
Development of a checklist of short-term and long-term psychological symptoms associated with ketamine use
2015-12-09 06:33:44NiFANKeXUYupingNINGDapingWANGXiaoyinKEYiDINGBinSUNChaoZHOUXuefengDENGRobertROSENHECKHongboHE
上海精神医学 2015年3期
Ni FAN, Ke XU, Yuping NING, Daping WANG, Xiaoyin KE, Yi DING, Bin SUN , Chao ZHOU,Xuefeng DENG, Robert ROSENHECK, Hongbo HE,*
•Research methods in psychiatry•
Development of a checklist of short-term and long-term psychological symptoms associated with ketamine use
Ni FAN1, Ke XU2, Yuping NING1, Daping WANG1, Xiaoyin KE1, Yi DING1, Bin SUN1, Chao ZHOU1,Xuefeng DENG3, Robert ROSENHECK2, Hongbo HE1,*
ketamine; substance-related disorders; signs and symptoms; questionnaire; factor analysis; China
1. Background
Ketamine is an N-methyl-D-aspartate (NMDA) receptor antagonist that can induce various effects including sedation, relaxation, euphoria, and hallucinations.At low doses, ketamine induces sedation and pain relief; at high doses it can induce an anesthetic dissociative state. Since ketamine was first synthesized in the 1960s, it has been widely used in anesthesia and pain management and is currently in the WHO Directory of Essential Drugs.[1]However, during recent decades ketamine has been increasingly used as a recreational drug. In China, where ketamine is referred to as ‘K-powder’, it is becoming a popular drug of abuse among illegal drug users, accounting for 21.5% of all substance abuse disorders in 2004 and 40% of all substance abuse disorders in 2009.[2-5]Studies have found that a single intravenous injection of a sub-anesthetic dose of ketamine (0.5mg/kg) in individuals with refractory depression can induce a pronounced anti-depressant effect within 1 to 2 hours that is sustained for up to one week.[6,7]Among healthy volunteers, a single intravenous injection of ketamine can induce schizophrenia-like symptoms.[8-10]Compared with the predominantly positive psychotic symptoms produced by amphetamines, ketamineinduced psychotic symptoms include positive symptoms(i.e., hallucinations and delusions), negative symptoms,and cognitive impairment.[11]Ketamine use has also been associated with cystitis and other physical problems.[12]Based on these fi ndings, some researchers have proposed using a ketamine model of schizophrenia to study the glutamate neural pathway believed to be important in schizophrenia.[13]
Despite its increasing popularity in China, there have been few reports about the effects of ketamine use among chronic ketamine users. To provide a pro file of ketamine-related symptoms in this population, we developed a preliminary 35-item symptom checklist of ketamine-related symptoms based on our clinical experience with such patients, administered it to a sample of ketamine users recruited from two hospitals in Guangzhou (a major metropolitan city in south China),and used exploratory and confirmatory factor analyses to identify the subset of items in the checklist that best represent the underlying clinical domains related to the short-term and long-term symptoms of ketamine use.
2. Methods
2.1 Recruitment
The recruitment of participants in the study is shown in Figure 1. The Department of Substance Dependence at Guangzhou Brain Hospital has 40 beds, and the Voluntary Rehabilitati on Ward of the Guangzhou Baiyun Mental Hospital has 100 beds. Two psychiatrists and a graduate student from the Guangzhou Brain Hospital recruited all participants, visiting the Baiyun Mental Hospital twice a week over the study enrollment period. They screened a convenience sample of 630 individuals with a history of ketamine use at the ti me of inpatient admission to the two participating hospitals from January 2012 to December 2013. Participants meeting the following inclusion and exclusion criteria were considered for the study: (a) receiving inpatient ketamine detoxification treatment or treatment for symptoms related to ketamine use; (b) met the DSM-IV-TR[14]diagnostic criteria for substance dependence;(c) no history of dependence on psychoactive drugs other than ketamine and tobacco; (d) other than tobacco and alcohol, did not use other drugs besides ketamine during the prior 6 months; (e) no serious physical illness; (f) had no history of a head injury that resulted in loss of consciousness; (g) no significant visual or hearing impairments; and (h) no history of other mental disorders. All eligible individuals were asked to participate in the study. Persons who signed the informed consent subsequently participated in a 2-hour interview about their current drug use patterns that included completion of a 35-item symptom checklist(described below).

Figure 1. Recruitment of participants in the study
This study was approved by the research ethics committee of the Guangzhou Brain Hospital.
2.2 Assessment
To our knowledge, there is no previous report of a scale used to assess clinical symptoms related to ketamine abuse. We constructed a preliminary 35-item symptom checklist that assess 19 acute effects of ketamine use(i.e., those that occur immediately after using ketamine)and 16 chronic symptoms that emerge aft er long-term use of ketamine (shown in Table 2). The items included in this preliminary checklist were based on a previous report that included individuals’ descriptions of their experiences related to ketamine use[15]and on our own knowledge and clinical experience with ketamine dependence. Each of the 35 items was rated on a binary scale (‘yes’ or ‘no’) based on patients’ responses to a structured interview conducted by a psychiatrist.All interviews were conducted within one week of admission. (The Chinese version of the checklist used in the study is available with the Chinese translation of this article on the website of theShanghai Archives of Psychiatry).
We also collected basic demographic information on each subject, and information about the age of onset,duration, and frequency of use of ketamine and other substances including tobacco and alcohol.
2.3 Data analysis
A total of 13 patients had incomplete data, so the analysis was based on data from 187 individuals.The results for these 187 individuals were randomly assigned to two groups using a random number table.The first group (n=94) was used for the exploratory factor analysis (EFA) and the second group (n=93) was used for the confirmatory factor analysis (n=93).
The scree plot from the initial EFA (on the first half of the sample) of all 35 items and consideration of the item loadings in different models (i.e., the 3-factor,4-factor, and 5-factor models) were used to decide on the best model to represent the results. The itemreduction process was conducted as follows. For each of the three possible models we removed items that had loadings of less than 0.30 on all factors or that had loadings of greater or equal to 0.30 on two or more factors (i.e., cross-loading). After removing these items the EFA was re-run and the loadings re-examined; if there were still items with no loadings of 0.30 or greater or items with cross-loadings they were removed and the EFA was re-run on the remaining items. This process was repeated until all remaining items had loadings of 0.30 or greater on only one factor. The three potential final models were then examined and the model in which the factors contained the most logical combination of items(symptoms) was selected as the final model.
This final model with factor-specific items was then tested using CFA based on the results of the second group of respondents. The validity of the factor structure identified in the EFA was assessed using various fit indices including the Goodness of Fit Index(GFI) and the Root Mean Square Error of Approximation(RMSEA). The internal consistency of the subscales of the final questionnaire was assessed using alpha values.SPSS 18.0 and Mplus (version 7) soft ware was used for data analyses.
3. Results
3.1 Sample characteristics
Table 1 shows the characteristics of the sample. A total of 187 individuals completed the interviews including 173 (92.5%) males and 14 (7.5%) females. Their mean(sd) age was 26.2 (5.0) years (range=15 to 44). The mean duration of ketamine use was 6.3 (3.1) years and the mean duration of ketamine dependence was 3.1 (2.0) years. Most participants were using ketamine daily prior to admission. The mean amount of ketamine used during the prior month was 3.4 (2.7) g/day. Our enrollment criteria excluded individuals who had previously been dependent on other illegal substances;nevertheless, the majority of these ketaminedependent individuals had previously used (but not been dependent on) other types of illegal psychoactive substances.
3.2 Acute and chronic symptoms of ketamine use
The reported prevalence of short-term and long-term effects of ketamine use are listed in Table 2. The most common short-term effects experienced immediately after using ketamine were ‘weightless floating or circling’ (94%), ‘euphoric when listening to rousing music’ (86%), and ‘excited, talkative, and full of energy’(67%). The most common long-term symptoms the individuals reported aft er using ketamine for more than a year were ‘memory loss’ (93%), ‘personality changes’(86%), and ‘slow reaction ti me’ (81%).
3.3 Item reduction and characteristics of the final model
As shown in Figure 2, the EFA of the initial 35 items in the first half of the sample identified 12 factors with eigenvalues >1. Based on the scree plot, we consideredthree possible models, a 3-factor model, a 4-factor model, and a 5-factor model. After completing the itemreducti on steps (described in the methods) for each of these models, the 22-item version of the 4-factor model provided the most coherent grouping of items (data provided on request), so this was selected as the final model and as the final version of the scale.
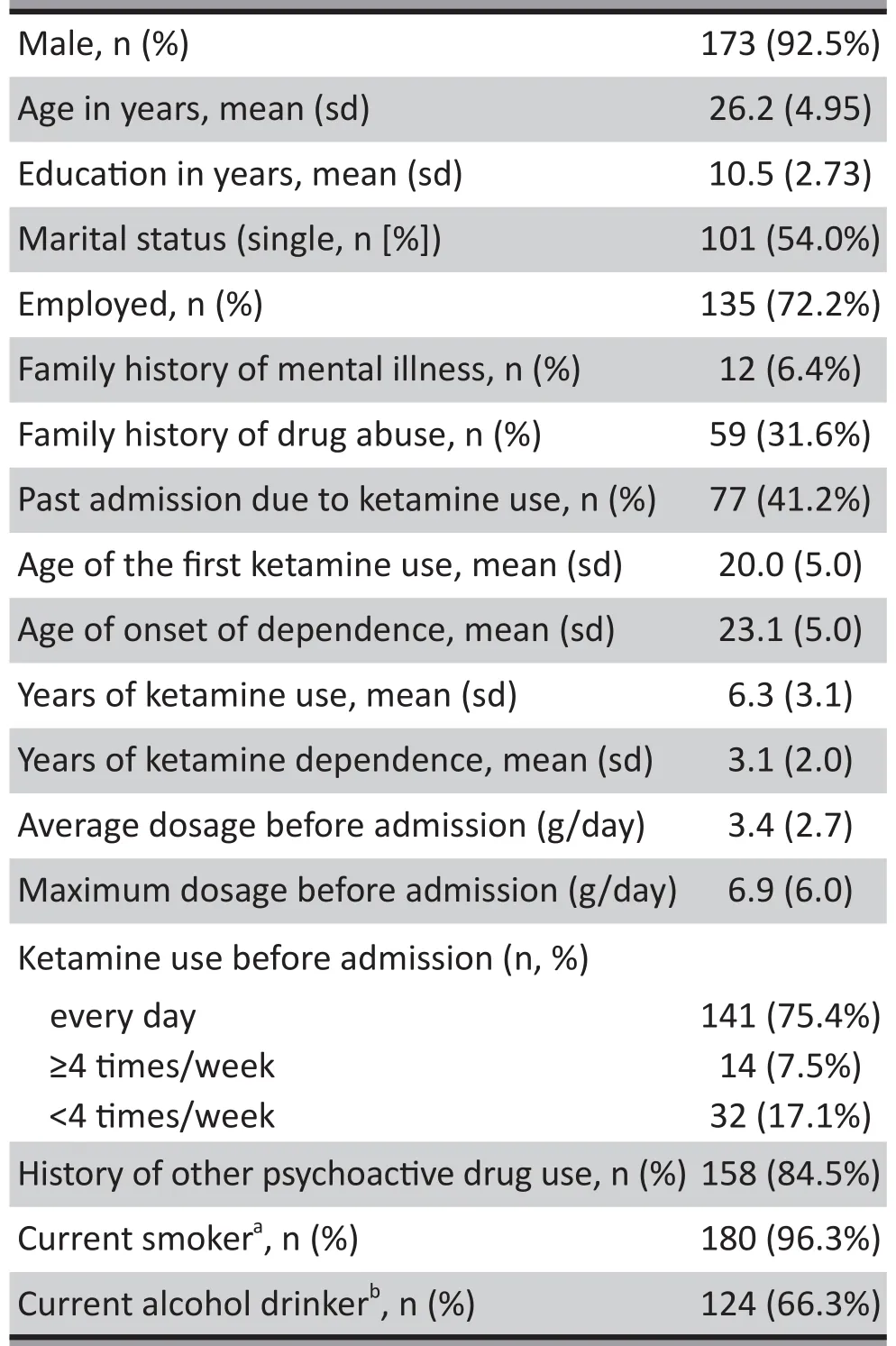
Table 1. Characteristics of the 187 participants

Figure 2. Scree plot of exploratory factor analysis of a 35-item checklist of short-term and longterm symptoms of ketamine use among 94 inpatients with ketamine dependence
The loadings of the 22 items on these 4 factors in the EFA are shown in the Table 3. In the EFA, the first factor included 5 long-term symptoms associated with social withdrawal; the second factor included 4 longterm symptoms associated with sleep disturbance;the third factor included 8 acute symptoms associated with psychotic-like experiences and irritability; and the fourth ‘other symptoms’ factor included 5 symptoms that combined long-term reports of decreased sex drive and reports of excitement and euphoria at the ti me of taking ketamine. Based on the results using the first random half of the sample, these 4-factors accounted for 49% of the variance in the 22-item scale and the internal consistency (based on Cronbach alpha) of the four factors – the subscales of the overall scale – range from 0.63 to 0.86.
3.4 Assessment of the fi nal model for the scale
The validity and robustness of this 22-item, 4-factor model of the acute and chronic symptoms of ketamine abuse identified using EFA based on the first half of the sample was assessed using CFA based on the second half of the sample. As shown in Table 3, the distributi on of items across factors and the loading of the items of the 4 factors in the CFA is very similar to that in the EFA. All the items loaded on the appropriate factors,and, with the exception of the ‘weightless floating or circling’ item, all items had loadings of 0.30 or greater on a single factor. In the CFA these 4 factors accounted for 50% of the variance. The internal consistency of the items included in the social withdrawal and sleep disturbance subscales was excellent (alpha=0.86 and 0.82, respectively), that for the psychotic-like symptoms subscale was fair (0.69), and that for the ‘other symptoms’ factor was poor (0.41). The correlation between the factors were all quite low, ranging from-0.03 to 0.28. The fi t parameters for this 4-factor model were fair (GFI=83.3%; RMSEA= 0.072, 90% confidence interval=0.062, 0.083).
4. Discussion
4.1 Main Finding
In this study, we found that among the 19 shortterm symptoms of ketamine use, the most common symptoms reported by individuals who are dependent on ketamine are a floating or circling sensation,euphoria, and excitement. Among the 16 long-term symptoms considered, the most commonly reported symptoms were memory loss, personality changes, slow reaction ti me, lethargy, and decreased libido.

Table 2. Prevalence of ketamine-related symptoms in 187 inpatients with ketamine dependence and loadings on 4-factor model in exploratory factor analysis (with varimax rotati on) in a random sample of 94 of these individuals
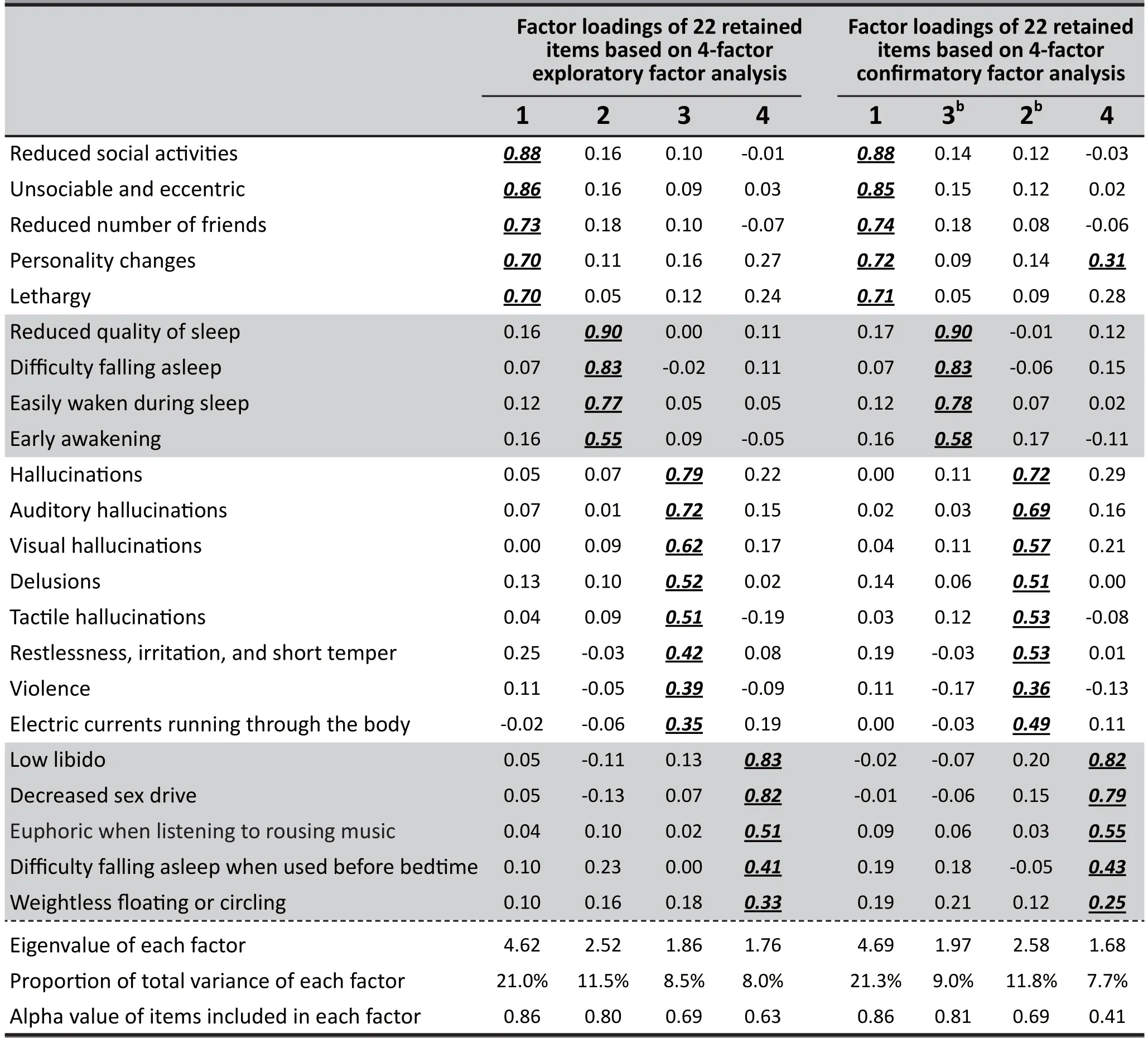
Table 3. Factor loadings (with varimax rotation) of the final 22-item, 4-factor model in the exploratory factor analysis (n-94) and the confirmatory factor analysis (n=93)a
A series of studies by Muetzelfeldt and colleagues,[15]Curran and colleagues,[16]and Morgan and colleagues,[17]used a 12-item, self-report questionnaire to ask 20 recreational ketamine users about their subjective experiences with ketamine on the night of use, 3 days later, and 3 years later. They observed a 80%drop in the amount of ketamine use (in both frequency and dosage) among these recreational users three years aft er the baseline assessment. They reported that commonly occurring short-term effects included bodily numbness, impaired concentration and memory, lack of coordinati on, unsteadiness, out of body experiences,altered perception, and altered reality; the impaired concentration and memory persisted at the 3-day and 3-year follow-up assessments. Our findings parallel these results, but in our sample of inpatients with chronic ketamine dependence (who used higher doses of ketamine for more prolonged periods than recreation users) social withdrawal and sleep disturbance were also prominent long-term symptoms.
Like ketamine use, amphetamine use has been associated with euphoria and a high prevalence of hallucinations but, somewhat unlike the symptoms of ketamine use, amphetamine use is also commonly associated with the occurrence of different types of delusions (reported in 30% to 52% of users) including erotomania, persecutory delusions, delusions of jealousy, grandiose delusions, and delusions of control.[18]Our study found delusions a relatively uncommon shortterm symptom following ketamine use, occurring in only 11% of the sample. A previous study that compared the occurrence of various psychiatric symptoms between amphetamine and ketamine users using the Brief Psychiatric Rating Scale[19]found higher levels of cognitive dysfunction, motor hyperactivity, and hostility among amphetamine users and higher levels of anxiety,depression, and motor retardation among ketamine users.
Exploratory factor analysis identified a subset of 22 items from the original pool of 35 items that segregated into four factors, representing the underlying groupings of symptoms that occur with ketamine use. The confirmatory factor analysis conducted on the second half of the sample confirmed the validity of this 22-item, 4-factor structure, but the model fit parameters(GFI=83%, RMSEA=0.072) were only fair, so further work will be needed to re fine the scale. The first three factors considered by the final version of the scale – longterm social impairment, long-term sleep disturbances,and short-term psychotic-like symptoms – appeared reasonably consistent and theoretically feasible;however, the final factor – which combines short-term euphoria and long-term deceases in sexual functioning– had poor internal consistency so it may not be a useful construct for understanding ketamine-related symptoms.
4.2 Limitations
All participants were inpatients seeking voluntary treatment for addiction, so it is uncertain whether or not the pattern of symptoms they report are similar to those of ketamine users who do not seek treatment. We tried to eliminate the effect of other psychoactive drugs by excluding patients who had used other psychoactive drugs (other than tobacco and alcohol) in the previous 6 months, but over 80% of participants reported prior use of other psychoactive drugs more than 6 months previously so we cannot be sure that all the long-term symptoms they report are actually due to ketamine use.We consulted previous reports and used our clinical experiences in the construction of the preliminary 35-item symptom checklist, but the list may have missed some relevant symptoms. Moreover, the checklist focuses on subjective feelings and mental symptoms so it does not include potentially important somatic symptoms related to ketamine use (e.g. urinary tract symptoms).[20]Conducting exploratory and confirmatory factor analysis usually requires large samples, so our sample of 187 individuals may not have been large enough to generate stable results from the factor analysis, particularly because 4 of the 35 symptoms in the preliminary scale were reported by less than 10%of respondents. Moreover, the inter-rater reliability and test-retest reliability of the symptom checklist was not assessed. Finally, it is uncertain how sensitive the symptom checklist will be to changes in the prevalence and severity of long-term symptoms of ketamine use during periods of abstinence.
4.3 Implicati ons
Despite the increasing popularity of ketamine abuse in contemporary China, the symptoms related to ketamine use are poorly understood. To the best of our knowledge, this is the first report on the pro file of short-term and long-term symptoms that are associated with ketamine use in China. We administered an initial symptom checklist with 35 items selected from reports in other countries and our own clinical experience to a large sample of individuals with ketamine dependence and used exploratory and confirmatory factor analysis to identify the 22 symptoms that best capture the shortterm and long-term clinical symptoms of ketamine abuse. These 22 key symptoms segregate into four dimensions, two sets of long-term symptoms (i.e., social withdrawal and sleep disturbance), one set of psychoticlike short-term symptoms, and one dimension that included both short-term items related to euphoria and excitement at the ti me of ketamine use and items about decreased sex drive that occurs aft er long-term use of ketamine. The first three dimensions appear reasonably robust but the last dimension is less internally consistent. Future work with this scale in larger samples is needed to confirm this 4-factor structure of ketamineuse-related symptoms, to assess the test-retest reliability of the scale, and to determine whether or not the scale can be useful in the differential diagnosis and monitoring of treatment of individuals with ketamine dependence.
Acknowledgement
The authors wish to thank all staff at the voluntary detoxification ward of Guangzhou Baiyun Hospital.
Con flict of Interest
The authors declare no conflict of interest related to this manuscript.
Funding
This study was funded by the Key Discipline Development Project (GBH2014-ZD02) and the China National Key Clinical Specialty Project to the Guangzhou Brain Hospital (201202-001) and by the Guangzhou Municipal Medical Science and Technology Fund (number: 20131A011091). Dr. He is supported by the National Natural Science Foundation of China(81371506) and by the Guangdong Province Natural Science Foundati on (S2013040012414).
Ethical approval
The study was approved by the research ethics committee of the Guangzhou Brain Hospital.
Informed consent
All participants provided written informed consent to participate in this study.
1. World Health Organizati on.18th WHO Model List of Essenti al Medicines (April 2013).Available at: http://www.who.int/medicines/publications/essentialmedicines/en/index.html
2. Lian Z, Liu RK, Mu Y, Cao JQ. [Epidemiological survey of ketamine in China].Zhongguo Yao Wu Yi Lai Xing Za Zhi. 2005; 14(4): 280-283. Chinese. doi: http://dx.doi.org/10.3969/j.issn.1007-9718.2005.04.012
3. Liu YH, Lian Z, Liu ZM. [Analysis of ketamine use in drug abusers].Zhongguo Yao Wu Yi Lai Xing Za Zhi. 2003;12(1): 52-54. Chinese. doi: http://dx.doi.org/10.3969/j.issn.1007-9718.2003.01.016
4. Chen HH, Fan CL, Du J, Sun HM, Zhao M. [DSM-IV Axls I diagnoses analysis in 506 patients with substance dependence].Zhongguo Yao Wu Yi Lai Xing Za Zhi. 2009;18(3): 200-203. Chinese
5. Wang YF, Zhang YZ, Lian Z, Sun GK, Bao YP, Liu ZM.[Epidemiological characteristics of three new drugs abuse in Beijing].Zhongguo Yao Wu Yi Lai Xing Za Zhi.2008; 17(6):445-454, 459. Chinese
6. Zarate CA Jr, Singh JB, Carlson PJ, Brutsche NE, Ameli R,Luckenbaugh DA, et al. A randomized trial of an N-methyl-D-aspartate antagonist in treatment-resistant major depression.Arch Gen Psychiatry. 2006; 63(8): 856-864. doi:http://dx.doi.org/10.1001/archpsyc.63.8.856
7. aan het Rot M, Collins KA, Murrough JW, Perez AM, Reich DL, Charney DS, et al. Safety and efficacy of repeated-dose intravenous ketamine for treatment-resistant depression.Biol Psychiatry. 2010; 67(2): 139-145. doi: http://dx.doi.org/10.1016/j.biopsych.2009.08.038
8. Krystal JH, Karper LP, Seibyl JP, Freeman GK, Delaney R, Bremner JD, et al. Subanesthetic effects of the noncompetitive NMDA antagonist, ketamine, in humans.Psychotomimeti c, perceptual, cognitive, and neuroendocrine responses.Arch Gen Psychiatry. 1994; 51(3): 199-214. doi:http://dx.doi.org/10.1001/archpsyc.1994.03950030035004
9. Becker A, Peters B, Schroeder H, Mann T, Huether G,Grecksch G. Ketamine-induced changes in rat behaviour:A possible animal model of schizophrenia.Prog Neuropsychopharmacol Biol Psychiatry. 2003; 27(4): 687-700. doi: http://dx.doi.org/10.1016/S0278-5846(03)00080-0
10. Aalto S, Ihalainen J, Hirvonen J, Kajander J, Scheinin H,Tanila H, et al. Cortical glutamate-dopamine interaction and ketamine-induced psychotic symptoms in man.Psychopharmacology (Berl). 2005; 182(3): 375-383. doi:http://dx.doi.org/10.1007/s00213-005-0092-6
11. Morgan CJ, Riccelli M, Maitland CH, Curran HV. Long-term effects of ketamine: evidence for a persisting impairment of source memory in recreati onal users.Drug Alcohol Depend.2004; 75(3): 301-308. doi: http://dx.doi.org/10.1016/j.drugalcdep.2004.03.006
12. Wu P, Zhu XQ, Yao MG. [“Street ketamine” associated urinary system dysfunction].Zhonghua Mi Niao Wai Ke Za Zhi. 2008; 29(7): 489-492. Chinese. doi: http://dx.doi.org/10.3321/j.issn:1000-6702.2008.07.018
13. Moore JW, Turner DC, Corlett PR, Arana FS, Morgan HL,Absalom AR, et al. Ketamine administration in healthy volunteers reproduces aberrant agency experiences associated with schizophrenia.Cogn Neuropsychiatry. 2011;16(4): 364-381. doi: http://dx.doi.org/10.1080/13546805.201 0.546074
14. American Psychiatric Associati on.Diagnostic and statistical Manual of Mental Disorders,4th ed. Text Revision.Washington: American Psychiatric Associati on; 1994
15. Muetzelfeldt L, Kamboj SK, Rees H, Taylor J, Morgan CJ,Curran HV. Journey through the K-hole: phenomenological aspects of ketamine use.Drug Alcohol Depend.2008; 95(3): 219-329. doi: http://dx.doi.org/10.1016/j.drugalcdep.2008.01.024
16. Curran HV, Morgan C. Cognitive, dissociative and psychotogenic effects of ketamine in recreational users on the night of drug use and 3 days later.Addicti on. 2000;95(4): 575-590. doi: http://dx.doi.org/10.1046/j.1360-0443.2000.9545759.x
17. Morgan CJ, Monaghan L, Curran HV. Beyond the K-hole:a 3-year longitudinal investigation of the cognitive and subjective effects of ketamine in recreational users who have substanti ally reduced their use of the drug.Addicti on.2004; 99(11): 1450-1461. doi: http://dx.doi.org/10.1111/j.1360-0443.2004.00879.x
18. Zhao Y, Jiang HF, Du J, Ren QH, Li X, Jiang WW, et al. [Clinical characteristics and risk factors of amphetamine-type stimulant- induced psychosis].Zhongguo Yao Wu Yi Lai Xing Za Zhi. 2014; 23(3): 201-205. Chinese
19. Zhang S, Xu ZF, Chen HJ, Yang W, Jiang T, Zhang Y. [Comparison of psychiatric symptoms among inpatients who used amphetamine tape stimulants, ketamine or mixed of them].Zhongguo Yao Wu Yi Lai Xing Za Zhi.2014; 23(04): 281-286.Chinese
20. Wang YX, Liu CX, Jiang CL, Xie XP. [The clinical survey and synthetical therapy of ketamine-associated cystitis].Chongqing Yi Xue. 2013; 32: 3911-3912, 3915. Chinese. doi:http://dx.doi.org/10.3969/j.issn.1671-8348.2013.32.024
, 2014-10-16; accepted, 2015-04-13)

Dr. Fan obtained her bachelor’s degree from Chongqing Medical College in 1997, her master’s degree in Neuropsychology from Jinan University (Guangdong) in 2003, her Ph.D. from Louisiana State University(USA) in 2009, and post-doctoral training at Yale University from 2009 until 2012. She then joined Guangzhou Brain Hospital where she is currently an associate professor and the deputy director of the Institute of Psychiatry and Neuroscience. Her main research interest is the mechanisms of ketamine dependence.
与氯胺酮滥用相关的短期和长期心理症状清单的编制
范妮,许柯,宁玉萍,王达平,柯晓殷,丁毅,孙彬,周超,邓雪峰,Rosenheck R,何红波
氯胺酮;物质相关障碍;体征和症状;因子分析;中国
Background: Ketamine is an increasingly popular drug of abuse in China but there is currently no method for classifying the psychological effects of ketamine in individuals with ketamine dependence.Aims: Develop a scale that characterizes the acute and long-term psychological effects of ketamine use among persons with ketamine dependence.Methods: We developed a preliminary symptom checklist with 35 dichotomous (‘yes’ or ‘no’) items about subjective feelings immediately after ketamine use and about perceived long-term effects of ketamine use that was administered to 187 inpatients with ketamine dependence recruited from two large hospitals in Guangzhou, China. Exploratory factor analysis (EFA) was conducted on a randomly selected half of the sample to reduce the items and to identify underlying constructs. Confirmatory factor analysis (CFA) was conducted on the second half of the sample to assess the robustness of the identified factor structure.Results: Among the 35 symptoms, the most-reported acute effects were ‘ floating or circling’ (94%), ‘euphoric when listening to rousing music’ (86%), and ‘feeling excited, talkative, and full of energy’ (67%). The mostreported long-term symptoms were ‘memory impairment’ (93%), ‘personality changes’ (86%), and ‘slowed reactions’ (81%). EFA resulted in a final 22-item scale best modelled by a four-factor model: two factors representing chronic symptoms (social withdrawal and sleep disturbances), one about acute psychoticlike symptoms, and one that combined acute drug-related euphoria and longer-term decreased libido.CFA showed that these 4 factors accounted for 50% of the total variance of the final 22-item scale and that the model fit was fair (Goodness of Fit Index, GIF=83.3%; Root Mean Square Error of Approximati on,RMSEA=0.072).Conclusions: A four-factor model including social withdrawal, sleep disturbance, psychotic-like symptoms,and euphoria at the time of drug use provides a fair description of the short-term and long-term psychological symptoms associated with ketamine use. Future work on the 22-item version of the scale with larger samples is needed to con fi rm the validity of this 4-factor structure, to assess the scale’s test-retest reliability, and to determine whether or not it can be useful in the diff erenti al diagnosis and monitoring of treatment of individuals with ketamine dependence.
[Shanghai Arch Psychiatry. 2015; 27(3): 186-194. Epub 2015 Apr 29.
http://dx.doi.org/10.11919/j.issn.1002-0829.214158]
1Guangzhou Brain Hospital (Guangzhou Hui Ai Hospital), Guangzhou Medical University, Guangzhou, Guangdong Province, China
2Department of Psychiatry, Yale University School of Medicine, New Haven, CT, United States
3Guangzhou Baiyun Voluntary Drug Rehabilitati on Hospital, Guangzhou, Guangdong, China
*correspondence: vglut2@126.com
背景:氯胺酮滥用在中国日渐增多,但目前还没有一个方法可以将氯胺酮对依赖个体的心理影响作用进行分类。目的:编制能反映氯胺酮依赖人群中因该物质滥用所致的急性心理影响和长期心理影响的量表。方法:我们编制了一个初步的症状清单,共有35个条目(“是”或“否”的二分法问题),内容是关于使用氯胺酮后即刻产生的主观感受以及氯胺酮滥用后感受到的长期作用。从中国广州市两个大医院招募氯胺酮依赖住院患者,共入组187例。随机选择一半的样本进行探索性因子分析(exploratory factor analysis,EFA),以精简条目并确定量表的基本结构。对另一半样本进行验证性因子分析(confirmatory factor analysis,CFA),以评估所提取因子结构的稳健性。结果:35个症状中常见的急性期症状是“身体的漂浮或盘旋感”(94%)、“在动感音乐的环境下心情更加舒畅、欣快感”(86%)、和“兴奋话多,精力充沛”(67%)。常见的慢性症状是“记忆力下降”(93%)、“性格变化”(86%)和“反应变慢”(81%)。探索性因子分析最终得到的最佳模型量表,共22个条目,构成四个因子:两个因子代表慢性症状(社交退缩和睡眠障碍),一个因子是关于急性精神病样症状的,而第四个因子整合了急性的药物所致的欣快感和长期的性欲下降。验证性因素分析显示这4个因子能解释最终22个条目量表总方差的50%,并且模型拟合良好(拟合指数,GFI=83.3%;近似误差均方根,RMSEA=0.072)。结论:四因子模型(社交退缩、睡眠障碍、精神病样症状和使用毒品时的欣快感)能较为客观地反映氯胺酮滥用相关的短期和长期心理症状。对这一22个条目的量表,今后的研究工作需要扩大样本量,以验证实该四因子结构的效度,评估量表的重测信度,并确定是否能将该量表用于氯胺酮依赖的鉴别诊断和治疗监测。
本文全文中文版从2015年8月6日起在http://dx.doi.org/10.11919/j.issn.1002-0829.214158 可供免费阅览下载
猜你喜欢
中学生数理化(高中版.高考数学)(2022年2期)2022-04-26 14:04:58
中学生数理化(高中版.高考数学)(2020年3期)2020-05-25 06:53:16
中国神经精神疾病杂志(2020年9期)2020-01-14 19:02:12
神州·下旬刊(2019年1期)2019-02-11 06:03:50
中国神经再生研究(英文版)(2017年10期)2017-11-08 11:48:42
课程教育研究·学法教法研究(2016年33期)2017-03-30 18:37:48
西南军医(2016年3期)2016-01-23 02:17:58
中国继续医学教育(2015年6期)2016-01-07 07:38:47
新高考·高二数学(2014年5期)2014-09-12 01:20:19
同位素(2014年2期)2014-04-16 04:57:16

- 上海精神医学的其它文章
- Meta-analysis for psychiatric research using free soft ware R
- Oligodendroglioma presenti ng as chronic mania
- Comparisons of family environment between homeless and non-homeless individuals with schizophrenia in Xiangtan, Hunan
- Abnormal inter- and intra-hemispheric integrati on in male paranoid schizophrenia: a graph-theoreti cal analysis
- Metacognitive training for schizophrenia: a systematic review
- Addressing risk of bias in trials of cognitive behavioral therapy