
50例磁性附着体在口腔义齿修复中的应用效果观察
2016-06-14 08:40石国成陈丽丹黄剑杰
重庆医学 2016年2期
石国成,陈丽丹,黄剑杰
(浙江省诸暨市中医院口腔科,浙江绍兴 311800)
50例磁性附着体在口腔义齿修复中的应用效果观察
石国成,陈丽丹,黄剑杰
(浙江省诸暨市中医院口腔科,浙江绍兴 311800)
[摘要]目的观察磁性附着体在口腔活动义齿修复中的应用效果。方法选择2012年4月至2014年4月于该科治疗的覆盖义齿修复患者共50例,对基牙进行预备后行磁性附着体修复,观察并记录患者咀嚼效率、满意度及修复后并发症的发生情况。结果给予磁性附着体修复后即刻咀嚼效率0.65±0.09,较修复前(0.22±0.04)咀嚼效率明显升高(t=20.812,P<0.05),修复后1年咀嚼效率(0.71±0.13),较修复前咀嚼效率高(t=25.060,P<0.05)。修复后即刻咀嚼效率与修复后1年咀嚼效率差异无统计学意义(t=0.018,P>0.05)。修复后即刻满意49例,较满意1例,满意度100%,明显高于修复前(46%),χ2=31.815,P<0.05。修复后1年满意45例,较满意5例,满意度100%,明显高于修复前(χ2=31.815,P<0.05)。结论采用磁性附着体修复牙列缺失或牙列缺损能明显改善患者的咀嚼效率,较传统活动义齿能明显缩短患者的适应时间,提高患者的满意度,具有广阔的临床应用前景。
[关键词]磁性附着体;义齿,局部,暂时; 义齿,全口;义齿,覆盖;咀嚼效率
口腔修复指利用人工装置对口腔内牙齿及相关附属组织发生的缺损进行恢复至正常功能和外形[1],龋病、牙周病及口腔颌面外伤等原因均可能导致牙列缺损或牙列缺失。过去往往采用局部可摘活动义齿或总义齿进行修复,但随着临床应用时间的推移,其修复后远期出现固位和稳定方面的不足逐渐显露[2],而采用种植进行修复的方法则因需花费患者大量费用而难以在临床上得到广泛开展。磁性附着体一方面具有固位稳定,另一方面修复费用相对便宜,故在临床上的应用较为广泛[3]。作者自2012年4月至2014年4月采用磁性附着体进行覆盖修复,效果较为理想,现将相关情况报道如下。
1资料与方法
1.1一般资料选择2012年4月至2014年4月于本科治疗的覆盖义齿修复患者共50例,其中男22例,女28例,患者年龄最小者42岁,最大者71岁,平均年龄(60.8±9.1)岁。行上颌全口覆盖义齿修复者共18例,行下颌全口覆盖义齿修复者共21例,行可摘局部义齿修复者共11例。所有患者行修复治疗前均给予相关影像学检查以了解牙根情况,拔除无保留价值的残根。纳入标准:(1)所有患者在本次修复前均有佩戴覆盖义齿经验;(2)牙根在牙槽骨内长度至少是牙根总长度的2/3,且牙根长度不少于8 mm;(3)基牙动度不超过Ⅰ°;(4)患者依从性较好,能配合随访,并同意将随访结果用于本研究资料。排除标准:排除存在根尖周病变者;本研究方案经上报医院伦理委员会论证通过后实施,所有患者参与本研究前均签署知情同意书。
1.2方法
1.2.1材料磁性附着体(日本爱知制钢,Magfit EX600W,Magfit EX400W),钴铬合金(日本GC),自凝塑料、玻璃离子(日本松风),聚酯硅橡胶(美国3M)。
1.2.2基牙预备基牙根管治疗和牙周基础治疗至少于修复治疗前一周进行,将牙根齐龈缘磨平,中心部位用磨头作一凹面,视根横截面形态于较厚处作一抗旋转沟(直径约为1 mm,深度约为2 mm)。

1.2.4修复后观察指标采用吸光度法测定磁性附着体修复前、修复后即刻及修复后1年患者的咀嚼效率。调查修复1年后患者对修复效果的满意度,随访复查记录修复后发生牙龈炎、基牙龋齿、义齿断裂等的发生情况。

2结果
2.1修复前后患者咀嚼效率改变情况给予磁性附着体修复后即刻咀嚼效率较修复前咀嚼效率明显升高(t=20.812,P<0.05),修复后1年咀嚼效率,较修复前咀嚼效率高(t=25.060,P<0.05)。修复后即刻咀嚼效率与修复后1年咀嚼效率差异无统计学意义(t=0.018,P>0.05)。见表1。
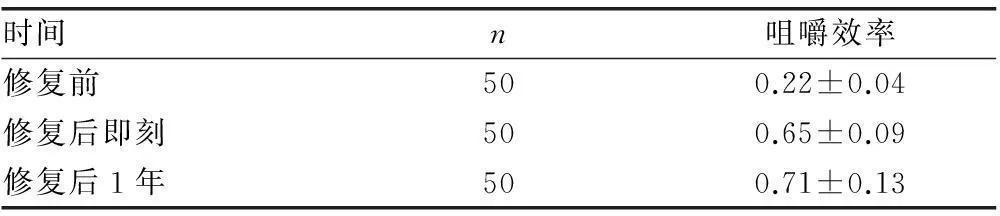
表1 修复前后患者咀嚼效率改变情况
2.2修复后患者满意情况修复前仅23例患者对所使用的活动义齿较满意,修复后即刻满意49例,较满意1例,满意度100%,明显高于修复前(χ2=31.815,P<0.05)。修复后1年满意45例,较满意5例,满意度100%,明显高于修复前(χ2=31.815,P<0.05)。
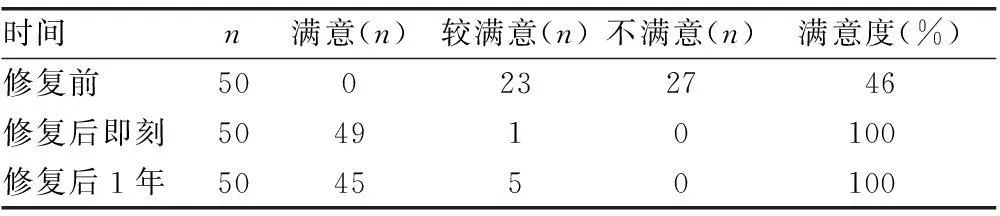
表2 修复后患者满意情况
2.3修复后并发症发生情况患者在随访中发生牙龈炎1例(2.00%),根面龋4例(8.00%)。并发症总发生5例(10.00%)。
3讨论
口腔修复主要是通过口腔修复医生设计出相应的人工装置来将患者口内的缺损或畸形组织恢复至正常的外形或(和)功能。利用磁性附着体来修复牙列缺损和牙列缺失是近些年在临床上才开始应用起来的修复方式,与传统的可摘局部义齿不同,磁性附着体的固位力来自于固定在义齿内的磁体与固定于根帽上的衔铁所产生的相互吸引[4]。对于下颌全口覆盖义齿而言,基牙的分布亦在一定程度上会影响到固位的效果[5],一般来说,基牙分布越分散,可为义齿提供的稳定性和固位能力越好[6],加上应用磁性附着体时对就位道并无特殊要求,在任何方向上均可就位[7],故理论上可应用在任何牙位。但在实际应用中,通常设置2~4个附着体[8],且位置尽可能设置分散且对称可获得更好的对抗翘动和摆动的效果[9]。传统的可摘局部义齿或全口覆盖义齿修复后患者需要3~6周时间进行适应才能正常行使咀嚼功能[10],而采用磁性附着体义齿修复后多数患者在修复完成当天即可适应,加上基托面积明显少于传统活动义齿,患者佩戴后的异物感亦显著减轻,对患者的发音功能亦不会造成明显影响[11]。
采用磁性附着体进行覆盖义齿修复时还需要重视保护基牙及长期维持修复效果。磁性附着体有利于基牙冠根比的调整,可避免基牙受到过大的侧向力[12],对于Ⅰ°松动的基牙而言,进行完善的牙周基础治疗及截冠后,松动度往往有明显的改善,部分病例中基牙甚至可恢复稳固[13],增加了覆盖基牙的留存时间,避免或大幅延迟基牙被拔除的时间,明显减缓牙周骨组织的吸收速度[14]。研究结果表明,磁性附着体几乎不会传递受到的侧向力[15],即使在行使咀嚼功能时承受侧向力,对基牙仍产生一个沿长轴方向传导的压应力,而正常的牙周膜则可均匀分散这些应力[16],这样有利于保护基牙健康,避免对基牙及周围黏膜产生压痛[17]。
本研究结果显示,给予磁性附着体修复后即刻咀嚼效率较修复前咀嚼效率明显升高(t=20.812,P<0.05),修复后1年咀嚼效率较修复前咀嚼效率高(t=25.060,P<0.05)。修复后即刻咀嚼效率与修复后1年咀嚼效率差异无统计学意义(t=0.018,P>0.05)。修复后即刻满意49例,较满意1例,满意度100%,明显高于修复前(χ2=31.815,P<0.05)。修复后1年满意45例,较满意5例,满意度100%,明显高于修复前(χ2=31.815,P<0.05)。咀嚼效率是义齿修复的一个重要指标,由于咀嚼效率存在明显的个体差异,故本研究中对修复前后的咀嚼效率改变情况采用了自身对照,排除了其他因素对咀嚼效率可能存在的影响。
磁性附着体在正常使用情况下可能出现以下问题:(1)牙周炎或基牙龈缘炎,在佩戴磁性附着体后,位于义齿与口腔组织之间的唾液流量少,流速慢,清洁功能下降,利于微生物的附着。加上局部氧化还原的电势差及局部微环境氧含量的改变,促进龈沟内形成厌氧环境,为革兰阴性厌氧菌的生长提供条件。此外,衔铁设计位置、表面是否光洁等均可能影响菌斑的附着而引起基牙牙周或龈缘的炎症[18];(2)基牙发生松动或脱落,往往见于设计缺陷,义齿设计沉降不足,磁性附着体处形成支点,应力过度集中,较长时间可能引起基牙的松动或脱落[19];(3)基牙根面继发龋坏,基牙根面继发龋坏是相对较为常见的修复后并发症,常见于衔铁未能完全覆盖牙根表面或粘结剂发生溶解[20];(4)义齿断裂,过度的应力集中即可能导致义齿发生断裂,应力集中的地方通常位于覆盖磁性附着体基牙的部位,由于义齿承受咀嚼压力后不能均匀下沉,加上粘结磁性附着体处的基托厚度相对薄,故易在此处发生断裂。
综上,采用磁性附着体修复牙列缺失或牙列缺损能明显改善患者的咀嚼效率,较传统活动义齿能明显缩短患者的适应时间,提高患者的满意度,具有广阔的临床应用前景。
参考文献
[1]Goto T,Nagao K,Ishida Y,et al.Influence of matrix attachment installation load on movement and resultant forces in implant overdentures[J].J Prosthodont,2015,24(2):156-163.
[2]Yang TC,Maeda Y,Gonda T,et al.Magnetic attachment for implant overdentures:influence of contact relationship with the denture base on stability and bending strain[J].Int J Prosthodont,2013,26(6):563-565.
[3]Gonda T,Yang TC,Maeda Y.Five-year multicenter study of magnetic attachments used for natural overdenture abutments[J].J Oral Rehabil,2013,40(4):258-262.
[4]Cristache CM,Muntianu LA,Burlibasa M,et al.Five-year clinical trial using three attachment systems for implant overdentures[J].Clin Oral Implants Res,2014,25(2):e171-178.
[5]Kanbara R,Nakamura Y,Ochiai KT,et al.Three-dimensional finite element stress analysis:the technique and methodology of non-linear property simulation and soft tissue loading behavior for different partial denture designs[J].Dent Mater J,2012,31(2):297-308.
[6]Takeshita S,Kanazawa M,Minakuchi S.Stress analysis of mandibular two-implant overdenture with different attachment systems[J].Dent Mater J,2011,25(3):119-125.
[7]Haruta A,Matsushita Y,Tsukiyama Y,et al.Effects of mucosal thickness on the stress distribution and denture stability of mandibular implant-supported overdentures with unsplinted attachments in vitro[J].J Dent Biomech,2011(1):894395.
[8]Chen J,Tomotake Y,Watanabe M,et al.Telescopic magnetic attachment for implant-supported denture:evaluation of splint effect[J].Int J Oral Maxillofac Implants,2011,26(3):657-664.
[9]Maeda Y,Yang TC,Kinoshita Y.Development of a self-adjusting magnetic attachment for implant overdentures[J].Int J Prosthodont,2011,24(3):241-243.
[10]Hasegawa M,Umekawa Y,Nagai E,et al.Retentive force and magnetic flux leakage of magnetic attachment in various keeper and magnetic assembly combinations[J].J Prosthet Dent,2011,105(4):266-271.
[11]Yang TC,Maeda Y,Gonda T,et al.Attachment systems for implant overdenture:influence of implant inclination on retentive and lateral forces[J].Clin Oral Implants Res,2011,22(11):1315-1319.
[12]Akin H,Coskun ME,Akin EG,et al.Evaluation of the attractive force of different types of new-generation magnetic attachment systems[J].J Prosthet Dent,2011,105(3):203-207.
[13]Ceruti P,Bryant SR,Lee JH,et al.Magnet-retained implant-supported overdentures:review and 1-year clinical report[J].J Can Dent Assoc,2010,76(4):a52.
[14]Pae A,Kim JW,Kwon KR.Immediate loading of two implants supporting a magnet attachment-retained overdenture:one-year clinical study[J].Implant Dent,2010,19(5):428-436.
[15]Cune M,Burgers M,Van Kampen F,et al.Mandibular overdentures retained by two implants:10-year results from a crossover clinical trial comparing ball-socket and bar-clip attachments[J].Int J Prosthodont,2010,23(4):310-317.
[16]Ellis JS,Burawi G,Walls A,et al.Patient satisfaction with two designs of implant supported removable overdentures;ball attachment and magnets[J].Clin Oral Implants Res,2009,20(11):1293-1298.
[17]Vere J,Deans RF.Tooth-supported,magnet-retained overdentures:a review[J].Dent Update,2009,36(5):305-308,310.
[18]Preiskel HW,Preiskel A.Precision attachments for the 21st century[J].Dent Update,2009,36(4):221-224,226-227.
[19]Kawamoto S,Hamamura S,Kawahara H,et al.Use of a magnetic attachment to retain an obturator prosthesis for an osseous defect[J].J Prosthodont,2009,18(4):359-362.
[20]Saha S,Ray-Chaudhuri A.Mandibular implant-retained complete overdenture using retentive abutments:a case report[J].Dent Update,2009,36(3):154-158.
Effect observation of 50 cases magnetic attachments application on oral denture restoration*
ShiGuocheng,ChenLidan,HuangJianjie
(DepartmentofStomatology,TraditionalChineseMedicineofZhujiCity,Shaoxing,Zhejiang311800,China)
[Abstract]ObjectiveTo observe the effect of magnetic attachments application on oral denture restoration.MethodsA total of 50 patients with overdenture restoration treatment in this department from April 2012 to April 2014 were enrolled.Abutment tooth were given magnetic attachments restoration after preparations.The masticatory efficiency,patient satisfaction and post-restoration complication were observed and recorded.ResultsThe immediate masticatory efficiency after magnetic attachments restoration (0.65±0.09) was significant higher than that before restoration(0.22±0.04),t=20.812,P<0.05.After one-year′s magnetic attachments restoration,masticatory efficiency(0.71±0.13) was higher than that before restoration(t=25.060,P<0.05).There was no statistic difference in magnetic attachments restoration between immediate masticatory efficiency and one-year masticatory efficiency(t=0.018,P>0.05).There were 49 cases of immediate satisfaction and 1 case of satisfactory after restoration,the patient satisfaction rate was 100%,it was significant higher than that of before restoration(46%),χ2=31.815,P<0.05.There were 45 cases of satisfaction and 5 case of satisfactory after restoration,the patient satisfaction rate was 100%,it was significant higher than that of before restoration (χ2=31.815,P<0.05).ConclusionThe masticatory efficiency could be improved significantly by magnetic attachments to restore denture depletion or dentition defect,compare with traditional denture,it can significant shorten adapt time for patients,and it can enhance patient satisfaction.It has wide prospect for future clinical application.
[Key words]magnetic attachments;denture,partial,temporary;denture,complete;denture,overlay;masticatory efficiency
doi:论著·临床研究10.3969/j.issn.1671-8348.2016.02.017
基金项目:浙江省卫生厅一般项目(2013KYB247)。
作者简介:石国成(1966-),主治医师,本科,主要从事口腔科研究。
[中图分类号]R783.4
[文献标识码]A
[文章编号]1671-8348(2016)02-0199-03
(收稿日期:2015-09-01修回日期:2015-09-25)
猜你喜欢
口腔医学(2021年1期)2021-02-27
口腔疾病防治(2020年7期)2020-06-11
中华老年口腔医学杂志(2016年3期)2017-01-15
中华老年口腔医学杂志(2016年2期)2017-01-15
西南国防医药(2016年6期)2016-12-01
新疆医科大学学报(2016年11期)2016-11-15
中国医药导报(2016年21期)2016-02-17
中国医疗美容(2015年2期)2015-07-19
中国医疗美容(2015年1期)2015-07-12
中国医药指南(2014年9期)2014-01-29
