical outcomes [48].Whatever the causal relationship is, the adverse association of depression with both a patient’s perceived health status and a patient’s prognosis suggests identifying and treating depression in ACHD is a potentially high-yield area for improving outcomes.
lnterventions
Despite the high prevalence of depression and its adverse prognostic impact, studies on psychiatric treatment for depression in ACHD patients are scarce.Ferguson and Kovacs [36] retrospectively examined 100 ACHD patients who had received psychological assessment at their ACHD-specialized psychological service.Their clients comprised less than 5% of patients followed up clinically in a large ACHD program, of which their center is a part.Twenty-nine percent of reviewed patients metDiagnostic and Statistical Manual ofMental Disorders, fourth edition criteria for clinical depression (23% had major depressive disorder and 6% had dysthymia).Treatment was offered to 87 patients with a diagnosis of any psychiatric disorder, and 14% declined it for unknown reasons.Psychotherapy was the only treatment option offered, and cognitive therapy (92%) was used most frequently.These patients attended a median of eight, 1-h therapy sessions.At the end of treatment, 88% of patients had reduced or no psychological distress.However, this study did not report treatment benef it for patients with depression separately.In the only ongoing prospective study in this population to date, Kovacs et al.[49] developed an eight-session, 90-min intervention program,namedAdult Congenital Heart Disease–Coping and Resilience(ACHD-CARE), and tested its feasibility with a pilot study.On the basis of patientreported needs and wants in treatment collected from previous work, they designed a group therapy with four to six patients facilitated by two therapists [50].Each session presented a different discussion topic with goals to improve psychosocial functioning, quality of life, and resilience through education, cognitive behavior therapy for coping,and social support.Each group consisted of participants of all ages and of various CHD lesion complexities.This study randomized participants evenly into ACHD-CARE and control (i.e., not receiving ACHD-CARE intervention) groups.A 3-month follow-up survey was collected from all participants following completion of the intervention period.This study is ongoing and will determine the feasibility of a full randomized clinical trial using ACHD-CARE in ACHD centers.Further studies on the efficacy of psychiatric interventions in depressed ACHD patients and their effects on prognosis are nevertheless needed.
Even with evidence that treating depression in ACHD is of benef it, substantial changes to care practices will likely be required to enjoy large-scale benef its from this information.Depression itself is quite treatable, with efficacy rates of up to 80%,even among individuals with severe clinical depression [3].However, a major reason for treatment failure is nonadherence.In one study, when treatment was recommended to 62 ACHD patients, only 26%received specific therapy [17].It is possible that the remaining 74% sought mental health services elsewhere at a later time, but this information was not available.One potential reason for this nonadherence to recommended depression care may be that patients are not interested in the type of therapy offered.This possibility is suggested by a comparison of two studies from England and Canada.Despite the higher prevalence of depression in ACHD reported in available data, Diller et al.[43]at the Royal Brompton Hospital in London found that only 3% of 6162 ACHD patients followed up in their clinic between 2000 and 2011 were receiving antidepressant drug therapy.This is likely an underestimation of the actual percentage of patients who were receiving any type of therapy for depression though, as Kovacs et al.[51] in Toronto found that ACHD patients preferred psychotherapy over pharmacotherapy (41 vs.9%).Tailoring therapy to patient preference may thus significantly help in achieving adherence and thereby maximize the benef its of depression therapy.
In addition to nonadherence, the lack of regular screening for and recognition of depression is a huge impediment to successful treatment.The prevalence of unrecognized and untreated depression in ACHD patients is underscored by studies documenting a high prevalence of depression(14, 27, and 32%) among patients without previous or ongoing psychiatric interventions [19, 30,34].In one study, among patients investigated by Bromberg et al.[30] and identified as “emotionally well-adjusted who were not in apparent need of mental health services” by ACHD cardiologists, 27% had a diagnosis of clinical depression.Education in the ACHD community on the importance of depression, its adverse prognostic impact,and broad implementation of effective screening techniques is thus an additional and essential factor required for optimizing psychological care quality.In addition to more reliably identifying patients in need of therapy for depression, there is some suggestion that the treatment adherence rate may increase with an active screening and referral conducted by ACHD clinicians within an established ACHD specialized program.Ferguson and Kovacs[36] observed that among 100 ACHD patients who were referred to their ACHD-specialized psychological service by ACHD specialists as part of routine care, 86% of 87 patients to whom psychotherapy was recommended received treatment.This is a very high rate of adherence compared with that reported in the clinical trial setting.One explanation for this finding might be that most of the patients who actually presented to the psychological service were already determined to proceed with treatment,while patients in research do not anticipate discovering that they have a psychiatric disorder requiring therapy.It is nevertheless possible that psychiatric referral within the established ACHD health care framework provided an opportunity for more thorough education of both clinicians and patients on the importance of psychological problems that resulted in increased awareness and improved receptiveness of patients to therapy.
Conclusions
Despite methodological limitations in existing studies, depression appears at least as common among ACHD patients as in the general population, and has a profound impact on clinical and psychological outcomes.Just as ACHD patients benef it from specialized clinical care for physical conditions, their unique psychological construction may require specialized psychological care.Study results on the efficacy of pharmacotherapy or psychotherapy for depression in patients with or without comorbidity have been conflicting, and practical impediments to the identification and treatment of depression in this population remain [2, 52–56].Given the potential for significantly impacting outcomes, however,investment in further investigation in this arena is warranted.
Conflict of lnterest
The authors declare that they have no conflicts of interest.
REFERENCES
1.Nielsen AC 3rd, Williams TA.Prevalence by self-report questionnaire and recognition by nonpsychiatric physicians.Arch Gen Psychiatry 1980;37:999–1004.
2.Zung WW, Magill M, Moore JT,George DT.Recognition and treatment of depression in a family medicine practice.J Clin Psychiatry 1983;44:3–6.
3.Preston J, O’Neal JH, Talaga MC.Handbook of clinical psychopharmacology for therapists.8th ed.Oakland: New Harbinger Publications; 2017.
4.Burg MM, Abrams D.Depression in chronic medical illness: the case of coronary heart disease.J Clin Psychol 2001;57:1323–37.
5.Chwastiak L, Ehde DM, Gibbons LE, Sullivan M, Bowen JD, Kraft GH.Depressive symptoms and severity of illness in multiple sclerosis: epidemiologic study of a large community sample.Am J Psychiatry 2002;159:1862–8.
6.van Manen JG, Bindels PJ, Dekker FW, IJzermans CJ, van der Zee JS,Schadé E.Risk of depression in patients with chronic obstructive pulmonary disease and its determinants.Thorax 2002;57:412–6.
7.Meijer A, Conradi HJ, Bos EH,Thombs BD, van Melle JP, de Jonge P.Prognostic association of depression following myocardial infarction with mortality and cardiovascular events: a meta-analysis of 25 years of research.Gen Hosp Psychiatry 2011;33:203–16.
8.Barefoot JC, Schroll M.Symptoms of depression, acute myocardial infarction, and total mortality in a community sample.Circulation 1996;93:1976–80.
9.DiMatteo MR, Lepper HS, Croghan TW.Depression is a risk factor for noncompliance with medical treatment:meta-analysis of the effects of anxiety and depression on patient adherence.Arch Intern Med 2000;160:2101–7.
10.Katon WJ.Epidemiology and treatment of depression in patients with chronic medical illness.Dialogues Clin Neurosci 2011;13:7–23.
11.Warnes CA.The adult with congenital heart disease: born to be bad? J Am Coll Cardiol 2005;46:1–8.
12.Marelli AJ, Ionescu-Ittu R, Mackie AS, Guo L, Dendukuri N, Kaouache M.Lifetime prevalence of congenital heart disease in the general population from 2000 to 2010.Circulation 2014;130:749–56.
13.Kovacs AH, Sears SF, Saidi AS.Biopsychosocial experiences of adults with congenital heart disease:review of the literature.Am Heart J 2005;150:193–201.
14.Pauliks LB.Depression in adults with congenital heart disease-public health challenge in a rapidly expanding new patient population.World J Cardiol 2013;5:186–95.
15.Kim GB.Psychosocial adjustment and quality of life of adolescents and adults with congenital heart disease.Korean J Pediatr 2014;57:257–63.
16.Eaton SL, Wang Q, Menahem S.Determinants of quality of life in adults with CHD: an Australian cohort.Cardiol Young 2017;27:1571–6.
17.Westhoff-Bleck M, Briest J,Fraccarollo D, Hilf i ker-Kleiner D,Winter L, Maske U, et al.Mental disorders in adults with congenital heart disease: unmet needs and impact on quality of life.J Affect Disord 2016;204:180–6.
18.Amedro P, Basquin A, Gressin V, Clerson P, Jais X, Thambo JB,et al.Health-related quality of life of patients with pulmonary arterial hypertension associated with CHD:the multicentre cross-sectional ACHILLE study.Cardiol Young 2016;26:1250–9.
19.Kourkoveli P, Rammos S, Parissis J, Maillis A, Kremastinos D,Paraskevaidis I.Depressive symptoms in patients with congenital heart disease: incidence and prognostic value of self-rating depression scales.Congenit Heart Dis 2015;10:240–7.
20.Bordin G, Padalino MA, Perentaler S, Castaldi B, Maschietto N,Michieli P, et al.Clinical profile and quality of life of adult patients after the Fontan procedure.Pediatr Cardiol 2015;36:1261–9.
21.White KS, Pardue C, Ludbrook P,Sodhi S, Esmaeeli A, Cedars A.Cardiac denial and psychological predictors of cardiac care adherence in adults with congenital heart disease.Behav Modif 2016;40:29–50.
22.Eslami B, Sundin O, Macassa G,Khankeh HR, Soares JJ.Anxiety,depressive and somatic symptoms in adults with congenital heart disease.J Psychosom Res 2013;74:49–56.
23.Bang JS, Jo S, Kim GB, Kwon BS,Bae EJ, Noh CI, et al.The mental health and quality of life of adult patients with congenital heart disease.Int J Cardiol 2013;170:49–53.
24.Pike NA, Evangelista LS, Doering LV, Eastwood JA, Lewis AB, Child JS.Quality of life, health status, and depression: comparison between adolescents and adults after the Fontan procedure with healthy counterparts.J Cardiovasc Nurs 2012;27:539–46.
25.Müller J, Hess J, Hager A.Minor symptoms of depression in patients with congenital heart disease have a larger impact on quality of life than limited exercise capacity.Int J Cardiol 2012;154:265–9.
26.Riley JP, Habibi H, Banya W,Gatzoulis MA, Lau-Walker M,Cowie MR.Education and support needs of the older adult with congenital heart disease.J Adv Nurs 2012;68:1050–60.
27.Overgaard D, Schrader AM, Lisby KH, King C, Christensen RF, Jensen HF, et al.Patient-reported outcomes in adult survivors with singleventricle physiology.Cardiology 2011;120:36–42.
28.Loup O, von Weissenfluh C, Gahl B,Schwerzmann M, Carrel T, Kadner A.Quality of life of grown-up congenital heart disease patients after congenital cardiac surgery.Eur J Cardiothorac Surg 2009;36:105–11;discussion 111.
29.Kovacs AH, Saidi AS, Kuhl EA,Sears SF, Silversides C, Harrison JL, et al.Depression and anxiety in adult congenital heart disease: predictors and prevalence.Int J Cardiol 2009;137:158–64.
30.Bromberg JI, Beasley PJ, D’Angelo EJ, Landzberg M, DeMaso DR.Depression and anxiety in adults with congenital heart disease: a pilot study.Heart Lung 2003;32:105–10.
31.Cox D, Lewis G, Stuart G, Murphy K.A cross-sectional study of the prevalence of psychopathology in adults with congenital heart disease.J Psychosom Res 2002;52:65–8.
32.Saliba Z, Butera G, Bonnet D,Bonhoeffer P, Villain E, Kachaner J,et al.Quality of life and perceived health status in surviving adults with univentricular heart.Heart 2001;86:69–73.
33.Popelová J, Slavík Z, Skovránek J.Are cyanosed adults with congenital cardiac malformations depressed?Cardiol Young 2001;11:379–84.
34.Horner T, Liberthson R, Jellinek MS.Psychosocial profile of adults with complex congenital heart disease.Mayo Clin Proc 2000;75:31–6.
35.Brandhagen DJ, Feldt RH, Williams DE.Long-term psychologic implications of congenital heart disease: a 25-year follow-up.Mayo Clin Proc 1991;66:474–9.
36.Ferguson M, Kovacs AH.An integrated adult congenital heart disease psychology service.Congenit Heart Dis 2016;11:444–51.
37.Cornett L, Simms J.At the ‘heart’of the matter: an exploration of the psychological impact of living with congenital heart disease in adulthood.J Health Psychol 2014;19:393–406.
38.Ferrari AJ, Somerville AJ, Baxter AJ, Norman R, Patten SB, Vos T,et al.Global variation in the prevalence and incidence of major depressive disorder: a systematic review of the epidemiological literature.Psychol Med 2013;43:471–81.
39.Segal DL, Hersen M, Van Hasselt VB.Reliability of the structured clinical interview for DSM-III-R:an evaluative review.Compr Psychiatry 1994;35:316–27.
40.Kroenke K, Spitzer RL, Williams JB.The PHQ-9: validity of a brief depression severity measure.J Gen Intern Med 2001;16:606–13.
41.Rutledge T, Reis VA, Linke SE,Greenberg BH, Mills PJ.Depression in heart failure a meta-analytic review of prevalence, intervention effects, and associations with clinical outcomes.J Am Coll Cardiol 2006;48:1527–37.
42.Kaulitz R, Hofbeck M.Current treatment and prognosis in children with functionally univentricular hearts.Arch Dis Child 2005;90:757–62.
43.Diller GP, Bräutigam A, Kempny A, Uebing A, Alonso-Gonzalez R,Swan L, et al.Depression requiring anti-depressant drug therapy in adult congenital heart disease: prevalence, risk factors, and prognostic value.Eur Heart J 2016;37:771–82.
44.Rozanski A, Blumenthal JA, Kaplan J.Impact of psychological factors on the pathogenesis of cardiovascular disease and implications for therapy.Circulation 1999;99:2192–217.
45.Luyckx K, Rassart J, Goossens E, Apers S, Oris L, Moons P.Development and persistence of depressive symptoms in adolescents with CHD.Cardiol Young 2016;26:1115–22.
46.Bredy C, Ministeri M, Kempny A, Alonso-Gonzalez R, Swan L,Uebing A, et al.NYHA classification in adults with congenital heart disease: relation to objective measures of exercise and outcome.Eur Heart J Qual Care Clin Outcomes 2018;4:51–8.
47.Mommersteeg PM, Denollet J,Spertus JA, Pedersen SS.Health status as a risk factor in cardiovascular disease: a systematic review of current evidence.Am Heart J 2009;157:208–18.
48.Mylotte D, Pilote L, Ionescu-Ittu R, Abrahamowicz M, Khairy P,Therrien J, et al.Specialized adult congenital heart disease care: the impact of policy on mortality.Circulation 2014;129:1804–12.
49.Kovacs AH, Bandyopadhyay M,Grace SL, Kentner AC, Nolan RP, Silversides CK, et al.Adult Congenital Heart Disease-Coping and Resilience (ACHD-CARE):rationale and methodology of a pilot randomized controlled trial.Contemp Clin Trials 2015;45:385–93.
50.Pagé MG, Kovacs AH, Irvine J.How do psychosocial challenges associated with living with congenital heart disease translate into treatment interests and preferences?A qualitative approach.Psychol Health 2012;27:1260–70.
51.Kovacs AH, Bendell KL, Colman J,Harrison JL, Oechslin E, Silversides C.Adults with congenital heart disease: psychological needs and treatment preferences.Congenit Heart Dis 2009;4:139–46.
52.van Heeringen K, Zivkov M.Pharmacological treatment of depression in cancer patients.A placebo-controlled study of mianserin.Br J Psychiatry 1996;169:440–3.
53.Glassman AH, O’Connor CM,Califf RM, Swedberg K, Schwartz P, Bigger JT Jr, et al.Sertraline treatment of major depression in patients with acute MI or unstable angina.J Am Med Assoc 2002;288:701–9.Erratum in: JAMA 2002;288:1720.
54.Moncrieff J, Kirsch I.Efficacy of antidepressants in adults.Br Med J 2005;331:155–7.
55.Cowan MJ, Freedland KE, Burg MM, Saab PG, Youngblood ME,Cornell CE, et al.Predictors of treatment response for depression and inadequate social support– the ENRICHD randomized clinical trial.Psychother Psychosom 2008;77(1):27–37.
56.Jones DA, West RR.Psychological rehabilitation after myocardial infarction: multicentre randomised controlled trial.Br Med J 1996;313:1517–21.
 Cardiovascular Innovations and Applications2018年2期
Cardiovascular Innovations and Applications2018年2期
- Cardiovascular Innovations and Applications的其它文章
- His Bundle Pacing: Rebirth of an lmportant Technique for Pacing the lntrinsic Conduction System
- Traditional Chinese Medicine ls Widely Used for Cardiovascular Disease
- The Fontan Circulation: Contemporary Review of Ongoing Challenges and Management Strategies
- D-Transposition of the Great Arteries: A New Era in Cardiology
- Heart Transplantation for Adult Congenital Heart Disease: Overview and Special Considerations
- Atrial Arrhythmias lncluding Atrial Fibrillation in Congenital Heart Disease: Mechanisms,Substrate ldentification and lnterventional Approaches