肱骨近端交锁髓内钉和锁定接骨板治疗肱骨近端骨折的生物力学研究
2016-06-27 08:16:24周君琳赵会秦永超陆铁
中华肩肘外科电子杂志 2016年2期
周君琳 赵会 秦永超 陆铁
·论著·
肱骨近端交锁髓内钉和锁定接骨板治疗肱骨近端骨折的生物力学研究
周君琳1赵会1秦永超2陆铁1
目的 通过生物力学研究,对比两种治疗肱骨近端骨折内固定结构的力学特性,为临床应用提供理论基础。方法 将36根经防腐处理的成人肱骨干随机平均分为6组:试验组(A1髓内钉压缩组、A2髓内钉拉伸组、B1锁定板压缩组、B2锁定板拉伸组)和对照组(C1压缩对照组、C2拉伸对照组)。试验前对所有肱骨干标本进行骨密度检查,计算小组间有无显著性差异以排除骨质情况对固定稳定性的影响。所有标本均拍摄前、后位及侧位X线片,以排除术前骨折及其他骨病。试验组按照统一标准制作肱骨近端3部分外科颈大结节骨折模型。A1、A2组使用施乐辉TRIGENTM钛合金肱骨交锁髓内钉固定,肱骨远端为2枚交锁髓内钉固定,肱骨近端为4枚交锁髓内钉固定。B1、B2组使用AO肱骨近端锁定钛板内固定,肱骨远端为3枚皮质骨螺钉固定,肱骨近端为5枚松质骨螺钉固定。C1、C2组不做骨折模型及固定。对A1、B1、C1组进行轴向压缩试验,对A2、B2、C2组进行轴向拉伸试验,以固定失效为试验终止点。分别记录极限载荷和位移曲线,计算刚度。试验结果用SPSS12.0版软件进行统计学分析,P<0.05为差异具有统计学意义。结果 (1)A1、B1组的极限压缩载荷低于C1组(t=2.712、t=2.389,P值均<0.05),A1、B1组间比较差异无统计学意义(t=1.951,P>0.05),A2、B2组的极限拉伸载荷低于C2组(t=3.194、t=3.201,P值均<0.05),A2、B2组间比较差异无统计学意义(t=2.136,P>0.05);(2)A1、B1组的刚度低于C1组(t=2.826、t=2.837,P<0.05),A1、B1组间比较差异无统计学意义(t=2.004,P>0.05),A2、B2组的刚度低于C2组(t=2.357、t=2.481,P值均<0.05),A2、B2组间比较差异无统计学意义(t=2.108,P>0.05)。结论 肱骨近端交锁髓内钉和锁定接骨板在抗压缩和抗拉伸方面的生物力学强度无明显差异,交锁髓内钉可以提供与锁定板相近的固定强度。
肱骨近端骨折;内固定;肱骨近端交锁髓内钉;肱骨近端锁定接骨板;生物力学
肱骨近端骨折是老年骨质疏松患者的一种常见骨折。相对于其他手术治疗手段,目前最流行的是锁定钢板和髓内钉内固定,两种内固定手术方法各有优缺点。对其术前内固定方式的选择,目前是创伤骨科医师需要面临的问题[1]。本研究体外模拟人体防腐肱骨近端骨折,分别应用肱骨近端锁定接骨板和肱骨近端交锁髓内钉进行骨折固定。模拟内固定术后肩关节的负重状态,测量和计算骨折内固定模型的轴向载荷及刚度,探讨两种内固定器械的固定强度。从生物力学角度分析这两种内固定方式的特点。
资 料 与 方 法
一、肱骨标本的选取
选取甲醛浸泡的18具60~85岁尸体标本,取双侧肱骨标本共36根,其中男性标本14根,女性标本22根。修整标本,去除附着的软组织。首先应用Definium8000型DRX线拍片机(美国通用公司)拍摄标本正、侧位X线片,排除先天性畸形、骨折和肿瘤。应用UnigammaX-rayPlus骨密度仪(意大利I,acn公司)测量骨密度(统一划定肱骨头区域进行测量)[2]。
二、骨折内固定模型的建立
按Neer标准[3]及Kwon等[4]所介绍的方法,制作肱骨近端3部分骨折模型。在外科颈平面用摆锯对肱骨头进行截骨,锯片厚度1mm,在截骨面上确定结节间沟的位置,再沿结节间沟垂直于结节面向远端锯开,直至小结节基底水平(肱骨头截骨面的内侧最低点),在小结节基底水平垂直于肱骨干长轴将大结节由肱骨干近端截骨分离,复制肱骨近端3部分骨折模型见图1。

图1 肱骨近端3部分骨折模型
三、分组及内固定方法
所有手术操作在首都医科大学附属北京朝阳医院外科试验室完成,所有手术均由同一个三人小组完成,术后复查X线片确定内固定螺钉的位置。
将36根防腐处理成人肱骨干随机平均分为6组:试验组(A1髓内钉压缩组、A2髓内钉拉伸组、B1锁定板压缩组、B2锁定板拉伸组)和对照组(C1压缩对照组、C2拉伸对照组)。(1)A1和A2组:制作骨折模型,骨折复位后,使用施乐辉TRIGENTM肱骨近端钛合金交锁髓内钉固定(由北京施洛辉Smith&Nephew公司提供,其中主钉长度18cm,近端直径9mm,远端直径7.5mm,近端弯曲4°;近端锁钉10枚,长度36~60mm,直径5mm,螺距2mm;远端锁钉3枚,长度30mm,直径4mm,螺距2mm),肱骨干端为2枚锁钉固定,肱骨头端为4枚交锁螺钉固定。(2)B1 和B2 组:制作骨折模型,骨折复位后,于肱骨外侧使用AO/ASIF锁定肱骨近端钛板内固定(AO/ASIF五孔锁定肱骨近端钛合金接骨板及相关手术器械由PHILOS,Synthes公司提供,其中钛板长度114mm,厚度3.7mm,近端锁钉8枚,长度36~50mm,直径3.5mm,远端锁钉4枚,长度30mm,直径3.5mm),肱骨干端为3枚皮质骨螺钉固定,肱骨头端为5枚松质骨螺钉固定。(3)C1和C2组:不做骨折模型及固定。
6组标本均自肱骨髁上方10cm处横行锯断,上下两端置入圆柱形钢管夹具内,用甲基丙烯酸甲酯(自凝牙托粉)包埋备用,其中自凝牙托粉购于上海贝康公司。
四、生物力学测试方法及检测指标
1.轴向压缩试验:A1、B1、C1组每组6个标本。将标本竖直放置于WDW4100微机控制电子万能生物力学试验机(中国长春试验机研究所生产)上,远端完整地夹于试验机下部的夹具中,调整上压盘的位置,使之与标本近端完全接触,模拟人体肩部负重状态,持续加压,设定加载速度为0.01mm/s,直至固定失效。固定失效判定:(1)出现新骨折;或者骨折缝明显增宽;应力形变曲线中线性负载曲线出现偏离或中断,出现其一即为固定失效。(2)固定失效时的载荷为极限压缩载荷。(3)记录压缩位移曲线及极限压缩载荷。
2.轴向拉伸试验:A2、B2、C2组每组6个标本。将标本竖直放置于生物力学试验机上,近端夹于试验机上部的特制夹具中,远端完整地夹于试验机下部的夹具中,模拟人体重力拉伸的肩部受力情况,设定拉伸速率0.01mm/s,直至固定失效。固定失效判定:(1)出现新骨折;或者骨折缝明显增宽;应力形变曲线中线性负载曲线出现偏离或中断,出现其一即为固定失效。(2)固定失效时的载荷为极限拉伸载荷。(3)记录拉伸位移曲线及极限拉伸载荷。
五、统计学分析

结 果
一、操作前后肱骨标本大体和X线片
如图2~4所示。
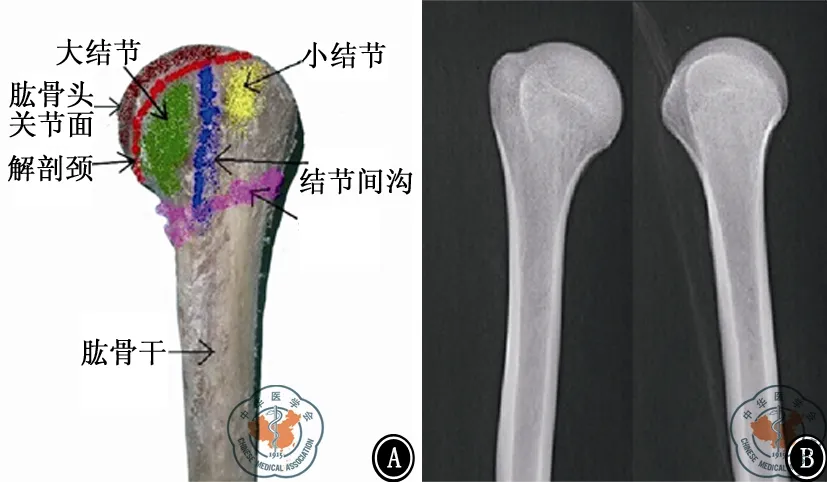
图2 未操作前大体标本(A)和X线片影像(B)
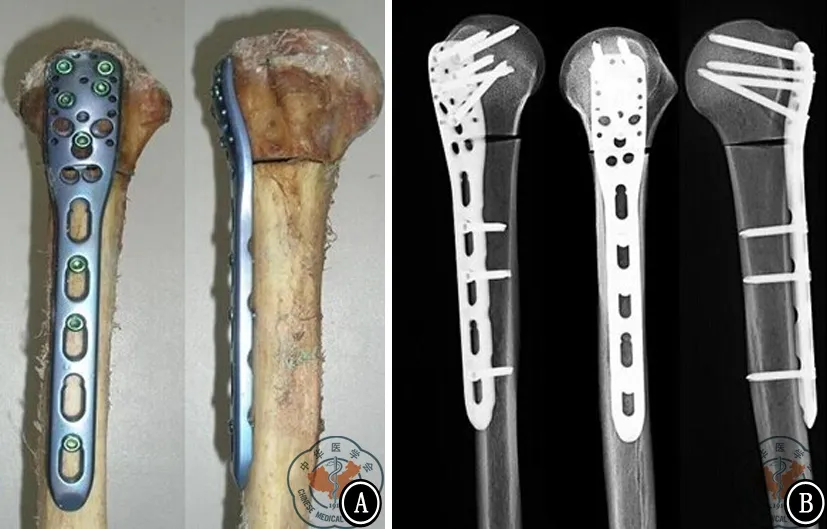
图3 AO/ASIF五孔锁定肱骨近端钛合金接骨板固定后大体标本(A)和X线片影像(B)

图4 TRIGENTM肱骨近端钛合金交锁髓内钉固定后大体标本(A)和X线片影像(B)
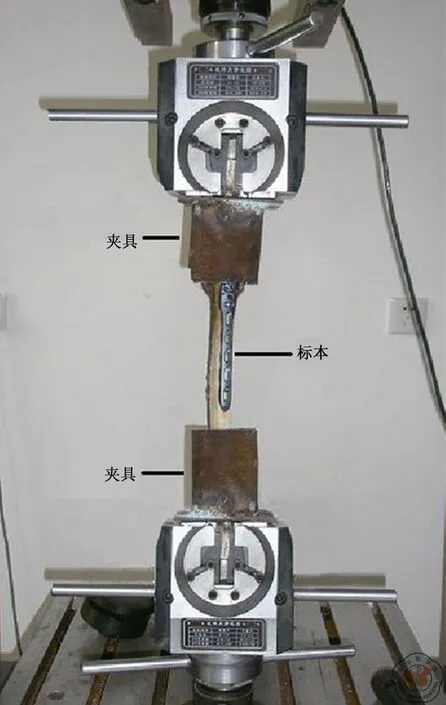
图5 生物力学试验照片
二、骨密度
如表1所示,各组之间差异无统计学意义(t=2.017,P>0.05)。

表1 六组骨密度测试结果比较±s)
三、压缩试验
如表2所示,A1、B1组的极限压缩载荷低于C1组(t=2.712、t=2.389,P值均<0.05),A1、B1组间比较差异无统计学意义(t=1.951,P>0.05);A1、B1组的刚度低于C1组(t=2.826、t=2.837,P值均<0.05),A1、B1组间比较差异无统计学意义(t=2.004,P>0.05)。

表2 三组压缩试验测试结果比较
四、拉伸试验
如表3所示,A2、B2组的极限拉伸载荷低于C2组(t=3.194、t=3.201,P值均<0.05),A2、B2组间差异无统计学意义(t=2.136,P>0.05);A2、B2组的刚度低于C2组(t=2.357、t=2.481,P值均>0.05),A2、B2组间差异无统计学意义(t=2.108,P>0.05)。
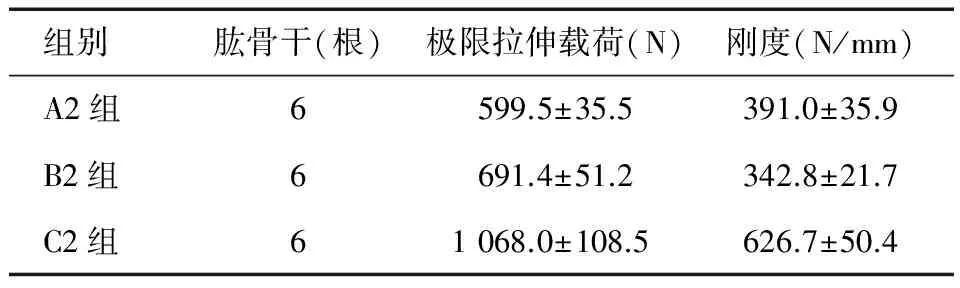
组别肱骨干(根)极限拉伸载荷(N)刚度(N/mm)A2组6599.5±35.5391.0±35.9B2组6691.4±51.2342.8±21.7C2组61068.0±108.5626.7±50.4
讨 论
肱骨近端骨折是老年骨质疏松患者临床常见的骨折类型,对于大部分无移位或轻微移位的骨折,非手术治疗可取得较好的临床疗效[5]。但是非手术治疗不能对骨折部位进行有效的原位固定和减压,手术治疗可以实现有效的内固定,并可以尽早进行功能锻炼以恢复肩关节功能。肩关节是人体活动范围最大的关节,肱骨近端骨折内固定术后需要可以耐受各个方向活动受力,同时保持骨折断端复位的稳定,内固定手术内植物需要承担活动范围的多向应力,以保持肱骨的解剖长度和序列稳定性[6]。本研究比较肱骨交锁髓内钉和锁定接骨板内固定术后的生物力学特性,发现肱骨近端交锁髓内钉和锁定接骨板在抗压缩和抗拉伸方面的生物力学强度无明显差异,交锁髓内钉可以提供与锁定接骨板相近的固定强度。
所有内固定都有各自的优缺点,交锁髓内钉可以通过闭合复位,与锁定接骨板相比,可以有效的防止软组织剥离破坏。另外,锁定接骨板减压和螺钉的植入过程时间相对较长,且增加了术中出血量。但是,在植入肱骨髓内钉的过程中,会对肩袖造成损伤,造成术后肩部疼痛的长期残留[7]。两种内固定方式都取得了积极可靠的临床疗效。当内固定失败的时候,经常发生内翻塌陷,是否可以有效地防止内翻塌陷的发生,也是影响内固定方式选择的因素之一[8-10]。
在内固定手术中,内固定材质的刚度通常不是内固定选择的影响因素。文献回顾发现过度的坚强内固定可以减小内固定的微活动,后续影响骨痂的形成,并导致延迟骨愈合甚至骨不连的发生。而对骨愈合影响最小的内固定角度、强度等参数尚且没有定论,既往的生物力学研究主要集中在循环负荷加载、扭转和其他的物理测试,而没有进行轴向负荷测试[11-12]。Edwards等[13]比较了肱骨近端髓内钉和3.5 mm锁定钢板的生物力学特性,发现锁定钢板优于髓内钉,但是他们仅仅进行循环负荷,而没有进行纯粹的轴向应力试验直到固定失败生物力学测试。在本研究中,不仅进行轴向压缩试验,也进行了拉伸试验,发现两者之间差异无统计学意义。
该研究的最大局限性是:目前还没有肱骨近端处理的标准流程,因此也没有肩关节的生物力学的基础数据可以参考。另外,作者没有进行模拟生理条件下肩关节多向运动的生物力学情况,在实际生理状态下,扭力剪切以及环形运动都会影响到内固定的应力效果,而在本研究中没有进行模拟考虑。此外,在临床工作中,大部分内固定失败的患者,不是因为进行单一动作导致的,而本研究中则是进行单一轴向压缩和拉伸进行到内固定失败。
肱骨髓内钉系统和锁定钢板在体外肱骨近端骨折模型上,抗压缩和抗拉伸方面的生物力学强度无明显差异,肱骨髓内钉系统可以提供与锁定钢板相近的固定强度。
[1] Misra A, Kapur R, Maffulli N. Complex proximal humeral fractures in adults--a systematic review of management[J]. Injury, 2001, 32(5): 363-372.
[2] Andresen R, Haidekker MA, Radmer S, et al. CT determination of bone mineral density and structural investigations on the axial skeleton for estimating the osteoporosis-related fracture risk by means of a risk score[J]. Br J Radiol, 1999, 72(858): 569-578.
[3] Neer CS 2nd.Displaced proximal humeral fractures. II. Treatment of three-part and four-part displacement[J].J Bone Joint Surg Am,1970,52(6):1090-1103.
[4] Kwon BK, Goertzen DJ, O′Brien PJ,et al. Biomechanical evaluation of proximal humeral fracture fixation supplemented with calcium phosphate cement[J].J Bone Joint Surg Am,2002,84A(6):951-961.
[5] Banco SP, Andrisani D, Ramsey M,et al.The parachute technique: valgus impaction osteotomy for two-part fractures of the surgical neck of the humerus[J].J Bone Joint Surg Am,2001,83A:s38-42.
[6] Warner JP, Costouros JG, Gerber C. Fractures of the proximal humerus [M]//Bucholz RW, Heckman JD, Court-Brown CM.Rockwood and Green′s fractures in adults. Philadelphia: Lippincott Williams & Wilkins, 2006:1164-1167.
[7] Hessmann MH, Hansen WS, Krummenauer F, et al. Locked plate fixation and intramedullary nailing for proximal humerus fractures: a biomechanical evaluation[J]. J Trauma, 2005, 58(6): 1194-1201.
[8] Gardner MJ, Weil Y, Barker JU, et al. The importance of medial support in locked plating of proximal humerus fractures[J]. J Orthop Trauma, 2007, 21(3): 185-191.
[9] Agudelo J, Schürmann M, Stahel P, et al. Analysis of efficacy and failure in proximal humerus fractures treated with locking plates[J]. J Orthop Trauma, 2007,21(10):676-681.
[10] Bottlang M, Doornink J, Byrd GD, et al. A nonlocking end screw can decrease fracture risk caused by locked plating in the osteoporotic diaphysis[J]. J Bone Joint Surg Am, 2009, 91(3): 620-627.
[11] Kitson J, Booth G, Day R. A biomechanical comparison of locking plate and locking nail implants used for fractures of the proximal humerus[J]. J Shoulder Elbow Surg, 2007, 16(3): 362-366.
[12] Füchtmeier B, May R, Hente R,et al.Proximal humerus fractures: a comparative biomechanical analysis of intra and extramedullary implants[J]. Arch Orthop Trauma Surg, 2007, 127(6): 441-447.
[13] Edwards SL, Wilson NA, Zhang LQ,Two-part surgical neck fractures of the proximal part of the humerus. A biomechanical evaluation of two fixation techniques[J].J Bone Joint Surg Am,2006,88(10):2258-2264.
(本文编辑:胡桂英)
周君琳,赵会,秦永超,等.肱骨近端交锁髓内钉和锁定接骨板治疗肱骨近端骨折的生物力学研究[J/CD]. 中华肩肘外科电子杂志,2016,4(2):87-92.
Biomechanicalinvestigationoncurrentfixationoptionsforproximalhumerusfractures:lockedintramedullarynailandlockedplate
ZhouJunlin1,ZhaoHui1,QinYongchao2,LuTie1.
1DepartmentofOrthopedics,BeijingChaoyangHospital,CapitalMedicalUniversity,Beijing100028,China;2DepartmentofOrthopedics,PekingUniversityFirstHospitalFengtaiHospital,Beijing100028,ChinaCorrespondingauthor:ZhouJunlin,Email:zhoujunlin@medmail.com.cn
Background Proximal humeral fracture is a common fracture in elderly patients with osteoporosis, locking plate and intramedullary nail fixation are the most popular methods for its surgical treatment at present. There are advantages and disadvantages for both methods of internal fixation treatment. Currently, the choice of internal fixation method is a problem faced by traumatic orthopedic doctors. In this study we used proximal humeral locking plate or interlocking intramedullary nail for fracture fixation in vitro human samples with anticorrosive treatment tosimulate theload condition of shoulder joint after internal fixation, measured and calculated the axial load and stiffness of the fracture model, and discussed the fixed strength of the two internal fixation devices. We also analyzed the characteristics of these two kinds of internal fixation methods from the perspective of biomechanics.Methods (1)Selection of humeralsamples.A total of 36 humeralsamples with antiseptic treatment wereselected from 18 specimens of 60-85 years old, including 14 male samplesand 22 female samples. The X-ray films of the samples were taken to exclude congenital deformity, fracture and tumor. We appliedUnigamma X-ray Plus bone mineral density instrument to measure bone mineral density (humeral head area were unified delimited), results in each group were recorded for variance analysis.(2)Construction of fracture model with internal fixation.According to Neerclassification and the method introduced by Kwon, we produced three-partproximal humeral fracture model. We cut the humeral head with a oscillating saw at the surgical neck plane, the thickness of saw blade was 1 mm, confirmed the position of intertubercular sulcus on the osteotomy plane, then saw the bone along intertubercular sulcus to the distal humerus, thedirection is perpendicular to the osteotomy plane, until to the base of the lesser tubercle level, cut the greater tuberosity from proximal humerusat the base of lesser tuberosity, the direction is perpendicular to the long axis of the shaft.(3)Grouping and internal fixation method.All operationswere performed by a same team in the surgical lab of Beijing Chaoyang Hospital affiliated to the Capital Medical University, postoperative X-ray filmswere taken to confirm the location of the internal fixation screws.Thirty-six embalmed adult shaft samples were divided into 6 groups randomly: the experimental group (A1 intramedullary nailing compression group, A2 intramedullary nail stretching group, B1 locking plate compression group, B2 locking plate stretching group) and control group (C1 compression control group, C2 stretching control group).A1 and A2 groups: (1)Producedfracture models, the fractures were fixed with TRIGENTM titanium alloylocking proximal humeral intramedullary nail (provided by Beijing Smith & Nephew company, of which the main nail length is 18 cm, proximal diameter is 9 mm, distal diameter is 7.5 mm, proximal bending is 4°, there were 10 proximal interlocking screws, the length is 36-60 mm, the diameter is 5 mm, there are 3 locking screws at distal humerus, the length is 30 mm, the diameter is 4 mm), humeral shaft were fixed with 2 locking screws, humeral headwere fixed with 4 locking screws.(2)B1 and B2 group: produced fracture models, the humeral fractures were fixed with AO/ASIFlateral titanium proximal humeral locking plate (AO/ASIF titanium alloy proximal humeral locking plate with five holesand related surgical instruments provided by the Synthes company, the length ofthe plate is 114 mm, the thickness is 3.7 mm, there are 8 proximal screws, length is 36-50 mm, the diameter is 3.5 mm, there are 4 distal locking screws, the length is 30 mm, the diameter is 3.5 mm), there are 3 cortical bone screws in the humeral shaft, 5 cancellous bone screws in the humeral head for fixation. (3)C1 and C2 groups: no fracture modelor fixation.All samples in 6 groups were sawed off from 10 cm above the humeral condyle,both ends were fixed in cylindrical steel pipe clamp, embedded with methyl methacrylate (Shanghai Nutrinen company).(4)Biomechanical test method and parameter.(A)Axial compression test: There were 6 samples in A1, B1 and C1 group respectively.Samples were place vertically on the electron universal biomechanical testing machine controlled by WDW4100 microcomputer (produced by Changchun testing machine institute, China), distalhumeral shift were fixed on the gripper at thebottom of the machine, modified the position of the pressure plate forcompletely contact with proximal of the samples, simulating theload state of human shouldersduring sustained compression, set the loading speed to 0.01 mm/s, until fixation failure.Fixation failure criteria: (a) new fracture occurred;fracture linesbroadening obviously;deviation or interruption of the linear load curve appeared in stress-strain curve, one of above is the mark of fixation failure. (b)fixationfailure load is same with the ultimate compression load. (c) record compressive-displacement curve and ultimate compression load.(B)Axial tensile test: There were 6 samples in A2, B2,C2 group respectively. Samples were placed vertically on the biomechanical test machine, with proximal humeral fixed to the gripper at the top of the machine, distal humeral shift fixedto the bottom of the tester, simulating human shoulder force of gravity stretch, set the stretching rate to 0.01 mm/s, until fixation failure. Fixation failure criteria: (a) new fracture occurred, fracture lines broadening obviously, deviation or interruption of the linear load curve appeared in stress-strain curve, one of above is the mark of fixed failures. (b) fixation failure load is same with the ultimate tensile load;(c) record tensile-displacement curve and ultimate tensile load.(5)Statistics processing.Data from density of bone samples and biomechanical test were analyzed by SPSS12.0 statistics software, the results were compared with variance analysis andttest,andP<0.05wasconsideredsignificant.ResultsTheultimatecompressionloadoffixationgroupswerelowerthanthatofthecontrolgroup(P<0.05),nosignificantdifferencebetweengroupsoffixations(P>0.05).Thetensileloadoffixationgroupswerelowerthanthatofthecontrolgroup(P<0.05).Thestiffnessofthefixationgroupswerelowerthanthatofthecontrolgroup(P<0.05).Nosignificantdifferencewasdetectedbetweenthefixationgroupswithdifferentloads(P>0.05).ConclusionsBiomechanicaltestingofmodernfixationoptionsforproximalhumeralfractureexhibitedthatthebiomechanicalstrengthincompressionandtensileresistanceissimilaraffordedbyPHNandLPHP,bothdevicescanprovidestablefixationinthetreatmentofproximalhumeralfractures.However,prospectiveclinicaltrialswithlongerfollowing-uparerequiredfordefinitiveassessmentoftheidealfixationchoiceforsurgicaltreatmentofproximalhumeralfractures.
Proximalhumerusfracture;Internalfixation;Proximalhumeruslockedintramedullarynail;Lockedproximalhumerusplate;Biomechanics
10.3877/cma.j.issn.2095-5790.2016.02.005
国家自然科学基金项目(81202124)
100028首都医科大学附属北京朝阳医院骨科1;100071北京大学第一医院丰台医院骨科2
周君琳,Email:zhoujunlin@medmail.com.cn
2015-07-20)
猜你喜欢
中华养生保健(2020年10期)2021-01-18 06:45:16
中华肩肘外科电子杂志(2019年4期)2019-08-24 06:38:52
中华骨与关节外科杂志(2016年5期)2016-05-17 06:10:58
西南军医(2016年4期)2016-01-23 02:19:16
中国卫生标准管理(2015年16期)2016-01-20 09:26:21
中国医疗器械杂志(2015年5期)2015-12-31 06:15:28
动物医学进展(2015年10期)2015-12-07 05:46:22
实用手外科杂志(2015年2期)2015-08-28 09:50:48
实用手外科杂志(2015年4期)2015-08-27 01:54:18
西南医科大学学报(2014年6期)2014-03-20 15:43:53