
Heart Transplantation for Adult Congenital Heart Disease: Overview and Special Considerations
2018-07-04 06:40:04DipankarGuptaMDJanaReidARNPDiegoMoguillanskyMDMSRenataShihMDMarkBleiweisMDFrederickFrickerMDandBiagioPietraMD
Dipankar Gupta, MD, Jana Reid, ARNP, Diego Moguillansky, MD, MS, Renata Shih, MD,Mark S.Bleiweis, MD, Frederick J.Fricker, MD and Biagio A.Pietra, MD
lntroduction
Success in the management of congenital heart disease (CHD) in the young is leading to an increasing number of heart transplants in adults with CHD.CHD has an incidence of 0.8–1%, translating to approximately 40,000 newborns per year[1, 2].With improving surgical and interventional techniques and medical management, approximately 90% of children with CHD survive to adulthood [3].On the basis of a recent study, there are approximately 2.4 million people in the United States with CHD.On the basis of this study, the estimated number of adults with CHD in the United States is approximately 1.4 million.The population of adults with CHD in 2010 demonstrated a 63%increase when compared with the estimates from 2000, making it the fastest growing population in congenital cardiology.In addition, approximately 300,000 patients of the 1.4 million adults with CHD have evidence of severe CHDs [4].Adult CHD(ACHD) is associated with multiple morbidities secondary to the original anatomic substrate, multiple palliative procedures, and associated complications.Unfortunately, despite improved surgical and medical management, approximately 10–20%patients with CHD progress to end-stage heart failure as adults [5], and it is the most common cause of late death in patients with ACHD [6, 7].
ACHD patients are an extremely complex group of patients to manage.ACHD brings unique challenges in medical care that is influenced by a variety of different factors.These factors include initial anatomy and physiology, multiple palliative procedures, multiple sternotomies, bystander organ dysfunction, elevated pulmonary vascular resistance (PVR), and chronic heart failure [8, 9].In a study by Oechslin et al.[7], congenitally corrected transposition of the great arteries, tricuspid atresia,and univentricular connection were associated with the highest mortality, with the mean age at death of 37 ± 15 years.As the population of ACHD patients continues to rise, increasing numbers of these patients will need to be evaluated for heart transplantation.Historically the outcomes for heart transplantation in ACHD patients have been considered worse than in patients with acquired cardiovascular disease, typically related to their complex anatomy,higher incidence and severity of preformed antibodies, prior cardiovascular surgery, and complex vascular connections.Patients with ACHD listed for heart transplantation are younger and have fewer comorbid conditions than patients with acquired heart disease [10].Patients with ACHD have high perioperative mortality (16–25%), with better longterm survival [9–12].Therefore, before selection for transplant candidacy, all these factors must be taken into consideration for accurate prognostication.
Assessment and Management of Heart Failure in ACHD
Patients with ACHD should be followed up by physicians with expertise in ACHD as they have high familiarity with the unique anatomy and physiology, the surgical approaches, and the associated complications.Patients with ACHD may remain falsely asymptomatic because of younger age and lifelong adaptations that may limit accurate assessment of functional capacity [13].Early recognition of worsening heart failure is extremely important,as these patients may be candidates for optimization of medical management of heart failure therapy,surgical intervention depending on anatomy and residual lesions, and recognition of development of renal or liver dysfunction.In our experience, early surgical intervention for worsening atrioventricular valve regurgitation in patients with atrial switch or congenitally corrected transposition of the great arteries may delay the need for heart transplantation.Similarly, Fontan revision to improve fl ow dynamics and address difficult-to-treat atrial arrhythmias has demonstrated reduction in symptoms of heart failure,delaying the need for heart transplantation in patients with univentricular circulation.In addition to the usual features of advanced heart failure, ACHD patients may have some specific presentations, which may prompt evaluation for heart transplantation:
• Worsening cyanosis and arteriovenous malformations.
• Conditions that cause increasing or fi xed PVR.
• Progressive deterioration in renal or liver function.
• Protein-losing enteropathy or plastic bronchitis in Fontan patients.
• Worsening atrioventricular valve regurgitation.
• Changes in the surgical approach in the management of CHD over the years influence the presentation and onset of heart failure.
Therefore early referral to an advanced heart failure team should be recommended.In the scientific statement from the American Heart Association regarding transplantation and mechanical circulatory support in CHD, Ross et al.[14] provide an excellent algorithm for assessment and treatment of ACHD patients with advanced heart failure.On the basis of the consensus statement, any patient with CHD and heart failure needs to be assessed for worsening symptoms, including exercise intolerance and available biomarkers.Hemodynamic evaluation must be considered, with the aim to optimize medical therapy and consider device therapy or percutaneous or surgical intervention.In the event that these options are not viable, then evaluation for transplantation and/or mechanical circulatory support should be initiated.Use of mechanical circulatory support is less common in patients with CHD compared with those with other forms of heart disease [15] because patients with CHD have complex anatomy, have more scarring because of previous surgical procedures, and are more likely to have elevated PVR and multiorgan dysfunction.Additionally, currently available devices are often suboptimal for use in this patient population.Decreased use of mechanical circulatory support causes lower listing status and decreased organ allocation, which Gelow et al.have argued is justif ication for separate priority listing criteria for organ allocation for patients with CHD.However, there are counterarguments to not change the organ allocation criteria and continue to equitably allocate organs to the one with the greatest need while optimizing posttransplant survival outcomes [16].
Demographics and Statistics of Adult Heart Transplantation with a Focus on ACHD
From the 2017 International Society for Heart &Lung Transplantation (ISHLT) heart transplant statistics, 135,387 heart transplants had been performed from Jan 1982 to June 30, 2016, of which 120,991 had been in adults.While adults with CHD represent a small percentage of patients undergoing transplantation, there has been a slight increase in the recent era.Figure 1 shows a breakdown of the various diagnoses for heart transplantation from January 1982 to June 2016 and from January 2009 to June 2016 [17].Of note, patients with ACHD were younger at the time of transplantation, as demonstrated in Figure 2, constituting 11% in the age group from 18 to 39 years.In the recent era there has been a significant increase in the use of mechanical circulatory support use as a bridge to transplantation in adults (see Figure 3), but this change seems to have affected the ACHD population to a lesser degree because of their challenging anatomy.In the ACHD population, patients are more likely to present with biventricular systolic dysfunction,pulmonary hypertension, or evidence of multiorgan involvement, such that some of these patients may require combined organ transplantation.Figure 4 shows the frequency of combined organ transplantation in adults, with heart-kidney transplantation being the most common, followed by heart-liver transplantation.The 1-year survival rate after heart transplantation for adults is shown in Figure 5, with a lower survival rate early after transplantation for ACHD, which increases after the perioperative period.The median survival in adults with CHD after heart transplantation is 15 years, which is higher than for the other categories (Figure 6).With regard to the Kaplan-Meier survival by diagnosis conditional on survival to 1 year, the median survival of patients with ACHD after transplantation is 19.5 years (Figure 7), significantly longer than for the other categories.These statistics suggest that despite the early higher mortality in the ACHD population, their long-term outcomes are better or at least not worse than those of the other categories.
Special Considerations and lndications for Heart Transplantation in ACHD Patients

Figure 1 Adult Heart Transplants by Diagnosis.
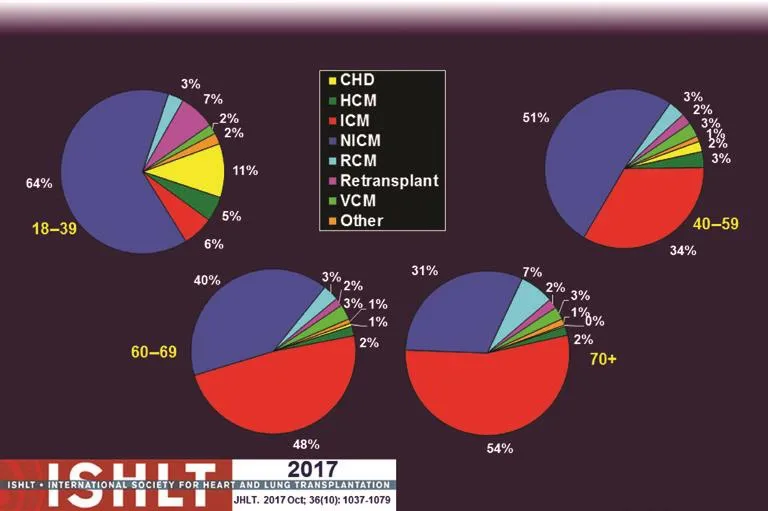
Figure 2 Adult Heart Transplants: Diagnosis by Age Group (Transplants from January 2009 to June 2016).

Figure 3 Adult Heart Transplants: Percentage of Patients Bridged with Mechanical Circulatory Support by Year and Device Type.

Figure 4 Adult Heart Transplants: Number and Percentage of Combined Organ Transplants Reported by Year and Type of Transplant.
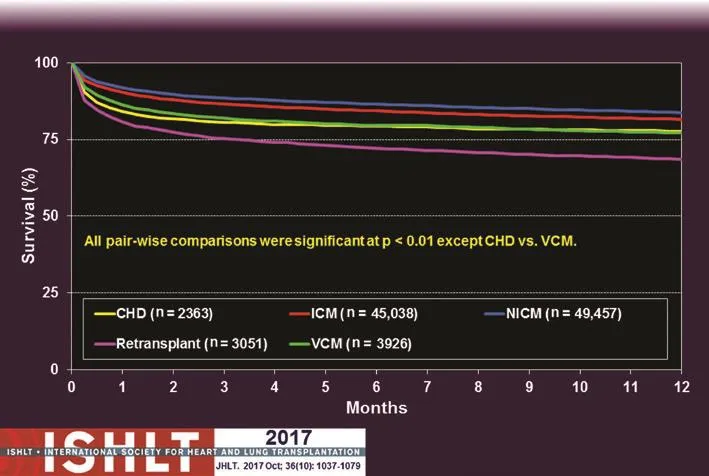
Figure 5 Adult Heart Transplants: Kaplan-Meier Survival within 1 year by Diagnosis (Transplants from January 1982 to June 2015).
There is currently no clear consensus on the indications for heart transplantation in ACHD patients.According to the most recent 10-year update on heart transplant listing criteria, the ISHLT provided class I–III recommendations in a special section for CHD, covering adults and children [18].According to the 2016 ISHLT recommendations, heart transplantation should be performed only at centers with established medical and surgical experience in both ACHD and transplantation (class I, level of evidence C).Detailed assessment of anatomic and vascular abnormalities, PVR, assessment of chronic or previous infections, qualitative and quantitative HLA antibody, assessment of other organ dysfunction, and psychosocial evaluation must be performed(class I, level of evidence C).Heart transplantation should be considered in certain conditions with or without the presence of ventricular dysfunction.These conditions may include stenosis/atresia in proximal coronary arteries, severe stenosis/insufficiency in atrioventricular valves, severe hypoxia,protein-losing enteropathy and/or plastic bronchitis associated with CHD, and pulmonary hypertension with the risk of developing fi xed elevated PVR in the future (class IIa, level of evidence C).The ISHLT also recommended that heart transplantation should be contraindicated in patients with severe irreversible multisystem disease; however, multiorgan transplantation may be considered (class III, level of evidence C).Similarly, patients with severe hypoplasia of central pulmonary arteries or pulmonary veins should not be considered for heart transplantation alone (class III, level of evidence C)[18].Tables 1 and 2 outline the indications and contraindications for heart transplantation in ACHD patients.
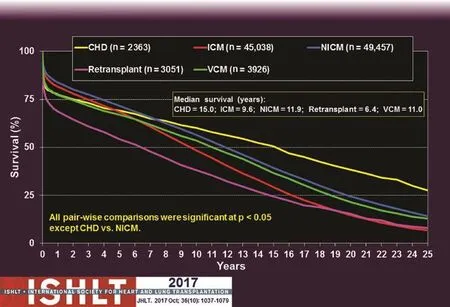
Figure 6 Adult Heart Transplants: Kaplan-Meier Survival by Diagnosis (Transplants from January 1982 to June 2015).CHD, congenital heart disease; ICM, ischemic cardiomyopathy; NICM, nonischemic cardiomyopathy; VCM, viral cardiomyopathy.
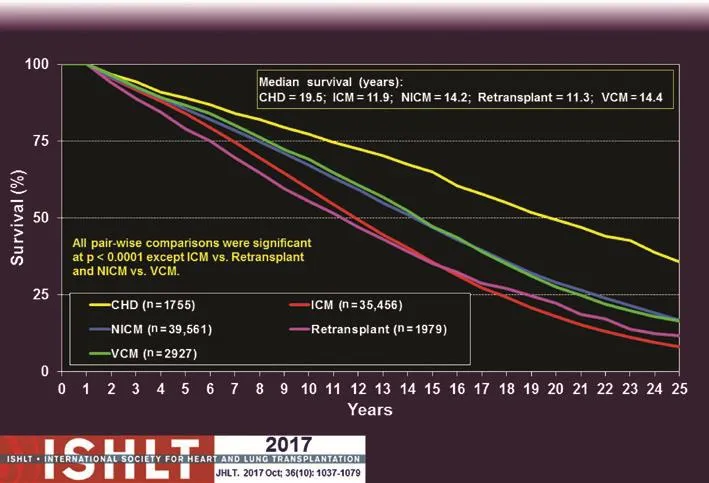
Figure 7 Adult Heart Transplants: Kaplan-Meier Survival by Diagnosis Conditional on Survival to 1 year (Transplants from January 1982 to June 2015).
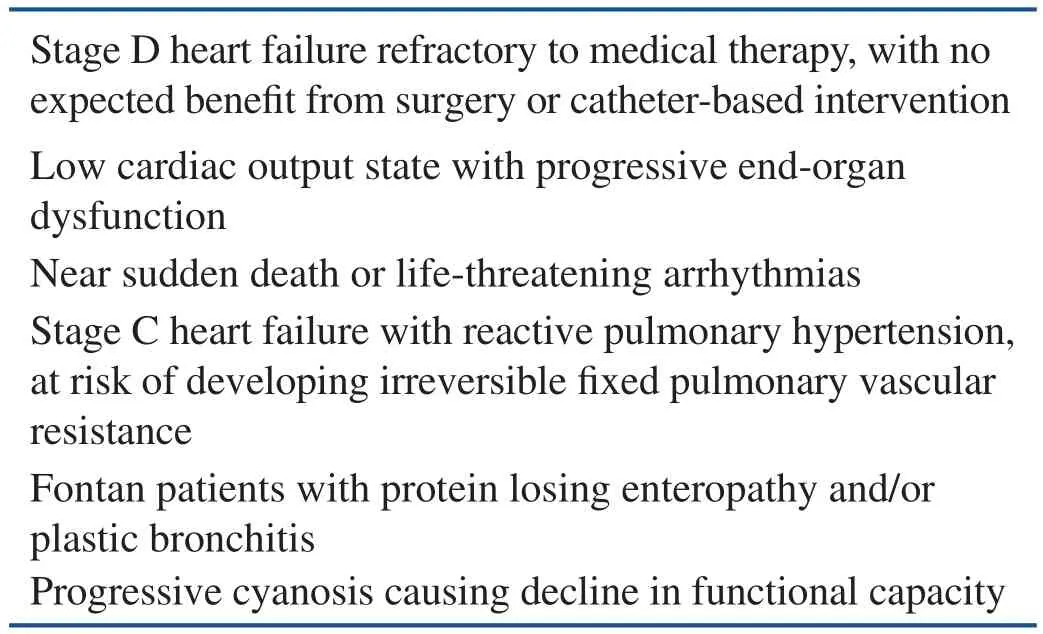
Table 1 Indications for Heart Transplantation for Adult Congenital Heart Disease.
Our Experience
At our center, we have a dedicated and robust ACHD program comprising two ACHD cardiologists, physician extenders, and two congenital cardiothoracic surgeons who work in conjunction with the adult heart failure/heart transplant team for the care of these patients.From January 2005 to June 2017, 269 patients older than 18 years underwent transplantation.Of these, 15 patients (5.5%) underwent transplantation for CHD.The anatomic details of the patients who underwent transplantation for CHD are given in Table 3.In the group with CHD,the median waiting time for transplantation was 228 days (interquartile range 77–408 days, range 45–1142 days).There were no waiting list deaths.A significant number of patients were presensitized, resulting in a panel reactive antibody titer ranging from 32% to 86%.The patients with CHD had undergone multiple prior cardiac surgical procedures (median 3, interquartile range 3–4).In the CHD group, the 1-year survival rate after transplantation was 100%.In comparison with the general population, 201 of 230 patients (87.4%) survived for at least 1 year, and 244 of 252 patients (96.8%)survived for at least 30 days after transplantation.In our experience, despite long waiting times, variable and sometimes extensive allosensitization, and numerous prior cardiac surgical procedures, the short- and intermediate-term outcomes for ACHD patients undergoing heart transplantation appear to be no worse than in the general population.
Special Considerations
Single Ventricle Physiology
Fontan and Baudet [19] initially reported the Fontan procedure to completely separate the systemic and pulmonary circulations in a patient with tricuspid atresia in 1971.Since then, it has undergone evolution from atriopulmonary connection, modifiedclassic Fontan procedure, and intracardiac lateral tunnel to the currently performed extracardiac Fontan procedure to improve the fl ow dynamics and decrease the long-term morbidities.The Fontan procedure is now performed as the final-stage palliation in patients who cannot have a biventricular repair, as it helps reduce hypoxia and eliminates cyanosis.Despite the tremendous success of this life-saving procedure, it continues to be associated with long-term morbidities.The Fontan physiology is usually associated with mean systemic venous pressure greater than 10 mmHg and mean pulmonary arterial pressure less than 15 mmHg.Fontan physiology is associated with a wide variety of complications, and most of them are related to systemic venous hypertension.In the current era,the perioperative mortality with the Fontan procedure is less than 2%.The Fontan procedure has been demonstrated to have rates of freedom from all-cause death and heart transplantation of 90%at 10 years, 83% at 20 years, and 70% at 25 years[20].The Fontan procedure can be associated with sudden death, most likely secondary to arrhythmias.Otherwise, the presence of intracardiac thrombus and the lack of antiplatelet/anticoagulant therapy were identified to be independent risk factors for thromboembolic death.Protein-losing enteropathy,single morphologic right ventricle and elevated right atrial pressure are independent risk factors for death associated with heart failure [20].The frequency of systolic and diastolic ventricular dysfunction after the Fontan procedure is 27% and 72%, respectively,on the basis of a multicenter study by the Pediatric Heart Network [21].There has been increasing evidence of improvement in functional capacity, global and diastolic ventricular function, and myocardial performance index with use of sildenafil in adult patients with heart failure [22].There are a multitude of other chronic problems associated with the Fontan procedure, including growth failure, cyanosis, liver dysfunction, coagulation abnormalities,protein-losing enteropathy, plastic bronchitis, and arrhythmias [23].Fontan physiology in the long term has a likelihood of failure most commonly due to increasing venous pressures and progressively decreasing cardiac output.This causes a decline in functional capacity at a rate of 2.6% per year after adolescence, with some exceptions [24–26].Liver dysfunction is commonly seen because of congestive hepatopathy in the setting of chronic passive congestion, which can lead to fi brosis and cirrhosis.There is a complex interplay of multiple factors in the Fontan circulation, which require very frequent monitoring by an ACHD cardiologist to improve the long-term outcomes.As more and more patients undergo this procedure, a higher number are bound to need heart transplantation in the future.
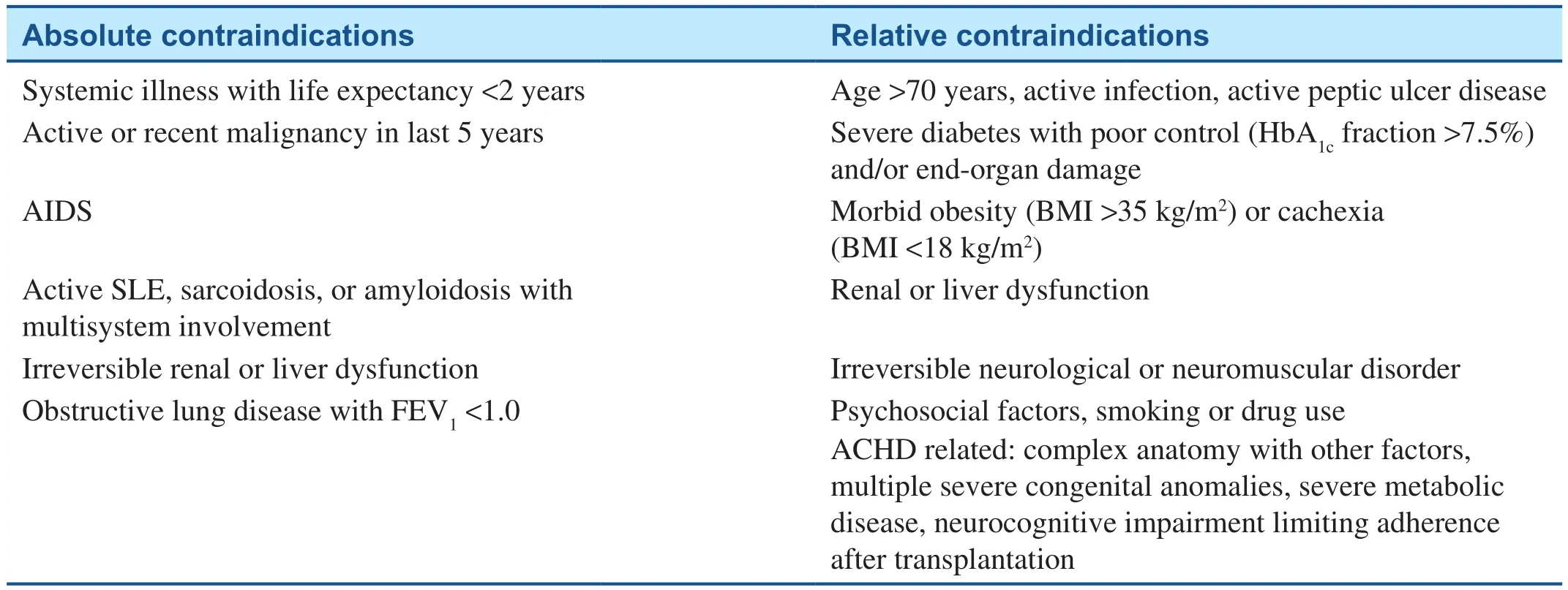
Table 2 Contraindications for Heart Transplantation for Adult Congenital Heart Disease (ACHD).
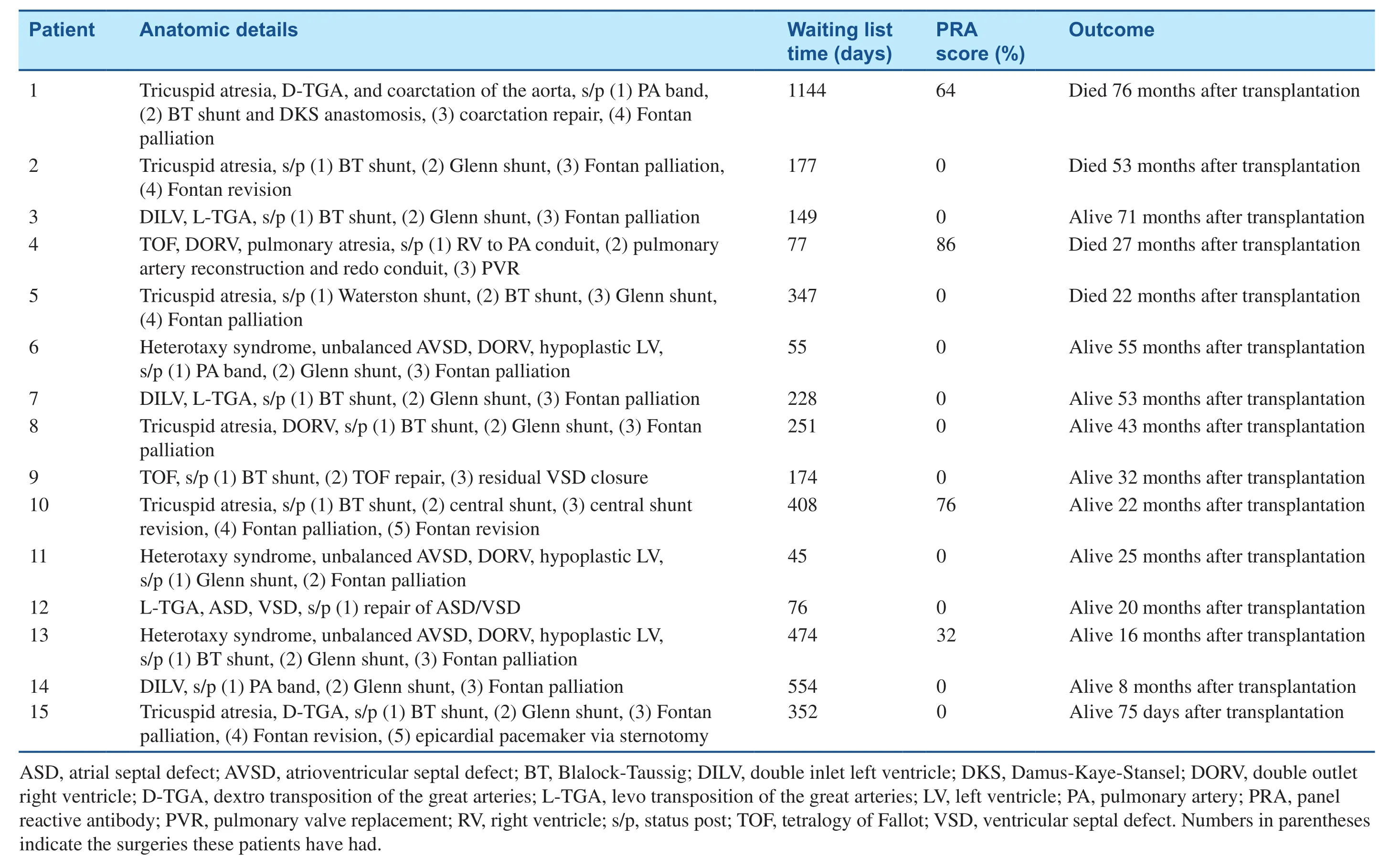
Table 3 Anatomic Details,Waiting List Time,Sensitization,and Outcomes of Patients Who Underwent Transplantation at Our Institution for Adult Congenital Heart Disease
Pulmonary Hypertension
Elevated PVR is seen commonly in ACHD patients[27].In a study by Krishnamurthy et al.[27], of 983 ACHD patients, 22% had evidence of pulmonary hypertension as evidenced by elevated transpulmonary gradient [27].In patients with pulmonary hypertension, there is higher waiting list mortality;however, the long-term outcomes appear to be similar.With advancements in oral pulmonary hypertension medications, targeted therapy can be used with repeated hemodynamic assessment before the candidacy for transplantation is determined.Rarely,heart-lung transplantation may be considered in ACHD patients with pulmonary hypertension and no response to therapy.
Other Factors
Patients with ACHD have undergone multiple previous surgical procedures, which increase the complexity of the transplant procedure itself because of a higher risk of bleeding.Patients with chronic cyanosis and univentricular palliation are especially prone to the formation of arteriovenous and venovenous collaterals.Patients with ACHD have a higher incidence of primary graft failure, stroke,multiorgan failure, and hemorrhage in the postoperative period [9, 28].In our experience, the median number of surgical procedures before transplantation is three.
With increasing number of freestanding children’s hospitals, patients with ACHD may have a difficult time finding an optimal balance for their care [3].Goldberg et al.[29] suggest improved survival in ACHD patients if the transplantation is performed at a high-volume center, especially at centers that perform pediatric transplants.Further, Mori at al.[30] document that heart transplantation in ACHD patients has improved survival when performed by a congenital cardiothoracic surgeon.In our institution,a congenital cardiothoracic surgeon performs transplantation in all patients with ACHD.In our opinion, patients with ACHD are different from the usual adult heart transplant patients and therefore they need a multidisciplinary approach for optimal care.
Patients with ACHD have higher chances of having preformed HLA antibodies.This is for multiple reasons, including previous surgical procedures, cardiopulmonary bypass, pregnancy, and exposure to multiple blood transfusions.Additionally, homograft material used in previous palliative surgical procedures can be antigenic and lead to allosensitization.Depending on the quantity and strength of the antibodies, some patients may require desensitization therapies with agents such as rituximab and/or bortezomib, as well as plasmapheresis.However, none of these therapies are an accepted strategy or a universally effective therapy.Subsequently, after transplantation and donor tissue exposure there is a likelihood of formation of de novo donor-specific HLA antibodies.The presence of presensitization increases the risk of the need for organ transplantation.Multiple studies have evaluated the effect of presensitization on graft survival, antibody-mediated rejection, and development of coronary vasculopathy.
Patients with ACHD have a history of multiple surgical procedures and procedures for palliation of their CHD.Because of the complexity of these procedures, there may be a delay in the normal developmental milestones.These patients are at high risk of chronic lifelong disability, which can essentially cause a delayed adulthood with increased need for ancillary services/therapies.Therefore ACHD patients are at higher risk of attention deficit disorder, anxiety, depression, and posttraumatic stress disorder [31–33].Social evaluation, including detailed assessment of social support, previous nonadherence to therapy, high-risk behaviors, smoking, and alcohol and drug use, must be performed.Currently,there is no consensus for a uniform systematic approach in these situations, but these factors can exert a strong influence on posttransplant outcomes.
Conclusion
In conclusion, the cohort of ACHD patients is increasing significantly.There is a high likelihood for the need for heart transplantation as these patients develop chronic heart failure and other chronic sequelae of palliated CHD.It is important to recognize advanced heart failure and other associated complications early in this cohort of complex patients for early referral to an ACHD specialist.Because of the presence of multiple factors that can affect the long-term outcomes, there needs to be a careful selection process for transplantation to optimize the utilization of donor organs.Our experience with transplantation in ACHD patients demonstrates excellent short-term outcomes; however,the timing of transplantation is a huge challenge,mostly related to other end-organ dysfunction.Further studies are needed to continue to improve the outcomes after transplantation.
Conflict of lnterest
The authors have no conflicts of interest.
REFERENCES
1.Gupta D, Chandran A.Cardiac magnetic resonance imaging and computed tomography in newborns with congenital heart disease.NeoReviews 2015;16(6):e362–e77.
2.Centers for Disease Control and Prevention.Congenital heart defects:data and statistics.2017 [cited 2017 November 1].Available from:https://www.cdc.gov/ncbddd/heartdefects/data.html.
3.Crumb SR, Cook SC, Cheatham JP,Galantowicz M, Feltes TF, Phillips A, et al.Quality outcomes of ACHD patients undergoing cardiovascular procedures and hospital admissions in a free-standing children’s hospital.Int J Cardiol 2011;146(3):326–9.
4.Gilboa SM, Devine OJ, Kucik JE,Oster ME, Riehle-Colarusso T,Nembhard WN, et al.Congenital heart defects in the United States:estimating the magnitude of the affected population in 2010.Circulation 2016;134(2):101–9.
5.Coskun O, Coskun T, El-Arousy M,Parsa MA, Reiss N, Blanz U, et al.Heart transplantation in adults with congenital heart disease: experience with 15 patients.ASAIO J 2007;53(1):103–6.
6.Nieminen HP, Jokinen EV, Sairanen HI.Causes of late deaths after pediatric cardiac surgery: a populationbased study.J Am Coll Cardiol 2007;50(13):1263–71.
7.Oechslin EN, Harrison DA,Connelly MS, Webb GD, Siu SC.Mode of death in adults with congenital heart disease.Am J Cardiol 2000;86(10):1111–6.
8.Lewis M, Ginns J, Schulze C,Lippel M, Chai P, Bacha E, et al.Outcomes of adult patients with congenital heart disease after heart transplantation: impact of disease type, previous thoracic surgeries,and bystander organ dysfunction.J Card Fail 2016;22(7):578–82.
9.Patel ND, Weiss ES, Allen JG,Russell SD, Shah AS, Vricella LA, et al.Heart transplantation for adults with congenital heart disease:analysis of the United Network For Organ Sharing database.Ann Thorac Surg 2009;88(3):814–21;discussion 821–2.
10.Davies RR, Russo MJ, Yang J,Quaegebeur JM, Mosca RS, Chen JM.Listing and transplanting adults with congenital heart disease.Circulation 2011;123(7):759–67.
11.Izquierdo MT, Almenar L, Martinez-Dolz L, Moro J, Aguero J, Sanchez-Lazaro I, et al.Mortality after heart transplantation in adults with congenital heart disease: a singlecenter experience.Transplant Proc 2007;39(7):2357–9.
12.Lamour JM, Kanter KR, Naftel DC, Chrisant MR, Morrow WR,Clemson BS, et al.The effect of age, diagnosis, and previous surgery in children and adults undergoing heart transplantation for congenital heart disease.J Am Coll Cardiol 2009;54(2):160–5.
13.Burchill LJ.Heart transplantation in adult congenital heart disease.Heart 2016;102(23):1871–7.
14.Ross HJ, Law Y, Book WM, Broberg CS, Burchill L, Cecchin F, et al.Transplantation and mechanical circulatory support in congenital heart disease: a scientific statement from the American Heart Association.Circulation 2016;133(8):802–20.
15.Gelow JM, Song HK, Weiss JB,Mudd JO, Broberg CS.Organ allocation in adults with congenital heart disease listed for heart transplant: impact of ventricular assist devices.J Heart Lung Transplant 2013;32(11):1059–64.
16.Bhama JK.Leveling the playing fi eld in adult heart transplantation.J Heart Lung Transplant 2013;32(11):1052–3.
17.Lund LH, Khush KK, Cherikh WS,Goldfarb S, Kucheryavaya AY,Levvey BJ, et al.The Registry of the International Society for Heart and Lung Transplantation: thirtyfourth adult heart transplantation report-2017; focus theme: allograft ischemic time.J Heart Lung Transplant 2017;36(10):1037–46.
18.Mehra MR, Canter CE, Hannan MM,Semigran MJ, Uber PA, Baran DA,et al.The 2016 International Society for Heart Lung Transplantation listing criteria for heart transplantation: a 10-year update.J Heart Lung Transplant 2016;35(1):1–23.
19.Fontan F, Baudet E.Surgical repair of tricuspid atresia.Thorax 1971;26(3):240–8.
20.Khairy P, Fernandes SM, Mayer JE,Jr., Triedman JK, Walsh EP, Lock JE, et al.Long-term survival, modes of death, and predictors of mortality in patients with Fontan surgery.Circulation 2008;117(1):85–92.
21.Anderson PA, Sleeper LA, Mahony L, Colan SD, Atz AM, Breitbart RE, et al.Contemporary outcomes after the Fontan procedure:a Pediatric Heart Network multicenter study.J Am Coll Cardiol 2008;52(2):85–98.
22.Guazzi M, Vicenzi M, Arena R,Guazzi MD.PDE5 inhibition with sildenafil improves left ventricular diastolic function, cardiac geometry,and clinical status in patients with stable systolic heart failure: results of a 1-year, prospective, randomized,placebo-controlled study.Circ Heart Fail 2011;4(1):8–17.
23.Mondesert B, Marcotte F, Mongeon FP, Dore A, Mercier LA, Ibrahim R, et al.Fontan circulation: success or failure? Can J Cardiol 2013;29(7):811–20.
24.Fernandes SM, McElhinney DB,Khairy P, Graham DA, Landzberg MJ, Rhodes J.Serial cardiopulmonary exercise testing in patients with previous Fontan surgery.Pediatr Cardiol 2010;31(2):175–80.
25.Paridon SM, Mitchell PD, Colan SD, Williams RV, Blaufox A, Li JS, et al.A cross-sectional study of exercise performance during the fi rst 2 decades of life after the Fontan operation.J Am Coll Cardiol 2008;52(2):99–107.
26.Giardini A, Hager A, Pace Napoleone C, Picchio FM.Natural history of exercise capacity after the Fontan operation: a longitudinal study.Ann Thorac Surg 2008;85(3):818–21.
27.Krishnamurthy Y, Cooper LB, Lu D, Schroder JN, Daneshmand MA,Rogers JG, et al.Trends and outcomes of patients with adult congenital heart disease and pulmonary hypertension listed for orthotopic heart transplantation in the United States.J Heart Lung Transplant 2016;35(5):619–24.
28.Karamlou T, Hirsch J, Welke K,Ohye RG, Bove EL, Devaney EJ,et al.A United Network for organ sharing analysis of heart transplantation in adults with congenital heart disease: outcomes and factors associated with mortality and retransplantation.J Thorac Cardiovasc Surg 2010;140(1):161–8.
29.Goldberg SW, Fisher SA, Wehman B, Mehra MR.Adults with congenital heart disease and heart transplantation: optimizing outcomes.J Heart Lung Transplant 2014;33(9):873–7.
30.Mori M, Vega D, Book W, Kogon BE.Heart transplantation in adults with congenital heart disease:100% survival with operations performed by a surgeon specializing in congenital heart disease in an adult hospital.Ann Thorac Surg 2015;99(6):2173–8.
31.Kovacs AH, Saidi AS, Kuhl EA,Sears SF, Silversides C, Harrison JL, et al.Depression and anxiety in adult congenital heart disease:predictors and prevalence.Int J Cardiol 2009;137(2):158–64.
32.Norozi K, Zoege M, Buchhorn R, Wessel A, Geyer S.The influence of congenital heart disease on psychological conditions in adolescents and adults after corrective surgery.Congenit Heart Dis 2006;1(6):282–8.
33.Ong L, Nolan RP, Irvine J, Kovacs AH.Parental overprotection and heart-focused anxiety in adults with congenital heart disease.Int J Behav Med 2011;18(3):260–7.
 Cardiovascular Innovations and Applications2018年2期
Cardiovascular Innovations and Applications2018年2期
- Cardiovascular Innovations and Applications的其它文章
- His Bundle Pacing: Rebirth of an lmportant Technique for Pacing the lntrinsic Conduction System
- Depression in Adults with Congenital Heart Disease: Prevalence, Prognosis,and lntervention
- Traditional Chinese Medicine ls Widely Used for Cardiovascular Disease
- The Fontan Circulation: Contemporary Review of Ongoing Challenges and Management Strategies
- D-Transposition of the Great Arteries: A New Era in Cardiology
- Atrial Arrhythmias lncluding Atrial Fibrillation in Congenital Heart Disease: Mechanisms,Substrate ldentification and lnterventional Approaches