胸腔镜联合化疗与单纯化疗对晚期非小细胞肺癌患者预后的影响
2017-06-29 11:00韩文健肖龙敏
实用癌症杂志 2017年7期
韩文健 肖龙敏 吴 洪
胸腔镜联合化疗与单纯化疗对晚期非小细胞肺癌患者预后的影响
韩文健 肖龙敏 吴 洪
目的 评价胸腔镜联合化疗与单纯化疗对晚期非小细胞肺癌患者治疗后肺功能、生存率和生活质量的影响。方法 选取晚期非小细胞肺癌患者125例,依据随机原则并结合患者选择意愿将患者分为2组:胸腔镜联合化疗组(n=65),单纯化疗组(n=60)。计算随访时患者生存时间或患者死亡时间,并计算3年随访期间的死亡率。患者整个治疗结束后4周行肺功能检测。随访患者KPS评分,取其生存期限内的KPS评分的平均值。结果 随访患者治疗后的中位生存期和生存率,胸腔镜联合化疗组患者优于单纯化疗组的患者,差异有统计学意义(P<0.05)。胸腔镜联合化疗组的肺功能指标均优于单纯化疗组的患者,差异有统计学意义(P<0.05)。患者治疗后KPS评分在55~85分之间,胸腔镜联合化疗组患者优于单纯化疗组的患者,差异有统计学意义(P<0.05)。结论 非小细胞肺癌患者行胸腔镜联合化疗后,其肺功能、生存率和生活质量优于单纯化疗后的患者。
胸腔镜手术;化疗;非小细胞肺癌;肺功能;生存率;生活质量
(ThePracticalJournalofCancer,2017,32:1152~1155)
非小细胞肺癌(non-small cell lung cancer,NSCLC) 是人类发病率最高的恶性肿瘤之一,占肺癌患者的85%,已成为我国城市人口因恶性肿瘤致死的首要病因[1-3]。NSCLC患者5年生存率较低,晚期患者仅为10%左右[4]。微创外科(minimally invasive surgery,MIS)是现代外科发展的趋势,电视胸腔镜联合化疗(video-assisted thoracoscopic surgery,VATS)已成为近年来微创胸外科的热点[5]。因为胸腔镜能够减少肺叶切除术中的出血量,而且可以缓解胸痛,缩短胸管引流的时间和患者住院时间,故而引起业界的浓厚兴趣[6-8]。但是,胸腔镜联合化疗后,患者的肿瘤复发和生存率等诸问题缺乏大样本的临床调研,所以胸腔镜的临床推广使用受到影响。本文分析老年(≥65岁)Ⅲ期NSCLC患者的临床病例资料,探讨胸腔镜联合化疗与单纯化疗对晚期非小细胞肺癌患者的肺功能、生存率和生活质量的影响。
1 资料与方法
1.1 临床资料
患者入组标准:预期寿命3个月以上者Ⅲ期非小细胞肺癌老年患者,生活质量评分≥70 分,全部患者均自愿参加治疗,并签署知情同意书,治疗前各主要脏器功能正常,无手术禁忌证。
选取2006年1月至2011年1月本院收治的非小细胞肺癌患者125例,其中男性88例,女性37例;年龄65~83岁,中位年龄72岁;其中鳞状细胞癌79例,腺癌30例,腺鳞癌9例,大细胞肺癌7例;按照AJCC第7版非小细胞肺癌TNM分期患者均为Ⅲ期非小细胞肺癌;中央型肺癌67例,周围型肺癌58例;并发慢性阻塞性肺病患者46例。依据随机原则并结合患者选择意愿将患者分为2组:胸腔镜联合化疗组(n=65),单纯化疗组(n=60)。胸腔镜联合化疗组(n=65)平均年龄(70.33±9.42)岁,性别比例 (男性/女性)为8/8;单纯化疗组(n=65)平均年龄(72.25±9.83)岁,性别比例 (男性/女性)为8/8。2组受试者的年龄和性别比例无明显差异(P>0.05)。此外,受试者都完成试验,没有退出者,也无改用其他疗法者。
1.2 治疗方法
胸腔镜联合化疗组的受试患者首先实施胸腔镜下肿瘤切除术:①选择双腔导管实施插管,控制呼吸,全身静脉麻醉;②第6肋间的腋中线,置入套管联接胸腔镜摄像系统;③第7肋间的腋后线开放操作孔;④在胸腔镜下实施肺癌切除;⑤在胸腔镜下清扫纵膈淋巴结;⑥第4肋间开5~7 cm口,放入残端闭合器,取出标本;⑦游离肺血管与支气管,使用闭合器钉合患者的肺血管与支气管;⑧清扫肺门淋巴结和纵隔淋巴结。手术后2周实施化疗,化疗采纳EP方案,即依托泊苷80 mg/m2,第1~5天静脉点滴,顺铂30 mg/m2,第1~3天静脉点滴。4周为1个周期,共计实施治疗3个周期。单纯化疗组的化疗方案与胸腔镜联合化疗组的化疗方案相同。
1.3 疗效评价
化疗结束后4周时进行基线评估,每2至3个月随访1次。
①计算随访时患者生存时间(从确诊之日起算)或患者死亡时间,并计算3年随访期间的死亡率。
②患者治疗结束后4周行肺功能检测:用力肺活量占预计值的百分比(FVC%)、第1秒用力呼气容积占预计值的百分比(FEV1%)、1秒率(FEV1/FVC%)、最大分钟通气量占预计值的百分比(MVV%)、肺弥散功能占预计值的百分比(DLCO%)、肺总量占预计值的百分比 (TLC%)、最大摄氧量占预计值的百分比(VO2max%)、最大公斤摄氧量占预计值的百分比(VO2max/kg%)、最大运动功率占预计值的百分比(WRmax%)、最大氧脉占预计值的百分比(VO2/HRmax%)。
③患者治疗后Karnofsky评分法(KPS评分)的比较。Karnofsky功能状态评分标准体力状况评分标准是由美国东部肿瘤协作组提出,并依据患者能否正常活动、病情、生活自理程度把患者的健康状况分为100分,得分越高越能忍受治疗的副作用,因而也就有可能接受彻底的治疗。70分的患者生活可自理,但不能维持正常工作。
1.4 统计学方法
选择SPSS 20.0软件行统计学分析,计量资料用均数±标准差来表示,选择t检验进行分析;计数资料用%表示,使用χ2检验进行分析。P<0.05为差异有统计学意义。
2 结果
2.1 患者的中位生存期和生存率的比较
随访时间从治疗完毕开始计算,随访患者生存时间(从确诊之日起算)或患者死亡时间。胸腔镜联合化疗组:患者中位生存期22个月,死亡患者54例,其中31例死于胸部肿瘤局部进展,20例死于肿瘤远处转移,3例死于脑卒中。1年生存率89.2 %,3年生存率21.5%,5年生存率16.9%。
单纯化疗组:患者中位生存期20个月,死亡患者52例,其中28例死于胸部肿瘤局部复发,22例死于肿瘤发生远处转移,2例死于脑卒中。1年生存率45.0%,3年生存率18.3%,5年生存率13.3%。两者生存情况对比,差异有统计学意义,见表1。
2.2 患者的肺功能检查结果
胸腔镜联合化疗组的肺功能指标(VO2max/kg、VO2max、WRmax、VO2/HR和FEV1%、FVC%、MVV%、DLCO%、TLC%)均优于单纯化疗组的患者,2组差异有统计学意义,见表2。
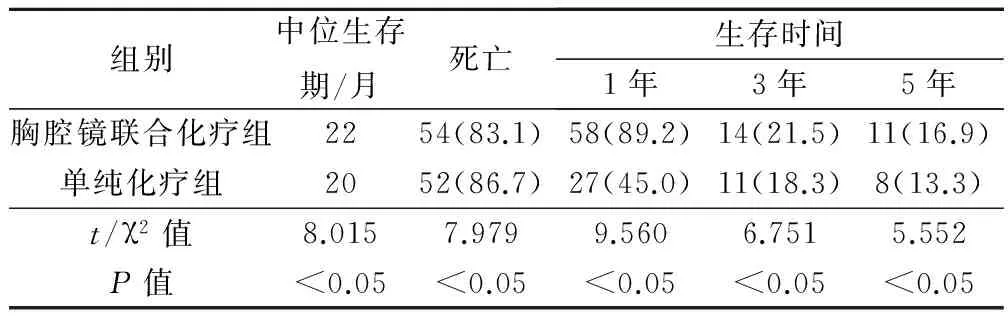
表1 患者的中位生存期和生存率的比较(例,%)

表2 2组患者术后运动心肺功能指标
2.3 患者治疗后KPS评分
随访发现,患者治疗后KPS评分在55~85分之间,胸腔镜联合化疗组KPS评分为(76.38±24.43)分,优于单纯化疗组的(64.12±16.74)分,两者差异有统计学意义(t=11.63,P<0.05)。
3 讨论
NSCLC发病率高,占肺癌患者的85%,常规标准治疗方法主要依靠手术切除,患者生存率较其他恶性肿瘤较低[9-11]。NSCLC大概占肺癌的将近80%,是最常见肺癌类型。NSCLC的恶性程度比较低,发展比较缓慢,但NSCLC的微转移灶是决定治疗的成败。正因为NSCLC的原发灶的生长比较缓慢,故而肺内原发病灶比较小的时候,其已经循淋巴道或者血道发生了远处转移,所以对NSCLC早期手术并彻底清扫相关淋巴结尤为重要[12-14]。
本研究发现,采用不同治疗措施后患者的生存时间存在差异,胸腔镜联合化疗组优于单纯化疗组。胸腔镜联合化疗组:患者中位生存期22个月,死亡患者54例,其中31例死于胸部肿瘤局部进展,20例死于肿瘤远处转移,3例死于脑卒中;1年生存率 89.2 %,3年生存率21.5%,5年生存率16.9%。单纯化疗组:患者中位生存期20个月,死亡患者52例,其中28例死于胸部肿瘤局部复发,22例死于肿瘤发生远处转移,2例死于脑卒中;1年生存率45.0%,3年生存率18.3%,5年生存率13.3%。本研究还发现,胸腔镜联合化疗组的肺功能指标(VO2max/kg、VO2max、WRmax、VO2/HR和FEV1% 、FVC%、MVV%、DLCO%、TLC%)均优于单纯化疗组的患者,两者差异有统计学意义。
使用胸腔镜实施早期NSCLC根治和淋巴结清扫术创伤小,出血少,对患者的心肺功能干扰比较小,手术后的并发症亦少,利于患者康复[15-17]。但是,胸腔镜联合化疗的适应证非常局限,其不能实施过于复杂的术式,目前限于肺癌的早期手术治疗和淋巴结清扫。而且,术中若出现大量或者快速出血,胸腔镜则缺少有效止血方法,所以术中应预备开胸包,随时做好中转开胸的准备工作[18]。
研究者认为,对于早期发现的NSCLC患者选择胸腔镜实施原发灶切除和淋巴结清扫术,这是因为利用胸腔镜实施手术清除纵隔附近的淋巴结能得到非常好的治疗效果。单纯化疗容易摧毁NSCLC患者的免疫系统,容易诱发肿瘤发生转移和复发,使得患者的生存时间缩短、生存率降低。
综上所述,非小细胞肺癌患者行胸腔镜联合化疗后,其肺功能、生存率和生活质量优于单纯化疗患者,建议在临床推广使用。
[1] Liao Y,Gu J,Wu Y,et al.Low level of 5-Hydroxymethylcytosine predicts poor prognosis in non-small cell lung cancer〔J〕.Oncol Lett,2016,11(6):3753-3760.
[2] Lu Y,Zhou X,Xu,et al.Long noncoding RNA ANRIL cou- ld be transactivated by c-Myc and promote tumor progression of non-small-cell lung cancer〔J〕.Onco Targets Ther,2016,9(5):3077-3084.
[3] Mori A,Hirose T,Tamura A,et al.Evaluation of the efficacy and safety of platinum doublet re-challenge chemotherapy in patients with recurrent advanced non-small cell lung cancer〔J〕.Gan To Kagaku Ryoho,2016,43(6):723-726.
[4] Wang L,Chen Z,An L,et al.Analysis of long non-coding RNA expression profiles in non-small cell lung cancer〔J〕.Cell Physiol Biochem,2016,38(6):2389-2400.
[5] Tacconi F,Pompeo E,Forceua D,et al.Non-intubated video-assisted thoracic surgery:where does evidence stand?〔J〕.J Thorac Dis,2016,8(Suppl 4):S364-375.
[6] Abe T,Kawai R,Uemura N,et al.Chylous leakage from a remaining duplicated left-sided thoracic duct after esophagectomy successfully treated by ligation of the left-sided thoracic duct with left-sided video-assisted thoracoscopic surgery with the patient in the prone position〔J〕.Asian J Endosc Surg,2016,9(2):138-141.
[7] Li S,Liu J,He J,et al.Video-assisted transthoracic surgery resection of a tracheal mass and reconstruction of trachea under non-intubated anesthesia with spontaneous breathing〔J〕.J Thorac Dis,2016,8(3):575-585.
[8] Song N,Zhao DP,Jiang L,et al.Subxiphoid uniportal video-assisted thoracoscopic surgery (VATS) for lobectomy:a report of 105 cases〔J〕.J Thorac Dis,2016,8(Suppl 3):S251-257.
[9] Lin Y,Zheng W,Zhu Y,et al.Comparison of treatment outcomes between single-port video-assisted thoracoscopic anatomic segmentectomy and lobectomy for non-small cell lung cancer of early-stage:a retrospective observational study〔J〕.J Thorac Dis,2016,8(6):1290-1296.
[10] Pastuszak-Lewandoska D,Kordiak J,Antczak A,et al.Expression level and methylation status of three tumor suppressor genes,DLEC1,ITGA9 and MLH1,in non-small cell lung cancer〔J〕.Med Oncol,2016,33(7):75.
[11] Jurišiĉ V,Obradoviĉ J,Tošiĉ N,et al.Effects of DMSO,glycerol,betaine and their combinations in detecting single nucleotide polymorphisms of epidermal growth factor receptor (EGFR) gene promoter sequence in non-small-cell lung cancer (NSCLC) patients〔J〕.J Pharm Biomed Anal,2016,128(5):275-279.
[12] Inagaki M,Shinohara Y,Kaburagi T,et al.S-1-containing chemotherapy for patients with non-small-cell lung cancer:A population-based observational study by the Ibaraki thoracic integrative (POSITIVE) research group〔J〕.Mol Clin Oncol,2016,4(6):1025-1030.
[13] Jin F,Zhu H,Fu Z,et al.Prognostic value of the standardized uptake value maximum change calculated by dual-time-point (18)F-fluorodeoxyglucose positron emission tomography imaging in patients with advanced non-small-cell lung cancer〔J〕.Onco Targets Ther,2016,9(5):2993-2999.
[14] Zhao Z,Su Z,Zhang W,et al.A randomized study comparing the effectiveness of microwave ablation radioimmunotherapy and postoperative adjuvant chemoradiation in the treatment of non-small cell lung cancer〔J〕.J BUON,2016,21(2):326-332.
[15] He J,Wang W,Li J,et al.Video-assisted thoracoscopic surgery tracheal resection and carinal reconstruction for tracheal adenoid cystic carcinoma〔J〕.J Thorac Dis,2016,8(1):198-203.
[16] Wang LM,Cao JL,Hu J.Video-assisted thoracic surgery for pulmonary sequestration:a safe alternative procedure〔J〕.J Thorac Dis,2016,8(1):31-36.
[17] Asteriou C,Lazopoulos A,Rallis T,et al.Video-assisted th- oracic surgery reduces early postoperative stress.A single-institutional prospective randomized study〔J〕.Ther Clin Risk Manag,2016,12(7):59-65.
[18] Shi JL,Jiang LH,Li DB,et al.Left lower lobectomy and systematic lymph node dissection by complete video-assisted thoracic surgery〔J〕.J Thorac Dis,2015,7(12):2376-2378.
(编辑:甘 艳)
Effects of Thoracic Surgery Combined with Chemotherapy and Chemotherapy Alone on Prognosis of Advanced Non-small Cell Lung Cancer
HANWenjian,XIAOLongmin,WUHong.NationalHospitalofEnshiAutonomousPrefecture,Enshi,445000
Objective To evaluate the effect of radiotherapy combined with chemotherapy on lung function,survival rate and quality of life of patients with advanced non-small cell lung cancer after radiotherapy.Methods 125 patients with advanced non-small cell lung cancer were selected.The patients were divided into 2 groups according to the random principle and the choice of the patients.The patients were divided into 2 groups:the thoracic surgery combined with chemotherapy group (n=65) and the chemotherapy alone group (n=60).The researchers calculated the survival time and the time of death of the patients during follow-up,and calculated the mortality rate during the three year follow-up period.Pulmonary function tests were performed 4 weeks after the end of treatment (including chemotherapy).The KPS score of the patients was followed up,and the average value of KPS score in the survival time was taken.Results The postoperative median survival time and survival rate were compared between the 2 groups,the difference was statistically significant (P<0.05).The lung function indexes of the thoracic surgery combined with chemotherapy group were better than those of the chemotherapy group,the difference was statistically significant (P<0.05).The postoperative KPS scores was 55~85 points,the thoracic surgery combined with chemotherapy group than in the chemotherapy group were significantly different (P<0.05).Conclusion The lung function,survival rate and life quality of patients with non-small cell lung cancer after the thoracic surgery combined with chemotherapy are better than that of the patients with chemotherapy alone.
Thoracic surgery;Chemotherapy;Non-small cell lung cancer;Lung function;Survival rate;Quality of life
445000 湖北省恩施州民族医院
10.3969/j.issn.1001-5930.2017.07.033
R734.2
A
1001-5930(2017)07-1152-04
2016-10-07
2017-03-27)
猜你喜欢
大电机技术(2021年3期)2021-07-16
世界最新医学信息文摘(2021年12期)2021-06-09
中外文摘(2020年13期)2020-08-01
福建基础教育研究(2020年4期)2020-05-28
时代英语·高三(2019年4期)2019-09-03
国际呼吸杂志(2019年5期)2019-03-30
电子制作(2017年20期)2017-04-26
腹腔镜外科杂志(2016年12期)2016-06-01
腹腔镜外科杂志(2016年9期)2016-06-01
股市动态分析(2015年29期)2015-09-10