重T2WI和增强T1WI MRI联合评估泪囊鼻泪管的优势
2016-04-28 03:23司建荣张雅丽金梅戴灼南杜洁嫦
磁共振成像 2016年1期
司建荣,张雅丽,金梅,戴灼南,杜洁嫦
重T2WI和增强T1WI MRI联合评估泪囊鼻泪管的优势
司建荣1*,张雅丽1,金梅2,戴灼南1,杜洁嫦1
[摘要]目的 探讨MRI重T2WI (h-T2WI)和增强T1WI (Ce-T1WI)组合序列对正常和阻塞的泪囊鼻泪管的显示能力。材料与方法 在脂肪抑制的基础上,用h-T2WI和Ce-T1WI序列,薄层连续扫描正常和有阻塞的泪囊鼻泪管,扫描方位是轴面(AP)和冠状面(CP),用静态和动态两种扫描方式。结果 静态扫描正常泪囊鼻泪管23例46侧,其中24侧用h-T2WI+Ce-T1WI+AP+CP组合,6侧用h-T2 WI+Ce-T1 WI+AP组合,8侧用h-T2 WI+AP+CP组合,8侧用Ce-T1WI+AP+CP组合。动态轴面扫描正常泪囊鼻泪管10例20侧,均用h-T2WI+AP组合。静态扫描阻塞的泪囊鼻泪管9例10侧,均用h-T2WI+Ce-T1WI+AP+CP组合。正常和有阻塞的泪囊鼻泪管均能被良好显示。(1)正常的泪囊鼻泪管:静态扫描见泪囊鼻泪管的管腔狭小,鼻泪管更小,并且形态多样;动态扫描见部分节段的管腔可自主性增大或变小。横断面上泪囊呈长椭圆形(16侧)或裂隙状(30侧),移行部均呈半月形,鼻泪管呈短椭圆形(28侧)或类圆形(18侧)。用静态h-T2WI序列,轴面图像上94.7% (36/38 侧)的泪囊鼻泪管呈现了3层信号结构,冠状面图上31.2% (10/32 侧)呈现了3层信号结构;这3层信号结构分别代表了管腔内容物、管壁内1/4和管壁外3/4;管腔内的泪液、泪膜和空气分别呈最高信号、高信号和最低信号;管壁内1/4呈低信号,管壁外3/4呈高信号。在Ce-T1WI序列上,管壁可以被明显强化。(2)有阻塞的泪囊鼻泪管:梗阻部位和病变的范围均被精确显示,其中管腔狭窄1侧,闭塞9侧;梗阻点以上管腔积液(脓)扩张,管壁变薄;梗阻点管腔消失或明显狭小,在h-T2WI上丧失3层信号结构。结论 h-T2WI结合Ce-T1WI序列的MRI,可以清晰的显示正常生理状态下的泪囊鼻泪管的管腔、管壁的层次和行经;也能够精确显示有梗阻的泪囊鼻泪管的梗阻部位、病灶范围,区分有血供和无血供的组织结构。动态h-T2WI发现正常管腔的大小有自主性变化。
[关键词]泪器;磁共振成像;图像增强
1.广东省中西医结合医院放射科,佛山 528200
2.广东省中西医结合医院眼科,佛山528200
司建荣, Email: sjr1963nian@sina.com
接受日期:2015-11-27
司建荣, 张雅丽, 金梅, 等.重T2WI和增强T1WI MRI联合评估泪囊鼻泪管的优势.磁共振成像, 2016, 7(1): 20–27.
Benefits of the combination of MRI heavily-T2WI and contrast-enhanced T1WI pulse sequences to examine human lacrimal sac and nasolacrimal duct
SI Jian-rong1*, ZHANG Ya-li1, JIN Mei2, DAI Zhuo-nan1, DU Jie-chang1
1Department of Radiology, Guangdong Provincial Hospital of Integrated Traditional Chinese and Western Medicine, Foshan 528200, China
2Ophthalmology Department, Guangdong Provincial Hospital of Integrated Traditional Chinese and Western Medicine, Foshan 528200, China
*Correspondence to: Si JR, E-mail: sjr1963nian@sina.com
Received 28 Sep 2015, Accepted 27 Nov 2015
Abstract Objective: To evaluate capability of the combination of magnetic resonance imaging (MRI) heavily-T2 weighted imaging (h-T2WI) and contrastenhanced T1 weighted imaging (Ce-T1WI) pulse sequences revealing the anatomic details of normal or obstructed human lacrimal sac (LS) -nasolacrimal duct (NLD).Materials and Methods: Using 1.5 T MRI system, the normal and obstructed human LS-NLDs were imaged by h-T2WI and Ce-T1WI pulse sequences both with the fatsaturation technique.LS-NLD was scanned on its axial plane (AP) and coronal plane (CP).The thinnist slice thickness, consecutive sections (no spacing), static and dynamic scanning procedures were adopted.Results: Forty-six sides of normal LS-NLD(23 subjects) were imaged with the static scanning.Of them 24 sides were scanned with a combination of h-T2WI+Ce-T1WI+AP+CP, 6 sides with a combination of h-T2WI+Ce-T1WI+AP, 8 sides with a combination of h-T2WI+AP+CP, 8 sides with a combination of Ce-T1WI+AP+CP.The static scanning of 10 sides of obstructed LS-NLD (9 patients) was performed with a combination of h-T2WI+Ce-T1WI+AP+CP.The dynamic scanning of 20 sides of normal LS-NLD (10 subjects) was done with a combination of h-T2WI+AP.The normal and obstructed LS-NLDs were revealed vividly.(1)The normal LS-NLD.On the static scanning, their lumens were narrow and small, the size and shape of their lumens varied at different levels of LS-NLD, and NLD lumen was narrower and smaller than LS.On the dynamic scanning, the autonomous lumen changes (getting small or large) had been noticed.On cross sectional view, LS was long-ellipse (16 sides) or slit-shaped (30 sides), the junction was crescent, and NLD was short-ellipse (28 sides) or circular (18 sides).By h-T2WI, three-layer different signal intensities were revealed on a lot of images of LS-NLD, and 94.7% (36/38 sides) and 31.2% (10/32 sides) of LS-NLDs showed this signal pattern on axial and coronal scanning respectively.The three layer signals represented respectively (a) contents (tear, tear film or air) in their lumens, (b) medial part of their wall that was smaller than a quarter of their wall thickness and (c) lateral part of their wall that was more than three-fourths of their wall thickness.The tear, the tear film and the air in their lemen gave the most hyper-intense signal, middle-intense signal and the most hypo-intense signal respectively.The medial part and lateral part wall gave a hypo- and middle-intense signals respectively.The medial part wall consists of the epithelium layer, blood capillary layer and postcapillary venule layer, and the latter both are embedded in the lamina propria.The lateral part wall is venous lacunae layer embedded in the lamina propria, too.Ce-T1WI was able to enhance obviously the signal intensity of LS-NLD wall, therefor to promote distinguishing their wall from lumen (or contents).(2) The obstructed LS-NLD.Location and extent of the obstructive lesions were revealed precisely in all of the obstructed LS-NLDs.One side was lumen stricture and 9 sides were lumen occlusion.A lot of liquid (or pus) had been accumulated in the proximal LS-NLD lumen of the obstruction site, the lumen was dilatated, its wall was thinned and only showed one signal intensity.The lumen stricture might be revealed like an “hourglass” pattern.The site of lumen occlusion lost the normal three-layer signal pattern.Conclusions: MRI h-T2WI combined with Ce-T1WI pulse sequences can vividly reveal the lumen (or natures of the contents), wall and route of the normal human LS-NLD in normal physiological condition, and even can reveal detailed layers of their wall.They also can reveal the precise location and extent of lesions in the obstructed LS-NLDs.The tissues with blood supply can be distinguished from one (or the contents) without blood supply by this way.The autonomous size change of the normal LS-NLD lumens is revealed by the dynamic h-T2WI.This combination of MR pulse sequences can achieve aims of other imaging methods which are used to reveal LS-NLD and their lesions, so it is likely to replace the other approaches of dacryocystography with the combination.
Key words Lacrimal apparatus; Magnetic resonance imaging; Image enhancement
泪囊鼻泪管MRI检查,无放射线辐射,医源性损伤风险低,并可做到非侵入性;目前常用的方法是MR泪囊造影术(MR dacryocystography,MR DCG),或MR泪道水成像(MR hydrography)[1-9],目标是显示它们的管腔。本研究是在MR脂肪抑制技术基础上,用重T2WI和增强T1WI序列,在轴面和冠状面两个方位上连续薄层扫描泪囊鼻泪管,目的是探求一种既能显示管腔、又能显示管壁的MRI序列组合;同时,观察正常和有阻塞的泪囊鼻泪管的静态MRI表现,观察正常管腔形态和大小的动态变化。
1 材料与方法
1.1研究对象
1.1.1静态扫描正常的泪囊和鼻泪管
共23例46侧;男10例,女13例,年龄10~67 岁,平均(48.5±17.2)岁。受检者在临床上均无眼鼻部症状和体征,无眼鼻部手术和面部外伤病史,MRI检查眼和泪囊鼻泪管无异常发现。其中正常人4例,临床诊断需要头颅部位MRI平扫和增强检查的病人19例;首先满足临床诊断检查的需要,然后再进行正常泪囊鼻泪管的扫描。
1.1.2动态轴面扫描正常的泪囊和鼻泪管
共10例20侧,男8例,女2列,年龄20~40岁,平均(28.0±6.9)岁,受检者全部为作者的同事。
1.1.3 静态扫描有阻塞的泪囊和鼻泪管
共9例10侧;男3例,女6例,年龄33~64岁,平均(42.3±14.1)岁。泪溢病史3个月至10年;其中双侧梗阻1例,单侧梗阻8例。原发性获得性梗阻8例8侧,放射治疗后梗阻1例2侧。检查当日,不进行泪道冲洗,以免注入空气,产生伪影。通过泪道冲洗和MRI检查确定的泪囊前梗阻,未纳入本次研究。
1.2检查方法
1.2.1一般方法
与受检者本人或监护人签署相关检查知情同意书。用GE 1.5 T Signa Infinity 磁共振仪,标准正交头部线圈。增强扫描对比剂用钆喷酸葡胺注射液,用量0.2 ml/Kg体重,前臂静脉注射后1~10 min内扫描。在MRI机配套的工作站或GE AW4.5 工作站上进行图像观察和后处理。
1.2.2静态扫描
扫描时被检查者仰卧、闭眼,尽量减少眼球运动,保持平稳呼吸,防止头颅运动。用重T2WI和增强T1WI序列,序列转换期间可以瞬目。
1.2.3动态轴面扫描
被检查者仰卧,扫描期间严格要求闭眼;用轴面重T2WI脂肪抑制序列,不停歇连续扫描4遍,每遍扫描时间4 min 15 s,共17 min。
1.2.4扫描范围、扫描平面和扫描序列参数
扫描范围包括全部泪道系统。轴面扫描,扫描平面平行于眼眶下缘;冠状面扫描,扫描平面是前鼻棘前缘与额结节连线夹角9°的平面,并参考轴面上显示的泪囊和鼻泪管的位置定位。(1)轴面重T2WI脂肪抑制序列(FRFSE-XL):TR 5100.0 ms,TE 120.0 ms,层厚1.6 mm,层间隔0 mm,矩阵 288×224,FOV 180 mm×160 mm;扫描层数34 层,扫描时间4 min 15 s。(2)冠状面重T2WI脂肪抑制序列(FSE-XL):TR 4200.0 ms,TE 150.0 ms,层厚1.6 mm,层间隔0 mm,矩阵320×256,FOV 180 mm×150 mm;扫描层数9层,扫描时间2 min 52 s。(3)增强T1WI脂肪抑制序列(FSE-XL ):TR 450.0 ms,TE 最小,轴面层厚1.8 mm,冠状面层厚1.2 mm,层间隔0 mm;矩阵 288×224,FOV 180 mm×150 mm;扫描层数:轴面24 层,冠状面12层,扫描时间:轴面5 min 46 s,冠状面 2 min 53 s。
1.2.5图像质量评估标准
分为优秀、中等和差三个等级,由2名高年资MRI室医师共同进行,达成一致意见。优秀指图像无明显伪影,泪囊鼻泪管边缘清晰锐利,管壁与管腔内容物(泪液、气体、泪膜等)分界清晰明确;或在重T2WI上,泪囊鼻泪管的部分层面显现3层信号结构(图1~4)。中等指图像有伪影,泪囊鼻泪管边缘稍显毛糙,泪囊鼻泪管的整体形态和管腔的观察不受影响,管壁与管腔内液(气)体分界清晰。差指图像伪影多,不能分辨泪囊鼻泪管边缘、以及管壁与管腔内容物,影响对泪囊鼻泪管整体形态观察。

表1 静态扫描正常泪囊鼻泪管图像质量统计Tab.1 Quality grades of static MRI of the normal lacrimal sac and nasolacrimal duct
2 结果
2.1正常泪囊鼻泪管
2.1.1静态扫描序列分布和图像质量结果
在23 例46侧正常泪囊鼻泪管中,同时进行了重T2WI和增强T1WI两个序列、轴面和冠状面两个方位的受检者12例24侧。同时进行了重T2WI和增强T1WI两个序列、只有轴面一个方位的受检者3例6侧。单纯进行了重T2WI轴面和冠状面两个方位的受检者4例8侧。单纯进行了增强T1WI轴面和冠状面两个方位的受检者4例8侧。图像质量统计结果见表1。
图像质量优秀比例:重T2WI轴面图像94.7% (36/38侧),重T2WI冠状面图像31.2% (10/32侧),增强T1WI轴面图像100% (38/38侧),增强T1WI冠状面图像78.1% (25/32侧);图像质量不佳的主要原因是头颅、眼球和鼻翼的运动,以及管腔内空气造成的伪影。
2.1.2静态扫描时泪囊和鼻泪管的形态和管腔表现
泪囊鼻泪管从前上内逐渐向后下外下走行,在冠状面和矢状面上二者不完全处在同一平面,管径也不相同,因此只在少数冠状层面能显示泪囊鼻泪管全程。Hasner瓣下缘呈内高外低的弧形,但一部分人缺失(11侧)。 横断面的形态:泪囊呈长椭圆形(16侧)或裂隙状(30侧),移行部全部呈半月形(后外侧的压迹所致),鼻泪管呈短椭圆形(28侧)或类圆形(18侧)。
通过管腔内的泪膜、泪液和空气,可判断管腔的大小和形态、黏膜厚度、泪道海绵体的机能状态(萎陷和充盈);如果管腔内没有泪液和空气,只有泪膜,管腔则处于闭合状态。泪囊鼻泪管管腔狭小,形态和大小在不同的层面完全不同,管腔可呈偏心性或不规则花瓣形,表明黏膜的厚度在各个平面、在每个平面的不同方位有较大变化;泪囊黏膜厚度明显小于鼻泪管;泪囊腔全程充盈泪液的情况常见(24侧),而鼻泪管仅见斑点状泪液分布,因此可以说泪囊的管腔相对大于鼻泪管;泪囊腔虽然可以全程充盈泪液,但不饱满,甚至可以用“瘪陷”来描述(图3)。泪囊、移行部和鼻泪管可见全程充盈空气的情形(10侧)。

图1 女,58岁,正常的双侧鼻泪管下段横断面(箭),上图和下图是相同层面。上图,重T2WI。 右侧有3层信号,从内到外,高信号的是泪液,低信号的是管壁内侧部分,稍高信号的是管壁外侧部分。左侧有2层信号,最低信号的是腔内空气,稍高信号是管壁。下图,增强T1WI。双侧均呈现2层信号,右侧中心低信号是泪液,左侧中心最低信号是空气,双侧管壁呈高信号 图2 男,19岁,正常的双侧泪囊下部横断面(箭),重T2WI,腔内有较多泪液。从内到外呈现典型的高信号-低信号-稍高信号3层信号分布。注意:泪液中心的稍低信号区域,是伪影 图3 女,23岁,正常的双侧泪囊鼻泪管(箭)冠状面,重T2WI。双侧泪囊和鼻泪管均可见不对称、不规则分布的花纹状3层信号:高信号的是泪液,低信号的是管壁内侧部分,稍高信号的是管壁外侧部分;呈现了典型的管腔形态多变和狭小的特点;泪囊腔内泪液相对多于鼻泪管。右侧内眦静脉显示(箭头) 图4 女,40岁,正常的双侧鼻泪管下段(箭)轴面动态扫描,重T2WI。在正常生理状态下的连续4期同层面扫描,每期耗时4 min 15 s。泪液呈高信号,泪膜呈中等信号。管壁内1/4呈低信号,管壁外3/4呈中等信号。右侧管腔由大变小,左侧管腔几乎无变化Fig.1 A 58-year-old female normal subject.The axial plane sections of the lower parts of the nasolacrimal duct (NLD) (arrows).The upper figure is at the same level as the lower one.The upper figure, heavily-T2 weighted image (h-T2WI), reveals three layer signals on the right NLD and two layer signals on the left NLD respectively.On the right side, the hyper-intense signal represents the tear, the hypo-intense signal represents the medial part of its wall and the middle-intense signal represents the lateral part of its wall.On the left side, the hypo-intense signal represents air, and the middle-intense signal represents its wall.The lower figure, contrast-enhanced T1 weighted image (Ce-T1WI), reveals two layer signals on both sides.On the right side, the hypo-intense signal represents the tear, the hyper-intense signal represents its wall.On the left side, the hypo-intense signal represents air, and the hyper-intense signal represents its wall.Fig.2 A 19-year-old male normal subject.h-T2WI.The axial plane sections of the lower parts of the lacrimal sac (LS) (arrows).Typical three layer signals are exhibited on both sides.They are the hyper-intense signal (tear), hypo-intense signal (the medial wall) and middle-intense signal (the lateral wall) from center to outside.Notes: the hypo-intense signal in the center of the tear are the artifact.Fig.3 A 23-year-old female normal subject.The coronal plane sections of LS-NLD (arrows), h-T2WI, reveals three layer signals on both sides.But these signals are asymmetry, irregular and decorative patterns that indicate their lumen features shch as narrow, small and various shapes at different levels of LS-NLD.The hyper-intense signal represents the tear, the hypo-intense signal represents the medial part of their wall and the middle-intense signal represents the lateral part of their wall.There is relatively more tear in LS than in NLD.Right venae angularis is revealed (arrowhead).Fig.4 A 40-year-old female normal subject.Dynamic axial h-T2WI.Cross sections through the bilateral lower part of NLD (arrows).They are acquired at the same level in four phases (every phase taking 4 minutes 15 seconds) under normal physiological coditon.The tear gives the most hyper-intense signal, the tear film gives a middle-intense signal; the medial part of their wall gives a hypo-intense signal, the lateral part of their wall gives a middle-intense signal.Size of the right lumen shows a distinct change (getting smaller), but the left remains almost unchanged.
2.1.3动态扫描时泪囊鼻泪管的管腔变化
在轴面动态重T2WI脂肪抑制序列图上,比对层面相同、扫描时相不同的4幅图像。如果泪液(或空气)明显增多或变少、出现或消失,就视为管腔有明显变化,否则为管腔无变化(图4)。总共扫描10例20侧,图像质量全部优秀;其中5例8侧泪囊鼻泪管完全充气,管腔宽大直通。自下而上,将泪囊鼻泪管分为4个区段,Hasner瓣段、鼻泪管段、移行部段和泪囊段,分别统计每个区段内管腔变化的发生率(有变化的层面数量/总层面数量),结果依次为:11.9% (5/42层)、22.4% (28/125 层)、14.2% (6/42层)和12.0% (13/108层)。
2.1.4泪囊和鼻泪管的信号表现(图1~4)
在重T2WI序列上,从泪囊鼻泪管断面的中心向外,常常依次可见最高(最低,或稍高)信号-低信号-较高信号3层信号分布;中心信号代表管腔内容物(泪液,空气,或泪膜),最外2层信号代表管壁。但在泪囊和含气较多的鼻泪管断面,从中心向外,常仅显示2层信号,即最高(最低)信号-稍高信号,分别代表管腔内容物(泪液,或空气)和管壁;在静态重T2WI轴面和冠状面图像上,分别有94.7% (36/38侧)和31.2% (10/32侧)的泪囊鼻泪管的许多层面清晰显示了3层信号结构。在脂肪抑制增强轴面T1WI序列上,绝大多数(43侧)泪囊鼻泪管仅显示2层信号,即低信号-高信号2层,分别代表管腔内容物和管壁;偶尔可见3层信号分布(3侧)。
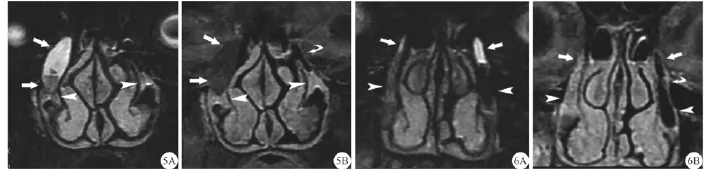
2.2有阻塞的泪囊鼻泪管(图5,6)
全部进行了静态重T2WI和增强T1WI两个序列、轴面和冠状面两个方位的扫描;图像质量全部优秀。全部病例精确显示了泪囊、鼻泪管及其阻塞部位、梗阻段长度和和其他细节。在9 例10侧病变中,移行部梗阻7侧,鼻泪管下端(Hasner瓣区域)梗阻3侧;管腔狭窄1侧,闭塞9侧。
梗阻点以上泪囊鼻泪管的表现:管腔积液(脓),管腔扩大,管壁变薄,管壁在重T2WI上只呈现单一信号;积液扩张的管腔内信号随内容物性质变化,可以是水样高信号(6侧)、高-低混杂信号或与管壁一样的稍高信号(4侧);特别要注意的是,在积液较多时,液体中心会形成低信号伪影(图2,6A)。在增强T1WI上,管腔内信号也随内容物性质变化,(与同层面肌肉比)呈现不同形态的低、等、高信号;管壁可以明显强化(8侧)或强化不明显(2侧)。
梗阻部位的表现:管腔消失或明显狭小;在重T2WI序列上丧失3层信号结构;在重T2WI和增强T1WI上,局部信号与正常管壁相同或稍低。每个梗阻点各有其形态特点,总体上分为狭窄(1侧)和闭塞(9侧)二类;梗阻点以下管腔内有空气时(1侧),狭窄表现为局部管壁梭形增厚,呈“沙漏”样(图6B);闭塞的表现是管腔的中断(图5B)。如果梗阻点(非Hasner瓣区域)以下是正常的、不含气体的泪囊或鼻泪管(6侧),病变段局部与正常段的信号可能相同,此时,病变段特点是丧失3层信号结构,并且在连续的横断面上显示更佳。
梗阻点(非Hasner瓣区域)以下的表现(6侧):它属于正常,在重T2WI序列上显示3层信号结构;如果腔内没有空气或液体时,管腔内仅有高信号的泪膜。
3 讨论
3.1泪囊鼻泪管的解剖组织学结构为MR成像提供了天然对比度
正常生理状态下,泪囊鼻泪管的解剖行经周围有筋膜、眶脂体和骨质,管腔内有泪膜、泪液或空气[10-11],这种管腔内、管壁和管壁周围不同的组织成分,为泪囊鼻泪管管壁在MRI上的显现提供了天然对比,而管腔内容物的多寡则代表了管腔的大小和形态及开放与关闭状态。
泪囊鼻泪管管壁是由上皮层和固有层构成的黏膜组织;上皮层有2层上皮细胞;在上皮之下,固有层内包埋着极端丰富的、被特异化的血管丛,即泪道海绵体[10,12-13]。泪道海绵体的基本血运有其自身特点:供血动脉发出的、垂直穿过固有层的分支,仅仅在上皮下面再分出表浅的连拱状分支,以供应上皮下密集的毛细血管网;紧邻毛细血管网的是收集它们血液的、短小的毛细血管后微静脉(postcapillary venule),而毛细血管后微静脉的血液又导入再靠外围的、管腔宽大、走行盘曲的静脉腔隙(venous lacunae);这些静脉腔隙最终引流到骨内、或靠近骨的静脉[10]。
观察光学显微镜下泪囊鼻泪管横断面的表现[10, 12-13],笔者发现小于管壁厚度1/4的内侧部分,由上皮层和包埋有毛细血管层和毛细血管后微静脉层的固有层构成,由于血管管腔所占面积相对小,所以显得较为致密;大于管壁厚度3/4的外侧部分,由包埋有静脉腔隙层的固有层构成,由于血管管腔所占面积相对大,所以显得较为疏松。这种结构,又奠定了MRI上管壁呈现不同信号层次的基础。
3.2重T2WI和增强T1WI
静态重T2WI和增强T1WI可显示正常泪囊鼻泪管的管腔、管壁层次和周围组织;动态轴面重T2WI可以显示正常泪囊鼻泪管管腔的动态变化。
MRI虽然具有良好的软组织分辨能力,但在常规T2WI或常规T2WI脂肪抑制序列上,当泪囊鼻泪管管腔内泪液较少,或仅有泪膜时,管腔与管壁信号近似,管壁常常呈现同一种信号;在水成像序列上[1-2, 4-7, 9],管腔内的液体呈明显高信号,而管壁呈现极低信号,管壁不能显示。
与常规T2WI相比,本研究中,T2WI序列应用了较长的TR和较长的TE,即TR和TE比常规T2WI序列长,比水成像序列短,因此也称之为重T2WI;该重T2WI脂肪抑制序列,秉承了常规T2WI和水成像序列的优点,即使非常少量的泪液也能在该序列上保持明显的高信号,泪膜呈高信号,同时增加了管腔内的泪液(或泪膜)、管壁内侧1/4、管壁外侧3/4和周围组织之间的对比,具体表现为:腔内容物、管壁内侧1/4、管壁外侧3/4和管壁周围组织呈现不同的信号,即泪囊鼻泪管呈现3层信号(图1~4)。
通过比对泪囊鼻泪管在光镜下的横断面组织结构[10, 12-13]与重T2WI的横断面信号表现,发现管壁的组织结构分层与MRI信号分层相吻合:管壁的内侧1/4厚度,虽然由上皮层、毛细血管层和毛细血管后微静脉层构成[10],但只呈现一种信号(即低信号),与此区域组织成分分布较密集有关;管壁外侧3/4厚度的静脉腔隙层,呈现另外一种信号(即较高信号),而与此处组织结构疏松含有大量血管有关。
在脂肪抑制增强T1WI序列上,因为泪囊鼻泪管的管壁富有血管,可以明显被强化,常常只呈现一种信号(即高信号);管腔内容物则保持平扫时原有的低信号。
动态轴面重T2WI扫描,虽然可以显示管腔的动态变化,但因为每个扫描期相的时间较长,不利于观察管腔的快速变化。动态扫描中发现的管腔大小的自主性变化,从另一方面印证了静态扫描发现的泪囊鼻泪管的管腔形态和大小在不同的平面的变化,就是黏膜厚度动态变化的结果。
需要解释的是:在重T2WI上,占管壁厚度约1/4的内侧低信号层,它的厚度比例并非恒定,因为在正常生理状态下,泪道海绵体静脉腔隙(容受静脉)的萎陷可致管壁变薄,反之,静脉腔隙的充盈可致管壁增厚[10]。增强T1WI上,管壁强化常不均匀,可见小点状明显强化区域,其与重T2WI上的局限性高信号一致,应该是反映了局部有开放的较大血管腔隙,而信号相对低的区域血管腔隙可能呈萎陷状态。
本研究中使用的方法,及其观察到的正常泪囊鼻泪管的静态和动态MRI表现,可能为某些疾病的早期诊断,如原发性获得性泪囊鼻泪管梗阻的早期诊断,找到了有效的检查方法和建立了参照基础;也可能为泪囊鼻泪管的生理解剖学研究提供了新的手段,特别是在闭眼状态下,动态扫描观察到的管腔的自主性变化,可能有助于理解泪囊鼻泪管在传输泪液过程中的生理功能。
3.3静态重T2WI和增强T1WI序列组合可显示阻塞泪囊鼻泪管的全程和病变的细节
本组检查有梗阻的泪囊鼻泪管数量不多,仅有10侧,但均明确显示了梗阻部位、病变累及的长度,还能区分管腔狭窄与闭塞。因为梗阻近段管腔内容物成分复杂,平扫时其信号与正常或异常的管壁可能相近,这两种序列的联合应用,可鉴别无血供、少血供、富血供的组织和成分;在两种序列上,梗阻处病变段的信号与正常管壁信号可能相同,为了判断梗阻段的长度,需要冠状面与轴面结合,并借助如下征象:梗阻近段管腔扩张、管壁变薄;梗阻远段尚属于正常,在重T2WI上有3层信号分布,管腔内可能只有泪膜信号而无泪液信号;梗阻段管腔消失,在重T2WI上3层信号消失,只呈现一种信号。
本组病例,根据其临床病史,梗阻部位无疑是包括了肉芽组织和瘢痕组织的慢性炎性改变;如果是其他病因所致的梗阻,如肿瘤、外伤等,局部形态表现和信号改变有待于进一步观察。泪道阻塞是常见病,治疗方法很多,但远期疗效均不太理想,原因之一是对早期病灶和病灶的治疗(手术)前评估达不到精准;用重T2WI结合增强T1WI的扫描,可以非常准确的显示位于泪囊鼻泪管中的病灶部位和范围,这是其他检查无可比拟的,为选用损伤小、疗效好而且持久的治疗方法,提供了可靠的信息。
3.4图像伪影的抑制和MRI序列参数的优化
从本组的观察结果来看,影响图像质量的主要因素是运动伪影和管腔内、鼻腔内、鼻窦内的空气造成的磁化率伪影,通过固定头部、与被检者良好的沟通、最大可能地消除对噪声的恐惧和在磁体内的幽闭恐惧,可以基本消除运动伪影。本研究中所选用的扫描参数,兼顾了层厚、视野、信噪比、采集时间等;层厚越薄,部分容积效应越小,组织分辨率越高,扫描层数增加,扫描时间增加,信噪比降低;层厚越厚,则正好相反。不同的MRI设备,扫描参数应该还可以进一步优化,采集时间应该可以进一步缩短[14]。但要注意识别MRI图像上的各种伪影和其他正常结构,如内眦静脉和鼻窦黏膜等(图3)。
3.5结论
总之,在脂肪抑制技术基础之上,重T2WI结合增强T1WI,轴面图像结合冠状面图像,再结合动态重T2WI扫描,可以清晰的显示正常生理状态下的泪囊鼻泪管的管腔、管腔内容物性质、管壁结构层次和行经,及其管腔的动态变化;可以显示有阻塞的泪囊鼻泪管的全程和病变部位的细节;增强扫描有助于区别阻塞点无血液供应的管腔内沉积物与有血液供应的管壁、肉芽组织等。这种MRI序列组合,可实现各种泪囊鼻泪管影像学检查的目标,因此有望替代它们,其中包括泪道逆行插管造影术[15];遗憾的是该检查不能显示正常的泪小管和泪总管。
参考文献[References]
[1]Wang Y, Zhou J, Chen LL, et al.Clinical application value of MR dacryocystography using 3D FIESTA to analyze the cause of epiphora.J Chin Clin Med Imaging, 2015, 26(2): 77–80.
王悦, 周军,陈琳琳,等.磁共振成像技术3D FIESTA序列对溢泪病因分析的临床应用价值.中国临床医学影像杂志, 2015, 26(2): 77–80.
[2]Jing Z, Lang C, Qiu-Xia W, et al.High-spatial-resolution isotropic three-dimensional fast-recovery fast spin-echo magnetic resonance dacryocystography combined with topical administration of sterile saline solution.Eur J Radiol, 2013, 82(9): 1546–1551.
[3]Coskun B, Ilgit E, Onal B, et al.MR dacryocystography in the evaluation of patients with obstructive epiphora treated by means of interventional radiologic procedures.Am J Neuroradiol, 2012, 33(1): 141–147.
[4]Cubuk R, Tasali N, Aydin S, et al.Dynamic MR dacryocystography in patients with epiphora.Eur J Radiol, 2010, 73(2): 230–233.
[5]Detorakis ET, Drakonaki E, Papadaki E, et al.Watery eye following patent external DCR: an MR dacryocystography study.Orbit, 2010, 29(5): 239–243.
[6]Zhang J, Shu HG, Hu JW et al.Nasolacrimal duct imaging using MR hydrography and its clinical application.Chin J Radiol, 2008, 42(6): 614–617.
张菁, 舒红格, 胡军武, 等.MR鼻泪管成像的临床应用.中华放射学杂志, 2008, 42(6): 614–617.
[7]Amrith S, Goh PS, Wang SC.Tear flow dynamics in the human nasolacrimal ducts: a pilot study using dynamic magnetic resonance imaging.Graefes Arch Clin Exp Ophthalmol, 2005, 243(2): 127–131.
[8]Manfrè L, de Maria M, Todaro E, et al.MR dacryocystography: comparison with dacryocystography and CT dacryocystography.Am J Neuroradiol, 2000, 21(6): 1145–1150.
[9]Takehara Y, Isoda H, Kurihashi K, et al.Dynamic MR dacryocystography: a new method for evaluating nasolacrimal duct obstructions.Am J Roentgenol, 2000, 175(2): 469–473.
[10]Paulsen FP, Thale AB, Hallmann UJ, et al.The cavernous body of the human efferent tear ducts: function in tear outflow mechanism.Invest Ophthalmol Vis Sci, 2000, 41(5): 965–970.
[11]Paulsen F.The human nasolacrimal ducts.Adv Anat Embryol Cell Biol, 2003,170(Ⅲ-Ⅺ): 1–106.
[12]Ayub M, Thale AB, Hedderich J, et al.The cavernous body of the human efferent tear ducts contributes to regulation of tear outflow.Invest Ophthalmol Vis Sci, 2003, 44(11): 4900–4907.
[13]Paulsen F, Hallmann U, Paulsen J, et al.Innervation of the cavernous body of the human efferent tear ducts and function in tear outflow mechanism.J Anat, 2000, 197(Pt 2): 177–187.
[14]Xue ZH, Wang YF, Zhao YB.Magnetic resonance imaging quality control and parameter optimization.Chin J of Magn Reson Imaging, 2013, 4(6): 441–444.
薛正和, 王永峰, 赵一冰.磁共振成像的质量控制及参数优化.磁共振成像, 2013, 4(6): 441–444.
[15]Wang TT, Tao H, Han C, et al.Preliminary study on CT retrograde intubation dacryocystography (CT-RIDC) and its impact factors.Chin J Ophthalmol, 2014, 10(50): 766–771.
王婷婷, 陶海, 韩毳, 等.CT泪道逆行插管造影检查及其影响因素的初步研究.中华眼科杂志, 2014, 10(50): 766–771.
DOI:10.12015/issn.1674-8034.2016.01.005
文献标识码:A
中图分类号:R445.2;R777.23
收稿日期:2015-09-28
通讯作者:
作者单位:
猜你喜欢
航天返回与遥感(2022年2期)2022-05-12
燃气涡轮试验与研究(2021年6期)2021-08-01
海洋信息技术与应用(2020年4期)2021-01-18
中国生物医学工程学报(2019年5期)2019-07-16
北京航空航天大学学报(2017年3期)2017-11-23
中国实用医药(2016年29期)2016-12-26
心脑血管病防治(2016年5期)2016-12-19
华夏医学(2016年4期)2016-12-12
中国实用医药(2016年28期)2016-12-07
现代电子技术(2016年15期)2016-12-01