
慢性肾脏病与非瓣膜性心房颤动患者发生缺血性脑卒中的风险研究
2017-11-14 10:41牟红梅姚丹林
中外医学研究 2017年19期
牟红梅 姚丹林
【摘要】 目的:探讨慢性肾脏病(CKD)与非瓣膜性房颤患者发生缺血性脑卒中风险的关系。方法:选取359例非瓣膜性房颤患者,分为非瓣膜性房颤并脑卒中组127例及非瓣膜性房颤无脑卒中组232例;非瓣膜性房颤无脑卒中组按照CHA2DS2-VASc评分分为非瓣膜性房颤低中危组(CHA2DS2-VASc评分≤1分)124例和非瓣膜性房颤高危组(CHA2DS2-VASc评分≥2分)108例,比较各组eGFR及蛋白尿情况。结果:非瓣膜性房颤并脑卒中组eGFR较非瓣膜性房颤无脑卒中组显著降低;非瓣膜性房颤并脑卒中组蛋白尿阳性率较非瓣膜性房颤无脑卒中组显著升高,差异有统计学意义(P<0.05);Logistic回归分析显示eGFR、蛋白尿与非瓣膜性房颤患者缺血性脑卒中发病显著相关。结论:慢性肾脏病可能增加非瓣膜性房颤患者缺血性脑卒中的发病风险。
【关键词】 非瓣膜性心房颤动; 缺血性脑卒中; eGFR; 蛋白尿; 慢性肾脏病
doi:10.14033/j.cnki.cfmr.2017.19.036 文献标识码 B 文章编号 1674-6805(2017)19-0053-03
非瓣膜性房颤(non-valvular atrial fibrillation,NVAF)使患者的缺血性脑卒中发病率增加5~6倍,故临床上需要进行风险评估来识别可能发生缺血性脑卒中的高危患者。目前临床上采用CHA2DS2-VASc评分来评估非瓣膜性房颤患者发生缺血性脑卒中的风险,然而有部分低危患者仍发生了缺血性脑卒中,故需要进一步研究来发现新的风险因素用于评估非瓣膜性房颤患者缺血性脑卒中的风险。研究显示慢性肾脏病患者肾小球滤过率(eGFR)降低及蛋白尿是心血管疾病的独立危险因素,与非瓣膜性房颤的发病及其并发血栓栓塞事件相关[1]。为探讨中国人群慢性肾脏病与非瓣膜性房颤患者发生缺血性卒中风险的关系,笔者对359例非瓣膜性房颤患者进行了回顾分析。
1 资料与方法
1.1 一般资料
收集2005年1月-2016年12月于笔者所在医院心内科、神经内科住院的非瓣膜性房颤患者临床资料,共计359例,其中男183例,女176例;年龄(60.5±12.6)岁。入选标准:(1)年龄≥18 岁;(2)心电图或24 h动态心电图证实的持续或永久房颤;(3)超声心动图证实的非瓣膜性心脏病;(4)缺血性脑卒中诊断符合1995年第四届全国脑血管病会议制定的诊断标准。排除标准:冠心病、心脏瓣膜疾病、先天性心脏病、心肌病、炎症性疾病、甲状腺功能亢进性心脏病、肺源性心脏病、心脏手术患者和围产期患者。
1.2 方法
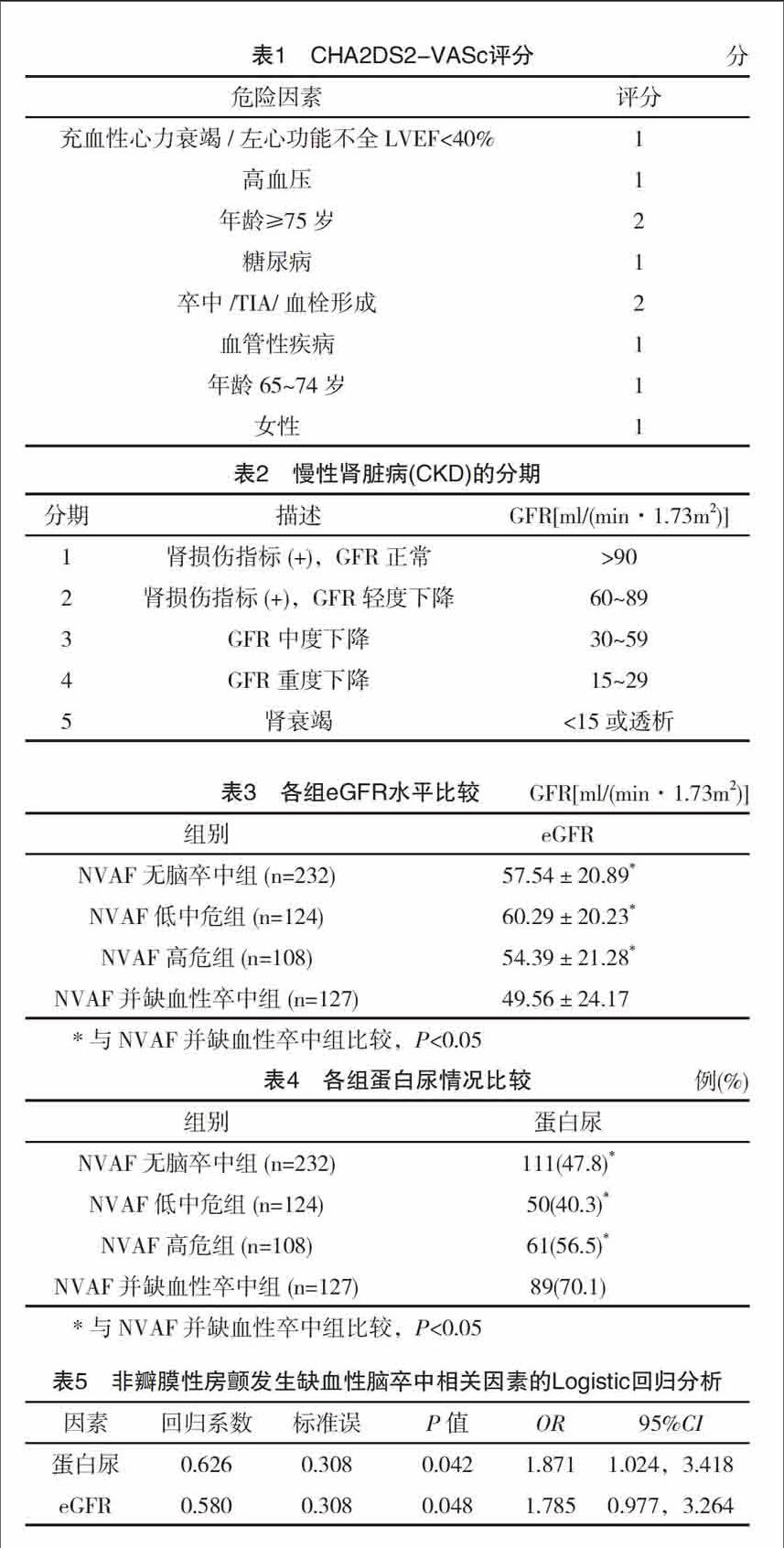
收集患者一般资料(姓名、性别、年龄、高血压、糖尿病、缺血性脑卒中史、血栓栓塞史、心功能级别、eGFR、蛋白尿、影像学辅助检查、颈动脉粥样斑块)。分组情况:根据有无合并缺血性卒中分为非瓣膜性房颤无脑卒中组232例和非瓣膜性房颤并缺血性卒中组127例;再根据CHA2DS2-VASc评分(表1):0分为低危,1分为中危,≥2为高危;将非瓣膜性房颤无脑卒中组分为非瓣膜性房颤低中危组124例(CHA2DS2-VASc评分≤1分)和非瓣膜性房颤高危组108例(CHA2DS2-VASc评分≥2分)。根据2006年我国预估肾小球滤过率协作组制定的适用于中国人的改良MDRD公式[2-3]:eGFR[(ml/min·1.73m2)]=175×血清肌酐(Scr)-1.234×年龄-0.179(女性×0.79)计算eGFR,eGFR与CKD的分期见表2。三次尿常规检测有两次尿蛋白≥1+并排除剧烈运动、重体力劳动、情绪激动、过冷、过热、应激状态、尿路感染和肾移植等情况后确诊为蛋白尿。比较各组间的eGFR水平和蛋白尿情况。
1.3 统计学方法
采用SPSS 22.0软件对所得数据进行统计分析,计量资料以(x±s)表示,采用t检验;计数资料以率(%)表示,采用字2检验,相关性分析采用二分类Logistic回归分析,P<0.05为差异有统计学意义。
2 结果
2.1 各组eGFR水平和蛋白尿情况
结果显示,非瓣膜性房颤并缺血性脑卒中组比非瓣膜性房颤无脑卒中组(及其亚分组:非瓣膜性房颤中低危组、高危组)的eGFR水平显著降低,蛋白尿发生率亦明显升高,差异均有统计学意义(P<0.05);非瓣膜性房颤低中危组血清eGFR水平明显高于非瓣膜性房颤高危组和非瓣膜性房颤合并缺血性脑卒中组,蛋白尿发生率亦明显降低,差异均有统计学意义(P<0.05),见表3、表4。2.2 危险因素相关性分析
以蛋白尿、eGFR为自变量,以非瓣膜性房颤患者发生缺血性脑卒中为因变量,进行二分类Logistic 回归分析,结果显示蛋白尿、eGFR是非瓣膜性房颤患者发生缺血性脑卒中的危险因素,差异均有统计学意义(P<0.05),见表5。
3 讨论
有研究对215例肾衰竭且无房颤或心血管病史的患者进行了研究,发现有33%的受试者在经食管超声心动图上发现了左心耳血栓[4]。慢性肾脏病患者缺血性卒中的发生率总体较高[5],在接受血液透析的患者中,房颤是常见的并发症之一[6-7],但是慢性肾脏病是否增加中国人群非瓣膜性房颤发生缺血性脑卒中的风险研究尚少。非瓣膜性房颤患者随着心房血流量的减少和由此产生的血供减少和血滞,容易形成左心耳血栓[8]。同時也可能通过各种代谢途径导致血液的高凝状态,虽然这些血栓形成的特异性因素并不明确[9-14],总的来说,各种影响因素会使心房血栓形成从而导致缺血性脑卒中。为什么慢性肾脏病会增加非瓣膜性房颤发生缺血性脑卒中的风险?
慢性肾脏病患者,各种内皮相关因子水平升高,比如血管内皮细胞纤溶酶原激活物抑制剂-1、血管性血友病因子(von Willebrand Factor,vWF)、各种凝血因子水平变化和活性的异常(如纤维蛋白原、纤维蛋白肽A、凝血酶原和凝血因子Ⅶ,Ⅷ、Ⅸ、Ⅻ等)及炎症介质的异常(如C反应蛋白和白细胞介素-6),而且慢性肾脏病与大动脉钙化和动脉粥样硬化的发生有关,从而导致血栓事件发生率增加[15-25]。轻中度慢性肾脏病患者促凝血功能和炎症通路的异常也是独立于其他因素的发生血栓危险因素之一[26]。endprint
非瓣膜性房顫患者发生的血栓主要是由纤维蛋白构成的静脉血栓而不是典型的动脉血栓。19073中老年受试者平均随访11.8年,在调整年龄、性别、种族、糖尿病、高血压等因素后,eGFR的下降与静脉血栓栓塞的风险增加显著相关[校正后OR为1.71;95%CI为(1.18,2.49)],这提示eGFR的下降可能与非瓣膜性房颤患者血栓事件有关[27]。有研究显示,尿蛋白排泄量与静脉血栓栓塞的风险增加显著相关[OR值为5.2;95%CI为(1.1,23)][28]。因此,慢性肾脏病通过各种上述途径增加非瓣膜性房颤患者发生缺血性卒中和其他血栓栓塞的风险。
2009年Lip等[29]提出了CHA2DS2-VASc评分法,但部分CHA2DS2-VASc评分为低中危患者仍发生了缺血性脑卒中[30],所以需要进行其它的危险因素研究,从而降低非瓣膜性房颤患者发生缺血性脑卒中的风险,而慢性肾脏病可能就是危险因素之一。
本研究发现非瓣膜性房颤并缺血性脑卒中组eGFR较非瓣膜性房颤无脑卒中组尤其是非瓣膜性房颤低中危组明显降低,蛋白尿发生率明显升高,结合Logistic 回归分析结果表明,在已知风险校正后eGFR水平降低和蛋白尿仍是非瓣膜性房颤并缺血性脑卒中发病的独立危险因素,这与2009年Go等[1]发表的文章研究结果(非瓣膜性房颤合并蛋白尿及eGFR下降患者血栓栓塞率较高,是缺血性脑卒中发病独立危险因素)一致。因此慢性肾脏病可能与非瓣膜性房颤患者发生缺血性脑卒中相关,故非瓣膜性房颤且CHA2DS2-VASs评分为低中危患者应评估其eGFR和蛋白尿情况,从而更好的预防非瓣膜性房颤患者发生缺血性脑卒中,改善预后。
参考文献
[1] Go A S,Fang M C,Udaltsova N,et al.Impact of proteinuria and glomerular filtration rate on risk of thromboembolism in atrial fibrillation:the anticoagulation and risk factors in atrial fibrillation(ATRIA)study[J].Circulation,2009,119(10):1363-1369.
[2] Xu Q,Li X,Gao B,et al.Comparative performance of four equations estimating glomerular filtration rate in adult Chinese diabetics[J].J Endocrinol Invest,2013,36(5):293-297.
[3] Ma Y C,Zuo L,Chen J H,et al.Modified glomerular filtration rate estimating equation for Chinese patients with chronic kidney disease[J].J Am Soc Nephrol,2006,17(10):2937-2944.
[4] Nishimura M,Hashimoto T,Kobayashi H,et al.The high incidence of left atrial appendage thrombosis in patients on maintenance haemodialysis[J].Nephrol Dial Transplant,2003,18(11):2339-2347.
[5] Seliger S L,Gillen D L,Longstreth W J,et al.Elevated risk of stroke among patients with end-stage renal disease[J].Kidney Int,2003,64(2):603-609.
[6] Vazquez E,Sanchez-Perales C,Borrego F,et al.Influence of atrial fibrillation on the morbido-mortality of patients on hemodialysis[J].Am Heart J,2000,140(6):886-890.
[7] Abbott K C,Trespalacios F C,Taylor A J,et al.Atrial fibrillation in chronic dialysis patients in the United States:risk factors for hospitalization and mortality[J].BMC Nephrol,2003,4(1):1.
[8] Bogousslavsky J,Cachin C,Regli F,et al.Cardiac sources of embolism and cerebral infarction-clinical consequences and vascular concomitants:the Lausanne Stroke Registry[J].Neurology,1991,41(6):855-859.
[9] Wang T D,Chen W J,Su S S,et al.Increased levels of tissue plasminogen activator antigen and factor VIII activity in nonvalvular atrial fibrillation:relation to predictors of thromboembolism[J].J Cardiovasc Electrophysiol,2001,12(8):877-884.endprint
[10] Chung N A,Belgore F,Li-Saw-Hee F L,et al.Is the hypercoagulable state in atrial fibrillation mediated by vascular endothelial growth factor?[J].Stroke,2002,33(9):2187-2191.
[11] Conway D S,Heeringa J,Van Der Kuip D A,et al.Atrial fibrillation and the prothrombotic state in the elderly:the Rotterdam Study[J].Stroke,2003,34(2):413-417.
[12] Feng D,D'Agostino R B,Silbershatz H,et al.Hemostatic state and atrial fibrillation (the Framingham Offspring Study)[J].Am J Cardiol,2001,87(2):168-171.
[13] Kahn S R,Solymoss S,Flegel K M.Nonvalvular atrial fibrillation: evidence for a prothrombotic state[J].CMAJ,1997,157(6):673-681.
[14] Marin F,Roldan V,Climent V,et al.Is thrombogenesis in atrial fibrillation related to matrix metalloproteinase-1 and its inhibitor, TIMP-1?[J].Stroke,2003,34(5):1181-1186.
[15] Segarra A,Chacon P,Martinez-Eyarre C,et al.Circulating levels of plasminogen activator inhibitor type-1, tissue plasminogen activator,and thrombomodulin in hemodialysis patients: biochemical correlations and role as independent predictors of coronary artery stenosis[J].J Am Soc Nephrol,2001,12(6):1255-1263.
[16] Hong S Y,Yang D H.Insulin levels and fibrinolytic activity in patients with end-stage renal disease[J].Nephron,1994,68(3):329-333.
[17] Tomura S,Nakamura Y,Doi M,et al.Fibrinogen, coagulation factor VII, tissue plasminogen activator,plasminogen activator inhibitor-1,and lipid as cardiovascular risk factors in chronic hemodialysis and continuous ambulatory peritoneal dialysis patients[J].Am J Kidney Dis,1996,27(6):848-854.
[18] Warrell R J,Hultin M B,Coller B S.Increased factor Ⅷ/von Willebrand factor antigen and von Willebrand factor activity in renal failure[J].Am J Med,1979,66(2):226-228.
[19] Tomura S,Nakamura Y,Deguchi F,et al.Plasma von Willebrand factor and thrombomodulin as markers of vascular disorders in patients undergoing regular hemodialysis therapy[J].Thromb Res,1990,58(4):413-419.
[20] Casserly L F,Dember L M.Thrombosis in end-stage renal disease[J].Semin Dial,2003,16(3):245-256.
[21] Owen W F,Lowrie E G.C-reactive protein as an outcome predictor for maintenance hemodialysis patients[J].Kidney Int,1998,54(2):627-636.
[22] Kaysen G A,Eiserich J P.Characteristics and effects of inflammation in end-stage renal disease[J].Semin Dial,2003,16(6):438-446.
[23] London G M,Guerin A P,Marchais S J,et al.Arterial media calcification in end-stage renal disease: impact on all-cause and cardiovascular mortality[J].Nephrol Dial Transplant,2003,18(9):1731-1740.endprint
[24] Raggi P,Boulay A,Chasan-Taber S,et al.Cardiac calcification in adult hemodialysis patients. A link between end-stage renal disease and cardiovascular disease?[J].J Am Coll Cardiol,2002,39(4):695-701.
[25] Groothoff J W,Gruppen M P,Offringa M,et al.Increased arterial stiffness in young adults with end-stage renal disease since childhood[J].J Am Soc Nephrol,2002,13(12):2953-2961.
[26] Shlipak M G,Fried L F,Crump C,et al.Elevations of inflammatory and procoagulant biomarkers in elderly persons with renal insufficiency[J].Circulation,2003,107(1):87-92.
[27] Wattanakit K,Cushman M,Stehman-Breen C,et al.Chronic kidney disease increases risk for venous thromboembolism[J].J Am Soc Nephrol,2008,19(1):135-140.
[28] Mahmoodi B K,Ten K M,Waanders F,et al.High absolute risks and predictors of venous and arterial thromboembolic events in patients with nephrotic syndrome:results from a large retrospective cohort study[J].Circulation,2008,117(2):224-230.
[29] Lip G Y,Nieuwlaat R,Pisters R,et al.Refining clinical risk stratification for predicting stroke and thromboembolism in atrial fibrillation using a novel risk factor-based approach:the euro heart survey on atrial fibrillation[J].Chest,2010,137(2):263-272.
[30] Glantzounis G K,Tsimoyiannis E C,Kappas A M,et al.Uric acid and oxidative stress[J].Curr Pharm Des,2005,11(32):4145-4151.
(收稿日期:2017-03-07)endprint
猜你喜欢
老友(2021年3期)2021-03-28
家庭百事通·健康一点通(2020年11期)2020-11-30
家庭用药(2018年12期)2018-02-14
中国民族民间医药·下半月(2016年12期)2017-01-19
心脑血管病防治(2016年6期)2017-01-16
中国当代医药(2016年30期)2017-01-07
中国实用医药(2016年23期)2016-12-26
中国实用医药(2016年28期)2016-12-07
中国实用医药(2016年16期)2016-07-26
中国实用医药(2016年13期)2016-07-05
