甲状腺乳头状癌18F-FDG PET/CT显像葡萄糖代谢与BRAF突变的相关性研究
2018-01-09 03:33:51王治国武晓丹张国旭
实用肿瘤学杂志 2017年6期
王治国 武晓丹 战 莹 张 彤 张国旭
·临床研究·
甲状腺乳头状癌18F-FDG PET/CT显像葡萄糖代谢与BRAF突变的相关性研究
王治国 武晓丹 战 莹 张 彤 张国旭
目的评估甲状腺乳头状癌(Papillary thyroid carcinoma,PTC)患者18F-FDG PET/CT的最大标准摄取值(SUVmax)与BRAF突变的相关性。方法回顾性分析我院在甲状腺切除术前接受18F-FDG PET/CT显像和活检的患者51例(平均年龄为49.3±12.9岁),病理诊断为PTC 48例,甲状腺滤泡状癌(Follicular thyroid carcinoma,FTC)3例。采用基因检测法检测BRAF V600E突变状态,半定量分析法测定甲状腺结节灶的SUVmax,分析患者临床资料包括性别、年龄、肿瘤大小和甲状腺球蛋白浓度与SUVmax之间的相关性;将患者分为BRAF V600E突变组和未突变组,分析比较两组间SUVmax值的差异。结果在PTC患者中,33例患者肿瘤发生BRAF V600E突变,15例患者肿瘤未发生突变,BRAF V600E突变组的SUVmax显著高于未突变组(5.5±3.9vs. 2.2±1.2,P=0.002);肿瘤直径≥1 cm的患者的SUVmax明显高于肿瘤<1 cm(P<0.05);甲状腺球蛋白浓度升高患者的SUVmax高于正常甲状腺球蛋白浓度的患者(P<0.05);FTC组中未观察到BRAF V600E突变。结论PTC患者携带BRAF V600E突变基因相对于未携带者具有更高的SUVmax值,不同肿瘤大小、血清甲状腺球蛋浓度的PTC患者SUVmax值存在统计学差异。
18F-FDG PET/CT;甲状腺乳头状癌;最大标准摄取值;BRAF突变
甲状腺乳头状癌(Papillary thyroid carcinoma,PTC)是一种生长缓慢,治愈率较高的头颈部最常见的肿瘤,占甲状腺恶性肿瘤的80%以上。高分化PTC通过手术切除肿瘤和碘治疗后预后良好[1]。患者年龄、性别、家族遗传史、肿瘤大小、病灶数量、肿瘤亚型、是否有血管侵袭和淋巴结转移与患者复发转移甚至死亡密切相关[2]。因此,风险分级和预后评估是患者进一步治疗的重要环节,也是研究人员需要关注的重点[3-4]。18F-FDG PET/CT显像是目前常用的影像学诊断工具,已被用于甲状腺复发转移的定位中,尤其是血清甲状腺球蛋白浓度升高和131I显像阴性的患者[5-6]。有研究显示,患者生存率与18F-FDG的摄取强度存在密切关系[7]。18F-FDG PET/CT可以反映不同类型癌症肿瘤的扩散性和侵袭性,原发性甲状腺癌PET阳性与肿瘤的大小、病理类型以及双侧高发等有关[8]。
目前,研究发现BRAF基因突变存在于黑色素瘤、结肠癌和甲状腺癌中[9-10]。BRAF V600E是PTC中常见的突变类型,有研究显示,BRAF V600E突变可作为PTC患者预后指标,携带突变基因的PTC患者预后较差[11];也有研究表明,18F-FDG高摄取的甲状腺癌患者预后较差[12]。最近有研究证明BRAF V600E突变与PTC患者18F-FDG摄取存在一定的联系,BRAF是甲状腺癌复发转移患者中突变频率较高的基因[13]。本研究通过回顾性分析术前进行18F-FDG PET/CT显像的甲状腺癌患者,旨在通过分析PTC患者18F-FDG摄取与肿瘤BRAF V600E突变之间的关系,以探讨糖代谢在甲状腺癌预后评估中的临床意义。
1 材料与方法
1.1 研究对象
回顾性分析我院2012年5月—2017年5月原发性甲状腺癌术前6~8个月行18F-FDG PET/CT显像的患者51例,男性28例,女性23例,平均年龄49.3±12.9岁。纳入标准:患者经病理确诊为原发性甲状腺癌,均进行了BRAF突变检测和术前血清甲状腺球蛋白的测定。所有患者均接受甲状腺全切术(n=35)或半切术(n=16)治疗。
1.2 PET/CT检查方法
PET/CT检查采用GE Discovery VCT PET/CT仪。PET由32环探测器组成,横断层中心和轴向分辨率分别为4.8 mm,4.0 mm,配置64排螺旋CT。显像剂18F-脱氧葡萄糖(18F-FDG)由GE Minitrace回旋加速器及自动合成系统制备,放化纯>98%。患者检查前空腹6h以上,血糖水平<11.1 mmol/L。静脉注入18F-FDG(180~370 MBq),静卧40 min后,行头颈部或全身PET/CT扫描,3 min/床位,头部采集2~3个床位,全身采集5~7个床位。
1.3 18F-FDG PET/CT图像处理与分析
所有患者PET数据经低剂量CT进行衰减校正,迭代法重建后进行横断面、冠状面及矢状面多幅图像显示。搜集患者所有影像学资料,图像由具有多年影像诊断经验的两名核医学医师采用双盲法阅片,诊断结果经两位或以上医师达成一致意见方可记录。采用半定量法勾画病灶ROI,利用固有软件计算最大标准摄取值(SUVmax),记录患者甲状腺结节每一个18F-FDG高摄取病灶,通过CT图像观察结节的部位、大小等特征。
1.4 BRAF V600E突变分析
病理结果由病理科医生做出分析,BRAF V600E突变采用基因突变试剂盒检测,搜集患者基因突变检测结果。
1.5 统计学方法
2 结果
2.1 病理结果
本研究包括51例患者,48例(94.1%)为PTC,3例(5.9%)为甲状腺滤泡状癌(Follicular thyroid carcinoma,FTC)。在PTC组33例患者存在BRAF V600E突变,15例未见BRAF突变;3例FTC患者均未发现BRAF V600E突变。
2.2 PET/CT显像SUVmax与临床特征比较
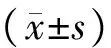
肿瘤直径大于1 cm的患者SUVmax(4.7±2.6)明显高于肿瘤直径小于1 cm患者(2.9±1.1)(P<0.05);血清甲状腺球蛋白浓度升高的患者SUVmax(5.8±2.4)明显高于正常浓度者(2.5±0.9)(P<0.05),男性PTC患者与女性PTC患者间SUVmax无统计学差异,年龄<45岁的PTC患者与≥45岁的PTC患者间SUVmax无统计学差异(P>0.05)(表1)。
2.3 BRAF突变与SUVmax的相关性研究
BRAF突变组患者SUVmax为5.5±3.9,BRAF未突变组患者SUVmax为2.2±1.2,差异具有统计学意义(P<0.05)(图1);典型病例如图2所示。
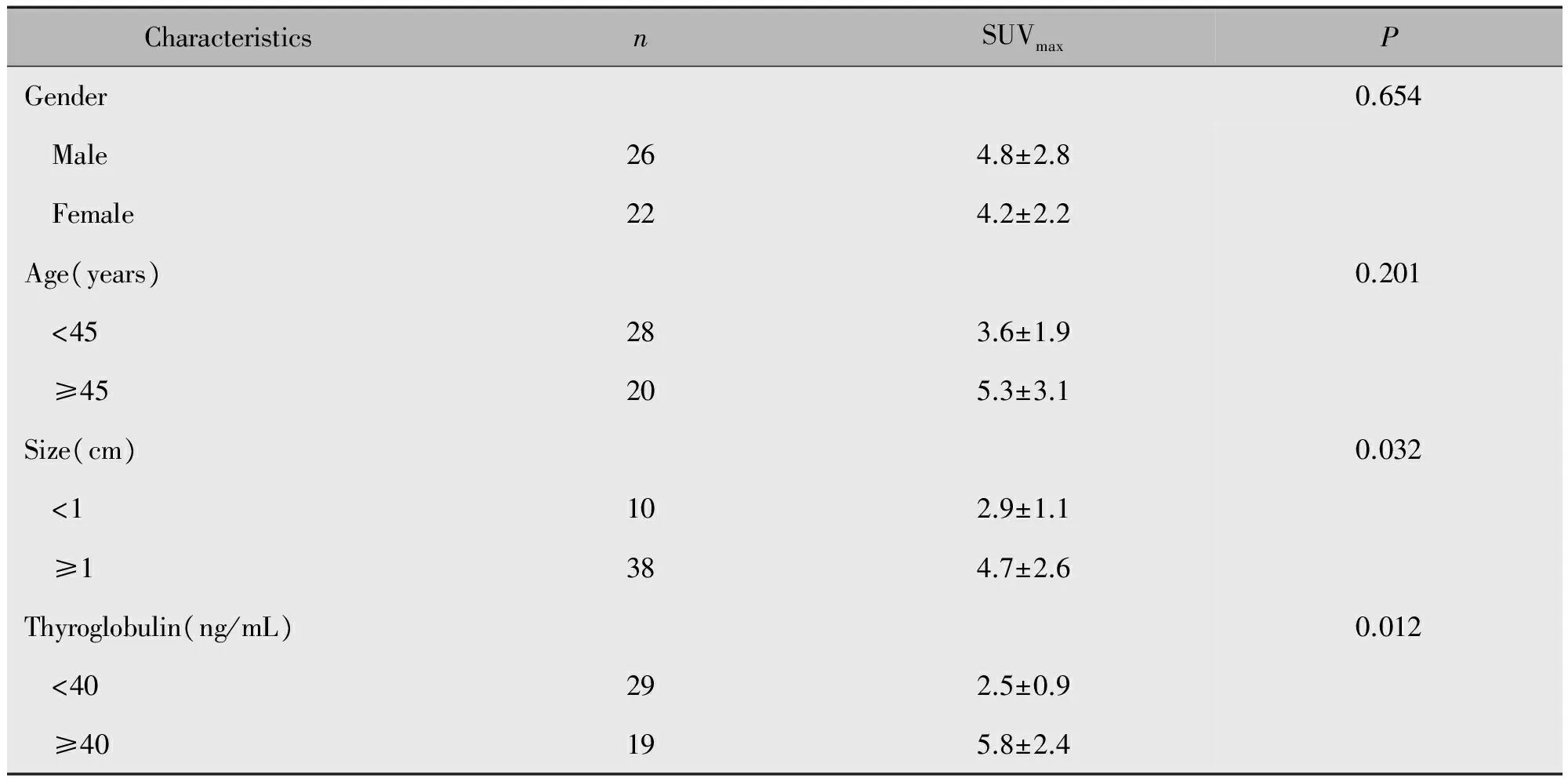
表1 PTC患者SUVmax与临床特征比较Table 1 Comparison of clinical characteristics and SUVmax in PTC patients

图1 BRAF V600E突变型与BRAF未突变型SUVmax比较Figure 1 Comparison of the SUVmax of BRAF V600E mutation with that of non-mutation
3 讨论
近年来,我国甲状腺癌的发病率有明显的增高趋势[14]。甲状腺癌属于内分泌领域最常见的恶性肿瘤,依据病理类型可分为PTC、FTC、甲状腺髓样癌(Medullary thyroid carcinoma)以及甲状腺未分化癌(Anaplastic thyroid carcinoma)。PTC是最常见的类型,对于甲状腺癌发病因素的研究已经成为甲状腺疾病研究领域的一个重要课题。本研究筛选的51例病例中,PTC患者48例(94.1%),FTC患者3例(5.9%)。甲状腺癌的发病机制尚无定论,目前认为潜在的诱发因素主要有家族性甲状腺疾病遗传史、基因突变、生活方式、饮食习惯、长期暴露于高辐射环境中以及其他肿瘤疾病等。PET/CT显像的原理是以肿瘤组织对葡萄糖的异常摄取为基础,将功能图像和解剖图像精确融合,能够在机体发生功能异常的早期,发现代谢的异常变化,在癌症复发和转移灶的探测定位和预后评估中具有广泛的应用,因此,PET/CT显像检查在甲状腺癌良恶性以及复发转移灶的早期探测中具有一定的应用价值。
葡萄糖是细胞生存代谢的必需物质,普遍认为,肿瘤细胞的高葡萄糖摄取率与其增殖有关,增殖细胞的快速转录和翻译消耗了大量腺苷三磷酸,使腺苷三磷酸与腺苷二磷酸的比例下降,通过影响代谢限速酶的结构增加葡萄糖的利用,但一些缓慢增殖的恶性肿瘤也表现出对葡萄糖的高摄取[15-16]。最近有研究人员提出肿瘤细胞高葡萄糖摄取不一定是快速增殖的结果,可能是由参与葡萄糖代谢的转运蛋白或酶引起致癌基因的激活导致的[17]。关于致癌基因与葡萄糖代谢的临床前研究较充分,但是临床资料相对较少。研究人员通过研究特异性致癌基因激活与葡萄糖代谢之间的关系了解致癌基因与葡萄糖代谢之间的关系。Parmenter和Palaskas等分别研究了黑色素瘤BRAF突变以及基底样乳腺癌活化丝裂原活化蛋白激酶(Mitogen-activated protein kinases,MAPKs)下游靶点与细胞葡萄糖摄取之间的关系,结果表明基因突变与葡萄糖的摄取密切相关[18-19]。
图2 携带与未携带BRAF V600E PTC患者18F-FDG PET/CT图像Figure 2 The 18F-FDG PET/CT images showed PTC patients with BRAF V600E and non-mutationNote:A.Patient,male,58 years old,no BRAF mutation,a round nodules in thyroid right lobe,1.5 cm in diameter on CT,SUVmax=2.6;B.Patients,female,65 years old,harboring BRAF V600E mutation,circular low density lesions in thyroid,2.0 cm in diameter on CT,SUVmax=14.3.
已有研究表明,PTC患者18F-FDG高摄取率与BRAF突变有关。这可能与BRAF V600E定位于线粒体导致PTC患者线粒体中O2消耗减少从而导致葡萄糖摄取增加以及携带BRAF V600E突变的PTC患者糖酵解的限速酶丙酮酸激酶亚型M2的表达增加有关[20-21]。也有研究显示,BRAF突变型PTC患者较未突变型的GLUT1和HIF-1α水平显著升高[22-23]。PTC患者携带BRAF V600E使肿瘤复发转移的风险增加2.14倍,这种突变与癌症死亡率显著相关[24-25];本研究量化了SUVmax与BRAF V600E突变之间的关系,携带BRAF V600E突变的PTC患者具有更高的葡萄糖摄取率,因此,18F-FDG摄取可辅助预测PTC患者突变基因BRAF V600E的存在。Kim等研究显示18F-FDG的摄取与肿瘤的大小相关[26],本研究也分析了SUVmax与患者临床资料,如性别、年龄、肿瘤直径以及术前血清甲状腺球蛋白之间的关系,得出PTC患者肿瘤直径大于1 cm比直径小于1 cm具有更高的18F-FDG摄取率,同时我们还得出术前血清甲状腺球蛋白升高与SUVmax高摄取显著相关。
本研究也存在一定局限性,第一,回顾性分析的患者数量相对较少,对于小于1 cm的小病灶,PET/CT的灵敏度和空间分辨率可能不是最佳的;第二,并非所有患者都接受18F-FDG PET/CT显像,一般是131I显像阴性患者或肿瘤恶性程度较大的患者行PET/CT显像,因此,患者选择可能出现偏倚;第三,患者在术前6~8个月行PET/CT显像,期间可能有些肿瘤的状态会发生改变,由此可能给研究结果带来一定的偏倚。
1 Tang KT,Lee CH.BRAF mutation in papillary thyroid carcinoma:pathogenic role and clinical implications[J].J Chin Med Assoc,2010,73(3):113-128.
2 Pak K,Kim SJ,Kim IJ,et al.The role of18F-fluorodeoxyglucose positron emission tomography in differentiated thyroid cancer before surgery[J].Endocr Relat Cancer,2013,20(4):203-213.
3 Sturgeon C,Angelos P.Identification and treatment of aggressive thyroid cancers.Part 2:risk assessment and treatment[J].Oncology,2006,20(3):397-404.
4 Randolph GW,Duh QY,Heller KS,et al.The prognostic significance of nodal metastases from papillary thyroid carcinoma can be stratified based on the size and number of metastatic lymph nodes,as well as the presence of extranodal extension[J].Thyroid,2012,22(11):1144-1152.
5 薛明媚,刘保平,谢新立,等.18F-FDG PET/CT检测Tg阳性而131I-诊断剂量全身显像阴性分化型甲状腺癌患者复发和转移[J].中国医学影像技术,2016,32(2):218-222.
6 Gao WL,Wei LL,Chao YG,et al.Prognostic prediction of BRAF(V600E)and its relationship with sodium iodide symporter in classic variant of papillary thyroid carcinomas[J].Clin Lab,2012,58(9):919-926.
7 Rosenbaum-Krumme SJ,Gorges R,Bockisch A,et al.18F-FDG PET/CT changes therapy management in high-risk DTC after first radioiodine therapy[J].Eur J Nucl Med Mol Imaging,2012,39(9):1373-1380.
8 Li YJ,Dai YL,Cheng YS,et al.Positron emission tomography(18)F-fluorodeoxyglucose uptake and prognosis in patients with bone and soft tissue sarcoma:A meta-analysis[J].Eur J Surg Oncol,2016,42(8):1103-1114.
9 Parmenter TJ,Kleinschmidt M,Kinross KM,et al.Response of BRAF-mutant melanoma to BRAF inhibition is mediated by a network of transcriptional regulators of glycolysis[J].Cancer Discov,2014,4(4):423-433.
10 Normanno N,Rachiglio AM,Lambiase M,et al.Heterogeneity of KRAS,NRAS,BRAF and PIK3CA mutations in metastatic colorectal cancer and potential effects on therapy in the CAPRI GOIM trial[J].Ann Oncol,2015,26(8):1710-1714.
11 Xing M,Alzahrani AS,Carson KA,et al.Association between BRAF V600E mutation and mortality in patients with papillary thyroid cancer[J].JAMA,2013,309(14):1493-1501.
12 Rosenbaum-Krumme SJ,Gǒrges R,Bockisch A,et al.18F-FDG PET/CT changes therapy management in high-risk DTC after first radioiodine therapy[J].Eur J Nucl Med Mol Imaging,2012,39(9):1373-1380.
13 Schulten HJ,Al-Maghrabi J,Al-Ghamdi K,et al.Mutational screening of RET,HRAS,KRAS,NRAS,BRAF,AKT1,and CTNNB1 in medullary thyroid carcinoma[J].Anticancer Res,2011,31(12):4179-4183.
14 Leenhardt L,Grosclaud P,Cherie-challine L,et al.Increased incidence of thyroid carcinoma in france:a true epidemic or thyroid nodule management effects? Report from the French thyroid cancer committee[J].Thyroid,2004,14(12):1056-1060.
15 Ward PS,Thompson CB.Metabolic reprogramming:a cancer hallmark even Warburg did not anticipate[J].Cancer Cell,2012,21(3):297-308.
16 Israel O,Yefremov N,Bar-Shalom R,et al.PET/CT detection of unexpected gastrointestinal foci of18F-FDG uptake:incidence,localization patterns,and clinical significance[J].Cancer Cell,2012,21(3):297-308.
17 Ward PS,Thompson CB.Metabolic reprogramming:a cancer hallmark even Warburg did not anticipate[J].Cancer Cell,2012,21(3):297-308.
18 Parmenter TJ,Kleinschmidt M,Kinross KM,et al.Response of BRAF-mutant melanoma to BRAF inhibition is mediated by a network of transcriptional regulators of glycolysis[J].Cancer Discov,2014,4(4):423-433.
19 Palaskas N,Larson SM,Schultz N,et al.18F-fluorodeoxy-glucose positron emission tomography marks MYC-overexpressing human basal-like breast cancers[J].Cancer Res,2011,71(5):5164-5174.
20 Lee MH,Lee SE,Kim DW,et al.Mitochondrial localization and regulation of BRAFV600E in thyroid cancer:a clinically used RAF inhibitor is unable to block the mitochondrial activities of BRAF V600E[J].J Clin Endocrinol Metab,2011,96(1):19-30.
21 Feng C,Gao Y,Wang C,et al.Aberrant overexpression of pyruvate kinase M2 is associated with aggressive tumor features and the BRAF mutation in papillary thyroid cancer[J].J Clin Endocrinol Metab,2013,98(9):1524-1533.
22 Grabellus F,Worm K,Schmid KW,et al.The BRAF V600E mutation in papillary thyroid carcinoma is associated with glucose transporter 1 over expression[J].Thyroid,2012,22(4):377-382.
23 Zerilli M,Zito G,Martorana A,et al.BRAF(V600E)mutation influences hypoxia-inducible factor-1alpha expression levels in papillary thyroid cancer[J].Mod Pathol,2010,23(8):1052-1060.
24 Kim TH,Park YJ,Lim JA,et al.The association of the BRAF(V600E)mutation with prognostic factors and poor clinical outcome in papillary thyroid cancer:a meta-analysis[J].Cancer,2012,118(7):1764-1773.
25 Liu C,Chen T,Liu Z.Associations between BRAF(V600E)and prognostic factors and poor outcomes in papillarythyroid carcinoma:a meta-analysis[J].Word J Surg Oncol,2016,14(1):241.
26 Kim MH,Ko SH,Bae JS,et al.Non FDG-avid primary papillary thyroid carcinoma may not differ from FDG-avid papillary thyroid carcinoma[J].Thyroid,2013,23(11):1452-1460.
ThecorrelationbetweenglucosemetabolismandBRAFmutationin18F-FDGPET/CTimagingofpapillarythyroidcarcinoma
WANGZhiguo,WUXiaodan,ZHANYing,ZHANGTong,ZHANGGuoxu
Department of Nuclear Medicine,The General Hospital of Shenyang Military Command,Shenyang 110016,China
ObjectiveThe objective of this study was to evaluate the correlation between maximum standard uptake values(SUVmax)of18F-FDG PET/CT and BRAF mutation in patients with papillary thyroid carcinoma(PTC).MethodsA total of 51 patients(mean age of 49.3±12.9 years)who underwent18F-FDG PET /CT imaging and biopsy before thyroidectomy were retrospectively analyzed.Based on the pathological results,there were 48 patients with PTC and 3 patients with follicular thyroid carcinoma(FTC).The SUVmaxof thyroid nodule was measured by semi-quantitative analysis.The correlation between clinical data(gender,age,tumor size and thyroglobulin concentration)and SUVmaxwas also analyzed.The difference of SUVmaxbetween the two groups was analyzed by comparing the BRAF V600E mutation group and the non-mutation group.ResultsIn patients with PTC,27 patients had BRAF V600E mutations and 11 patients had no tumor mutation.The SUVmaxof BRAF V600E mutation group was significantly higher than that in the non-mutated group(5.5±3.9vs. 2.2±1.2,P=0.002).The SUVmaxof patients with tumor diameter ≥ 1 cm was significantly higher than that in patients with tumor <1 cm(P<0.05).The SUVmaxof patients with elevated thyroglobulin concentration was higher than that in normal patients(P<0.05).No BRAF V600E mutation was observed in the FTC group.ConclusionThe BRAF V600E mutant gene has a high SUVmaxvalue in patients with PTC.There were significant difference in SUVmaxamong different tumor size and serum thyroglobulin concentration.
18F-FDG PET/CT;Thyroid papillary carcinoma;Maximal standard uptake value;BRAF mutation
沈阳军区总医院核医学科(沈阳 110016)
王治国,男,(1974-),硕士,副主任技师,从事PET/CT肿瘤显像的研究。
张国旭,E-mail:zhangguoxu502@sina.com
R736.1
A
10.11904/j.issn.1002-3070.2017.06.007
(收稿:2017-06-06)
猜你喜欢
疯狂英语·新读写(2021年10期)2021-12-07 02:41:30
国际放射医学核医学杂志(2021年10期)2021-02-28 08:43:46
国际放射医学核医学杂志(2021年10期)2021-02-28 08:43:24
中国甜菜糖业(2020年1期)2020-12-07 07:54:30
奥秘(2019年8期)2019-08-28 01:47:05
江苏卫生保健(2018年7期)2018-07-31 08:35:34
商周刊(2017年7期)2017-08-22 03:36:21
中国乳业(2016年4期)2016-11-07 09:50:27
小猕猴智力画刊(2016年6期)2016-05-14 09:21:40
中国卫生标准管理(2015年2期)2016-01-15 00:31:34