
His Bundle Pacing: Rebirth of an lmportant Technique for Pacing the lntrinsic Conduction System
2018-07-04 06:43:12MichaelKaufmannMDMatthewMcKillopMDFHRSThomasBurkartMDFACCFHRSMarkPannaMDFACCFHRSWilliamMilesMDFACCFHRSandRichardContiMDMACCDepartmentofMedicineUniversityofFloridaGainesvilleFL3260USA
Michael R.Kaufmann, MD, Matthew S.McKillop, MD, FHRS, Thomas A.Burkart,MD, FACC, FHRS, Mark Panna, MD, FACC, FHRS, William M.Miles, MD, FACC, FHRS and C.Richard Conti, MD, MACCDepartment of Medicine, University of Florida, Gainesville, FL 3260, USA
lntroduction
The cardiac conduction system consists of cells specialized for conduction of electrical impulses.Cardiac electrical activity arises via automaticity of cells within the sinoatrial node, usually generating an action potential at a rate of 60–100 bpm.That action potential is then conducted through atrial myocardium to the AV node, through the bundle of His,and down the right and left bundle branches to activate the ventricular myocardium via arborization of Purkinje fi bers.Importantly, the bundle of His and bundle branches contain fi bers specialized for rapid conduction of electrical impulses.Ventricular activation via the bundle of His and bundle branches not only ensures rapid and synchronous ventricular activation, but also activates the myocardium in such a way that papillary muscle contraction precedes that of the ventricles, thereby preventing AV valve regurgitation.
Permanent pacemaker implantation is most commonly indicated for sinus node dysfunction and atrioventricular (AV) block [1].The percentage of dual-chamber (atrial-ventricular) permanent pacemaker implantation is increasing [1, 2].Most commonly, the ventricular lead in a dual-chamber pacemaker system is implanted via trans-venous access to an endocardial location at the right ventricular (RV) apex or RV septum.However, pacing the RV results in non-physiologic electrical activation of the ventricular myocardium and causes electrical and mechanical dyssynchrony, and strong evidence now exists showing deleterious effects of chronic RV pacing.Chronic RV pacing is associated with altered cardiac histology with myofiber size variation and fi brosis on endomyocardial biopsy [3].In addition, clinical outcome studies show that higher cumulative percentage of RV pacing increases the risk of atrial fi brillation, heart failure hospitalization, and mortality [4, 5].
Role of Cardiac Resynchronization Therapy
Cardiac resynchronization therapy (CRT) is currently the most common approach to reduce ventricular dyssynchrony in cardiac pacing.CRT involves placement of two ventricular leads, one at the RV apex or septum, and one on the left ventricular (LV) lateral wall.Most commonly the LV lead is implanted via a trans-venous approach utilizing specialized delivery sheaths to place the lead in a lateral branch of the coronary sinus (CS); however,surgical epicardial LV lead placement can also be performed.Both ventricles are then paced simultaneously in an effort to treat (or prevent) ventricular dyssynchrony.In patients with preserved LVEF,CRT with “biventricular pacing” has been shown to result in higher LVEF at follow-up evaluation compared to RV apical pacing alone [6].In addition, patients with NYHA class I, II or III congestive heart failure and LVEF ≤50% randomized to CRT were found to have a lower risk of a combined endpoint of heart failure exacerbation requiring IV therapy, increase in LV end-systolic volume index,or all cause-mortality compared with patients randomized to RV pacing alone [7].
Limitations of CRT with Biventricular Pacing
Cardiac resynchronization therapy with biventricular pacing has several limitations.First, not all patients have suitable anatomy for trans-coronarysinus LV lead placement, with overall failure rate for CS lead placement estimated at 3–4% [8].Inability to cannulate the CS, poor CS branch anatomy, myocardial scar resulting in elevated LV pacing thresholds, and phrenic nerve stimulation are all anatomic barriers that can prevent successful CRT device implant.Moreover, even in patients in whom an LV lead is successfully implanted, some patients will not respond favorably to CRT.Although agreement amongst criteria to define CRT response is poor [9],estimates of non-response has been reported from 16% [10] to 48% [11].Finally, there are likely many more patients presenting for pacemaker implant that would benef it from having RV and LV synchrony than currently recommended by published CRT guidelines [12, 13] or appropriate use criteria [14]documents.Published guidelines and appropriate use criteria documents are published infrequently,and are slow to adapt as new studies are published.Third party payers, too, are slow to expand payment coverage for expensive CRT devices.
Permanent His-Bundle Pacing
Permanent His-bundle pacing represents a unique alternative to RV apical or RV septal pacing, and in some instances to LV-lead cardiac resynchronization.The His-Purkinje system is a longitudinallyoriented collection of cells specialized for rapid conduction of electrical signals.The His bundle cells are insulated from the surrounding ventricular myocardium and are normally activated by the electrical output from the compact AV node.Thus,in patients without significant infra-His conduction delay or block, His-bundle pacing allows synchronous activation of the ventricles, avoiding the deleterious effects of traditional RV-pacing induced dyssynchrony.
His-Bundle Pacing: Early Days
While His-bundle pacing has re-emerged as an important technique in cardiac pacing, the concept is not new.Benjamin Sherlag and Anthony Damato fi rst reported catheter recording of a Hisbundle potential in humans in 1969 [15].While catheter studies of transient His-bundle pacing were reported in the interim [16], the fi rst report of Hisbundle pacing with a permanent pacing lead was not reported until 2000 [17].In this initial cohort permanent His-bundle pacing was successful in 12 of 18 assessed patients.
His-Bundle Pacing: A Re-Birth
More recently an observational, retrospective, case-control study compared 94 consecutive patients undergoing permanent pacemaker implant with attempt at His-bundle pacing at one hospital with 98 consecutive patients undergoing permanent pacemaker implant with conventional RV lead implantation at a separate hospital [18].In this study His-bundle pacing was successful in 80% of attempted cases and while procedure time was higher in the His-bundle pacing group, fl uoroscopy time was similar between the two groups.Stability and reliability of a permanent pacing lead in the His-bundle location appears adequate with ventricular lead revision required in only three patients in the His-bundle pacing group and ventricular lead revision necessary in two patients in the conventional RV pacing group.Importantly,His-bundle pacing was associated with fewer heart failure hospitalizations in patients with >40% ventricular pacing burden.
Personal Experience with His- Bundle Pacing: Procedure Technique
In our lab we use a technique for direct His bundle pacing that has been described previously by Sharma and colleagues [18].A fi xed curve sheath(C315 HIS, Medtronic, Inc.Minneapolis, MN,USA) is used to direct a bipolar fi xed helix screw pacing lead (model 3830, 69 cm, Medtronic, Inc.,)to a location on the AV septum.Left axillary or subclavian vein access is obtained via the Seldinger technique and a short 7 French peel-away sheath is inserted into the vein.The His can be targeted either by advancing the sheath and lead directly from the right atrium (RA), or by advancing the sheath and lead into the RV and withdrawing until a His bundle potential is mapped.A 150 cm j-tipped guidewire is advanced into the RA and the C315 HIS fi xed curve sheath is inserted through the short 7Fr sheath and into the RA over the j-tipped guidewire.The guidewire is then removed and the 3830 pacing lead is advanced through the C315HIS sheath until only the very tip of the lead protrudes from the end of the sheath.Unipolar mapping is then performed from the tip of the lead and the unipolar electrograms are displayed on both the pacing analyzer (gain setting of 0.05 mV/mm and sweep speed of 50 mm/s) and the electrophysiology lab recording system (displayed at a sweep speed of 100 mm/s).Once the tip of the lead is through the delivery sheath and in the RA, the sheath is advanced to a low RA/high RV septal location and the tip of the lead is manipulated(and the AV septum mapped) by advancing (and later withdrawing, if necessary) the sheath, as well as placing clockwise or counterclockwise torque on the sheath.With the RV approach oftentimes a right bundle branch potential can be seen initially and then a His potential seen as the sheath and lead are withdrawn further across the septal leaflet of the tricuspid valve.When a septal site with a His potential on the lead tip (Figure 1) is identified, the lead is secured into place by clockwise rotation of 4–6 turns on the lead.The sheath is then withdrawn slightly, adequate slack added to the lead system(Figure 2), and testing of sensing and pacing thresholds performed in both unipolar and bipolar sensing and pacing configurations.Once the lead is secured in a position with His bundle capture, adequate ventricular sensing measurements, and an acceptable pacing threshold, the C315HIS delivery sheath is slit away from the lead, the short 7Fr sheath peeled away from the lead, and the lead is secured to the pocket fl oor.The atrial lead (if indicated) is then placed, and the leads are connected to the pacemaker generator (Figure 3).
While we have successfully implanted permanent His bundle pacing leads with either the RA or RV septal approach, we have occasionally had difficulty with the lead tip getting caught on the septal leaflet of the tricuspid valve when withdrawing the sheath and lead from the RV.Additionally, care should be given to not let more than just the tip of the 3830 lead extend beyond the C315 HIS sheath, because further extension can risk the lead getting entrapped in the tricuspid valve chordae.
Our early experience with eight cases (Table 1)demonstrates that utilizing the above recently described techniques, successful permanent Hisbundle pacing can be achieved with a short learning curve in the majority of candidates.While Hisbundle pacing lead implant was initially successfulin seven of our eight attempted cases, long-term follow-up data are needed to assign long-term success.
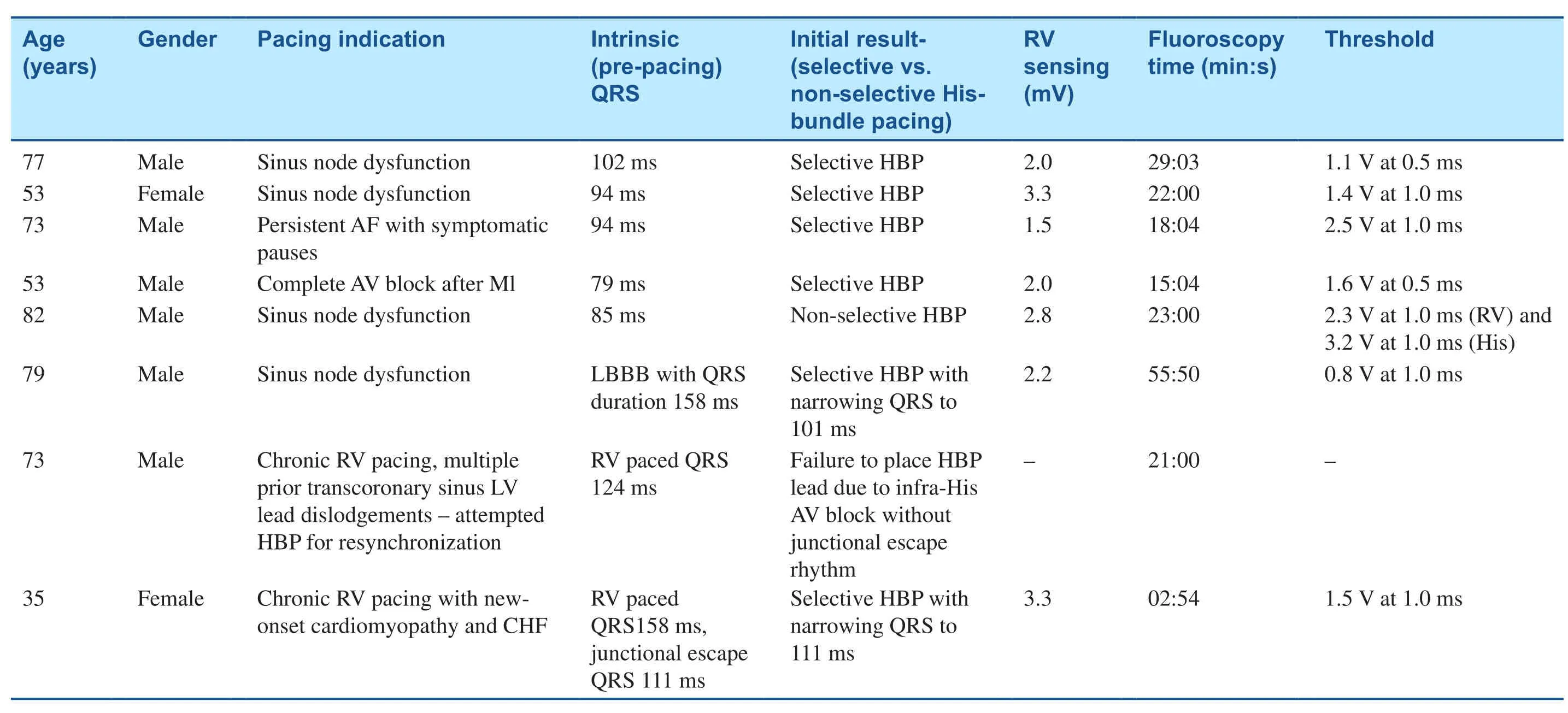
Table 1 HBP Outcomes.

Figure 1 Display of Surface ECG Leads and Unipolar Electrogram from Lead Tip (Bottom Tracing) Showing His Electrogram Potentials (Solid Black Arrows).
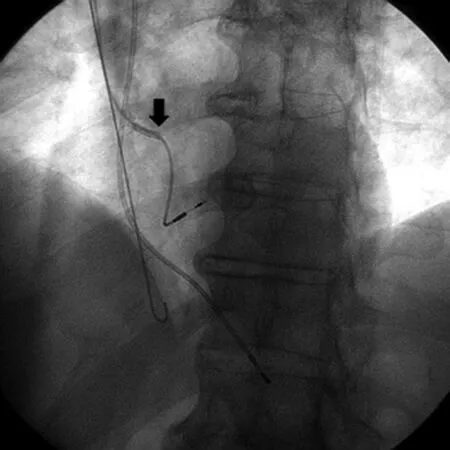
Figure 2 C315 His Delivery Sheath is Withdrawn and Slack Added to Lead to Test Unipolar and Bipolar Sensing and Pacing Thresholds.

Figure 3 Final LAO Cine of Dual-Chamber Permanent Pacemaker with Permanent His Bundle Pacing Lead and Right Atrial Appendage Lead.
Responses to His-Bundle Pacing
Two different responses to His bundle-pacing are possible, depending on the precise location of lead tip fi xation and pacing capture.When the tip of the lead is fi xed directly into His bundle fi bers, direct(selective) His-bundle pacing results (Figure 4).In direct His-bundle pacing lower pacing outputs capture only His-bundle fi bers resulting in a paced QRS with the same morphology as the native(non-paced) QRS, and a pacing stimulus to QRS interval equal to the HV interval in sinus rhythm.With direct (selective) His bundle pacing at higher energy outputs, both the His bundle fi bers and the“paraHis” ventricle are stimulated resulting in pre-excitation of the ventricle; this is characterized by a delta-wave appearance of the QRS complex,a QRS morphology that is slightly wider than the native (non-paced) QRS morphology, and a pacing stimulus to QRS interval shorter than the HV interval in sinus rhythm.
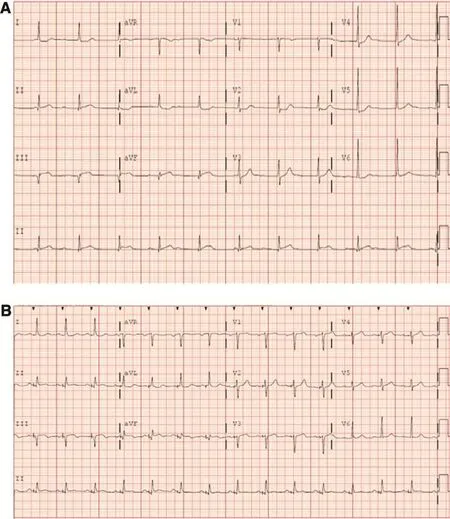
Figure 4 Direct (Selective) His-Bundle Pacing, All Images from Same Patient.
The second type of response seen with His bundle pacing is called indirect (non-selective) His bundle pacing and occurs when the tip of the lead is fi xed into the ventricular myocytes immediately adjacent to the His bundle (“para-His” ventricle) (Figure 5).With indirect (non-selective) His bundle pacing,pacing at lower pacing outputs results in only septal RV capture, whereas pacing at higher pacing outputs narrows the QRS duration as both the His bundle and the para-His ventricle are activated.Either direct or indirect His bundle pacing is considered acceptable.
Figure 4 (Continued)
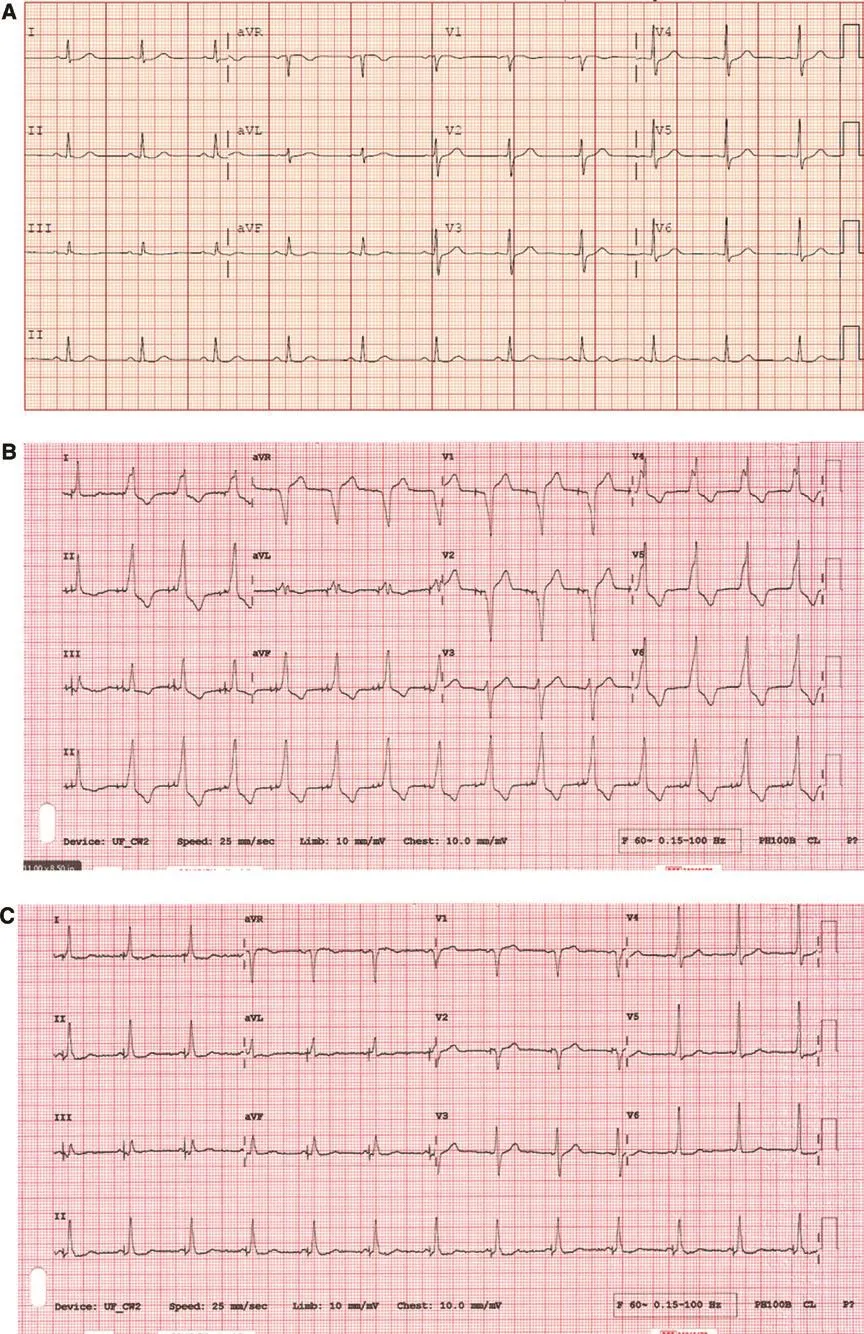
Figure 5 Indirect (Non-Selective) His-Bundle Pacing.
Advantages of His-Bundle Pacing
There are multiple advantages to placement of the ventricular lead at the His-bundle location instead of the conventional RV location.First, pacing the ventricle via the intrinsic conduction system preserves ventricular synchrony and can prevent the aforementioned deleterious effects of chronic RV pacing.Secondly, tricuspid valve dysfunction is a reported complication of trans-venous lead placement across the tricuspid valve [19].Autopsy analysis of direct (selective) His-bundle pacing lead placement has shown lead tip location on the atrial side of the tricuspid valve [20].As such,direct (selective) His-bundle pacing lead location may prevent lead-related tricuspid valve dysfunction associated with conventional RV apical or RV septal lead placement.
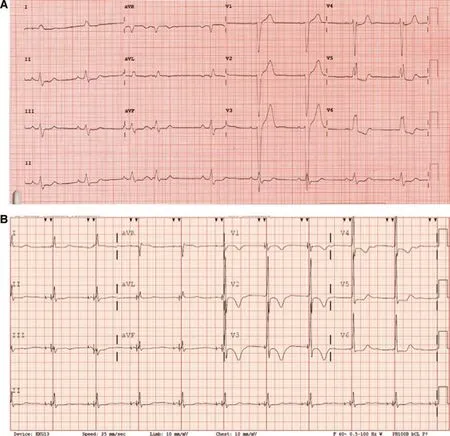
Figure 6 His-Bundle Pacing Narrows Lbbb.
Moreover, in some patients with bundle branch block His bundle pacing can actually narrow the QRS and restore ventricular synchrony [21] (Figure 6).In 1977 Narula fi rst described the phenomenon of “longitudinal dissociation in the His bundle”whereby bundle branch block was identified in some individuals as a discrete conduction slowing or block within the His bundle (and not block more distally in the bundle branches, which is what many conceptualize).He demonstrated that in 25 patients with LBBB pacing the distal His bundle (presumably distal to a focal lesion in the fi bers of the proximal His)abolished the left bundle branch block and narrowed the QRS [16].The potential to abolish bundle branch block and narrow the QRS with His-bundle pacing represents an alternative to conventional biventricular pacing in patients with bundle branch block who do not meet guideline criteria for CRT, in patients in whom attempted CS lead implant is unsuccessful, or in patients who do not respond to CRT.There is theoretical reason to believe that normal His-Purkinje conduction provides better synchrony than even the best biventricular pacing.
Limitations to Permanent His-Bundle Pacing
Limitations to permanent His bundle pacing exist.In the largest published study of His bundle pacing to date, implantation of a permanent His bundle pacing lead was unsuccessful in 20% of patients, and the lead instead had to be placed in a RV septal location[18].Challenges to successful His bundle pacing include variation in patient anatomy and limited equipment at present designed for His bundle lead placement.As His bundle pacing becomes more widely accepted, hopefully medical device companies will invest in developing new sheaths and leads that will increase success rates in difficult cases.
Summary
Emerging literature suggests that His bundle pacing can be reliably performed in a majority of patients,and in some instances may be superior to conventional RV pacing.While not appropriate for all patients,many patients in need of permanent pacing may benef it from maintaining synchronous activation of the ventricle via the rapidly conducting His-Purkinje system.Short-term follow-up is good, but long-term follow-up is necessary to assess the value of His-bundle pacing in preventing or treating ventricular dyssynchrony.Permanent His-bundle pacing should be considered in patients with indication for cardiac pacing,and procedure technique and outcomes should continue to improve as new tools become available to assist with the implant procedure.
Conflict of lnterest
The authors declare no conflict of interest.
REFERENCES
1.Mond HG, Proclemer A.The 11thworld survey of cardiac pacing and implantable cardioverter-def ibrillators: calendar year 2009 – A world society of arrhythmia’s project.Pacing Clin Electrophysiol 2011;34(8):1013–27.
2.Greenspon AJ, Patel JD, Lau E,Ochoa JA, Frisch DR, Ho RT, et al.Trends in permanent pacemaker implantation in the United States from 1993 to 2009.J Am Coll Cardiol 2012;60(16):1540–5.
3.Karpawich PP, Rabah R, Haas JE.Altered cardiac histology following apical right ventricular pacing in patients with congenital atrioventricular block.Pacing Clin Electrophysiol 1999;22:1372–7.
4.Sweeney MO, Hellkamp AS,Ellenbogen KA, Greenspon AJ,Freedman RA, Lee KL, et al.Adverse effect of ventricular pacing on heart failure and atrial fi brillation among patients with normal baseline QRS duration in a clinical trial of pacemaker therapy for sinus node dyfunction.Circulation 2003;107:2932–7.
5.Wilkoff BL, Cook JR, Epstein AE,Greene HL, Hallstrom AP, Hsia H, et al.Dual-chamber pacing or ventricular backup pacing in patients with an implantable def ibrillator: the dual chamber and VVI implantable defibrillator(DAVID) trial.J Am Med Assoc 2002;288(24):3115–23.
6.Yu CM, Chan JY, Zhang Q, Omar R, Yip GW, Hussin A, et al.Biventricular pacing in patients with bradycardia and normal ejection fraction.N Engl J Med 2009;361(22):2123–34.
7.Curtis AB, Worley SJ, Adamson PB, Chung ES, Niazi I, Sherfesee L, et al.Biventricular pacing for atrioventricular block and systolic dysfunction.N Engl J Med 2013;368(17):1585–93.
8.Gamble J, Herring N, Ginks M,Rajappan K, Bashir Y, Betts TR.Procedural success of left ventricular lead placement for cardiac resynchronization therapy: a metaanalysis.JACC Clin Electrophysiol 2016;2(1):70–7.
9.Daubert JC, Saxon L, Adamson PB,Auricchio A, Berger RD, Beshai JF, et al.2012 EHRA/HRS expert consensus statement on cardiac resynchronization therapy in heart failure: implant and follow-up recommendations and management.Heart Rhythm 2012;9(9):1524–76.
10.Linde C, Abraham WT, Gold MR,St John Sutton M, Ghio S, Daubert C, et al.Randomized trial of cardiac resychronization in mildly symptomatic heart failure patients and in asymptomatic patients with left ventricular dysfunction and previous heart failure symptoms.J Am Coll Cardiol 2008;52:1834–43.
11.Gorcsan J, Kanzaki H, Bazaz R, Dohi K, Schwartzman D.Usefulness of echocardiographic tissue synchronization imaging to predict acute response to cardiac resynchronization therapy.Am J Cardiol 2004;93:1178–81.
12.Epstein AE, DiMarco JP, Ellenbogen KA, Estes NA 3rd, Freedman RA,Gettes LS, et al.ACC/AHA/HRS 2008 guidelines for device-based therapy of cardiac rhythm abnormalities: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines.Circulation 2008;117:e350–408.
13.Epstein AE, Darbar D, DiMarco JP, Ellenbogen KA, Estes NAM,Freedman RA, et al.2012 ACCF/AHA/HRS focused update of the 2008 guidelines for device-based therapy of cardiac rhythm abnormalities: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines.Circulation 2012;126:1–17.
14.Russo AM, Stainback RF, Bailey SR, Epstein AE, Heidenreich PA,Jessup M, et al.ACCF/HRS/AHA/ASE/HFSA/SCAI/SCCT/SCMR 2013 appropriate use criteria for implantable cardioverter-defibrillators and cardiac resynchronization therapy.J Am Coll Cardiol 2013;61(12):1318–68.
15.Scherlag BJ, Lau SH, Helfant RH,Berkowitz WD, Stein E, Damato AN.Catheter technique for recording his bundle activity in man.Circulation 1969;39:13–8.
16.Narula OS.Longitudinal dissociation in the His bundle: bundle branch block due to asynchronous conduction within the His bundle in man.Circulation 1977;56:996–1006.
17.Deshmukh P, Casavant DA,Romanyshyn M, Anderon K.Permanent, direct his-bundle pacing: a novel approach to cardiac pacing in patients with normal His-Purkinje activation.Circulation 2000;101:869–77.
18.Sharma PS, Dandamudi G,Naperkowski A, Oren JW, Storm RH, Ellenbogen KA, et al.Permanent His-bundle pacing is feasible, safe, and superior to right ventricular pacing in routine clinical practice.Heart Rhythm 2015;12(2):305–12.
19.Chang JD, Manning WJ, Ebrille E, Zimetbaum PJ.Tricuspid valve dysfunction following pacemaker or cardioverter-defibrillator implantation.J Am Coll Cardiol 2017;69(18):2331–41.
20.Correa de Sa DD, Hardin NJ, Crespo EM, Nicholas KB, Lustgarten DL.Autopsy analysis of the implantation site of a permanent selective direct His bundle pacing lead.Circ Arrhythm Electrophysiol 2012;5:244–6.
21.Lustgarten DL, Crespo EM,Arkhipova-Jenkins I, Lobel R,Winget J, Koehler J, et al.Hisbundle pacing versus biventricular pacing in cardiac resynchronization therapy patients: a cross-over design comparison.Heart Rhythm 2015;12(7):1548–57.
 Cardiovascular Innovations and Applications2018年2期
Cardiovascular Innovations and Applications2018年2期
- Cardiovascular Innovations and Applications的其它文章
- Depression in Adults with Congenital Heart Disease: Prevalence, Prognosis,and lntervention
- Traditional Chinese Medicine ls Widely Used for Cardiovascular Disease
- The Fontan Circulation: Contemporary Review of Ongoing Challenges and Management Strategies
- D-Transposition of the Great Arteries: A New Era in Cardiology
- Heart Transplantation for Adult Congenital Heart Disease: Overview and Special Considerations
- Atrial Arrhythmias lncluding Atrial Fibrillation in Congenital Heart Disease: Mechanisms,Substrate ldentification and lnterventional Approaches