
C型臂X光机引导穿刺联合神经电生理分支定位技术在三叉神经半月节射频热凝术中的应用价值
2015-09-14 02:56李艳左欣鹭秦红军杨立强武百山岳剑宁杨惠婕倪家骧
中国全科医学 2015年32期
李艳,左欣鹭,秦红军,杨立强,武百山,岳剑宁,杨惠婕,倪家骧
C型臂X光机引导穿刺联合神经电生理分支定位技术在三叉神经半月节射频热凝术中的应用价值
李艳,左欣鹭,秦红军,杨立强,武百山,岳剑宁,杨惠婕,倪家骧
目的探讨C型臂X光机引导穿刺联合神经电生理指导三叉神经半月节射频热凝术治疗三叉神经痛(TN)的效果。方法选取2013年6月—2014年9月于首都医科大学宣武医院行C型臂X光机引导穿刺三叉神经半月节射频热凝术治疗的TN患者110例。采用随机数字表法将患者分为试验组和对照组,各55例。C型臂X光机扫描下确定卵圆孔,根据患者疼痛反应以及X线影像,调整射频针方向与深度,直至达卵圆孔内约3 mm。对照组根据给予电刺激时患者出现病变部位强烈的疼痛或感觉异常、肌肉抽动,确定针尖部位位于病变支。试验组分别于眶上孔、眶下孔、颏孔连接经皮记录电极,分别给予高、低频电刺激,多功能电流记录仪记录各支电位。以波幅较其他支波幅显著增高,确定针尖位置位于病变支。记录术后即刻、48 h疼痛视觉模拟评分(VAS)、麻木VAS及范围、并发症发生情况。分别于术后第1周及第1、3、6个月进行电话随访,记录疼痛VAS评分、麻木范围及复发情况。对照组和试验组分别完整随访53、47例。结果试验组术后即刻疼痛消失患者比例高于对照组,差异有统计学意义(P<0.05)。两组术后48 h、1周及1、3、6个月疼痛消失患者比例比较,差异无统计学意义(P>0.05)。试验组和对照组术后即刻麻木VAS分别为(7.3±1.4)、(8.5±1.5)分,差异有统计学意义(t=4.120,P<0.001)。对照组术后即刻、48 h、1周及1、3个月麻木超出预期范围患者比例高于试验组,差异有统计学意义(P<0.001)。对照组术后48 h呕吐发生率高于试验组,差异有统计学意义(P<0.05)。两组眩晕、恶心、复视、皮肤麻木及咀嚼肌无力发生率比较,差异均无统计学意义(P>0.05)。对照组1例患者于术后2周复发,试验组随访期间无复发患者。两组复发率比较,差异无统计学意义(P>0.05)。结论与电刺激患者反应引导穿刺技术比较,C型臂X光机引导联合神经电生理指导射频卵圆孔穿刺,病变支定位准确性较好,术后麻木超出预期范围的风险降低。
三叉神经痛;射频热凝术;X线;诱发电位
李艳,左欣鹭,秦红军,等.C型臂X光机引导穿刺联合神经电生理分支定位技术在三叉神经半月节射频热凝术中的应用价值[J].中国全科医学,2015,18(32):3926-3931.[www.chinagp.net]
Li Y,Zuo XL,Qin HJ,et al.Application value of puncture guided by C-arm X-ray machine combining nerve electrophysiology branch positioning technique in trigeminal semilunar ganglion radio frequency thermocoagulation[J].Chinese General Practice,2015,18(32):3926-3931.QIN Hong-jun,et al.Department of Pain Medicine,Xuanwu Hospital,Capital Medical University,Beijing 100053,China
三叉神经痛(trigeminal neuralgia,TN)是以面部三叉神经分布区内出现反复发作性、触电样、短暂而剧烈疼痛为临床特征的常见神经病理性疼痛。Koopman等[1]对荷兰调查显示TN发病率为12.6/10万,吴升平等[2]对我国6大城市调查显示TN发病率为4.3/10万。TN多发生于中老年人,女性多于男性[1]。原发性TN的发病机制尚不明确,因此,尚无确切根治性治疗方法。目前,TN首选药物治疗,但长期应用可发生耐药性。射频热凝术最初由Sweet等[3]不断改进并应用于治疗TN,因其创伤小、操作相对简单、并发症少而被临床医生及患者广泛接受,有效率达90%以上[4-7],但也存在咬肌瘫痪、复视、角膜炎、神经麻木性疼痛等术后并发症及复发的风险[5]。术中准确定位病变支是确保术后疗效及避免并发症的关键。目前临床TN病变支的定位主要依据电刺激及患者主诉,该方法主观性强,对于高度紧张、听力或语言沟通障碍等患者,术中判断可能会导致偏差,从而使疗效不佳或出现严重并发症。而神经电生理技术客观判断针尖位置,可较准确定位病变支。本研究探讨C型臂X光机引导下半月节穿刺,神经电生理辅助三叉神经分支定位的准确性,并分析术后疗效。
1 对象与方法
1.1病例纳入与排除标准纳入标准:(1)符合《国际头痛紊乱分类诊断》第2版[8]中TN诊断标准:突发性疼痛,持续数秒至2 min,涉及三叉神经一支或多支支配区,且疼痛特征为强烈的、尖锐的、表浅的或刀割样疼痛或由扳机点、诱发因素诱发,患者疼痛性质、发作形式不变,并排除神经损伤及其他疾病引起的疼痛; (2)年龄≥18岁;(3)疼痛程度为中重度;(4)药物治疗3个月以上仍有剧烈疼痛或不能耐受药物不良反应,或神经外科手术治疗无效或复发。排除标准:(1)颅脑CT或MRI扫描示颅内占位性病变,或颅内肿瘤继发性TN;(2)接受三叉神经感觉根切断术,面部遗留严重麻木;(3)严重系统性疾病;(4)有出血性疾病或凝血时间明显延长;(5)穿刺部位有感染病灶;(6)精神障碍或神经病变,语言沟通障碍,不能合作;(7)拒绝参加本研究。
1.2研究对象选取2013年6月—2014年9月于首都医科大学宣武医院行C型臂X光机引导穿刺三叉神经半月节射频热凝术治疗的TN患者110例。采用随机数字表法将患者分为试验组和对照组,各55例。患者合并慢性疾病主要为高血压、心脏病及糖尿病,入组前药物控制良好。
1.3方法
1.3.1手术方法患者入手术室后,监测心电图、无创血压、血氧饱和度,建立外周静脉通路,术前半小时静脉给予阿托品0.25 mg,氟哌利多2.5 mg。患者取仰卧位,肩稍垫高,头后仰,穿刺点为患侧口角延线与同侧眼眶中线垂直线的交叉点,局部常规消毒铺巾,局部给予局部麻醉药浸润麻醉。
C型臂X光机扫描下确定卵圆孔,依据Hartel穿刺方法,采用长150 mm、针尖裸露端直径5 mm的射频穿刺针进行穿刺,直达卵圆孔[9-10],针尖深度不能达到X线侧位颅底高密度叠加线。根据患者疼痛反应以及X线影像,不断调整进针方向与深度,直至达卵圆孔内约3 mm。
对照组患者给予高频电刺激(50 Hz,0.1 ms,0.1~0.5 V),从0.1 V逐渐增加,在此范围内如出现病变部位强烈的疼痛或感觉异常,确定针尖部位位于病变支;再以低频电刺激(2 Hz,1 ms,0.3~1.0 V),从1.0 V逐渐降低,在此范围诱发病变神经支配肌肉抽动,确定针尖部位位于病变支。针尖位置根据患者对神经系统电刺激反应进行微调至满足上述理想状态。
试验组针尖位置根据多功能电流记录仪(DAVINCI,Mogliano Veneto,意大利)行电刺激-分支皮区记录进行微调。第Ⅰ支经皮记录电极置于眶上孔,第Ⅱ支为眶下孔,第Ⅲ支为颏孔(见图1)。95%乙醇局部去脂,每一记录部位为正负一对盘状电极(正极在内,负极在外,两者间距为0.5 cm,且保证两电极间电阻≤5Ω,地线夹于病变同侧耳垂)。分别给予高频电刺激(50 Hz,0.1 ms,0.1~0.5 V)和低频电刺激(2 Hz,1 ms,0.3~1.0 V),多功能电流记录仪记录各支电位。以波幅较其他支波幅显著增高,确定针尖位置位于病变支(见图2)。

图1 体表记录电极固定位置Figure 1 Body surface records of electrode fixed positions
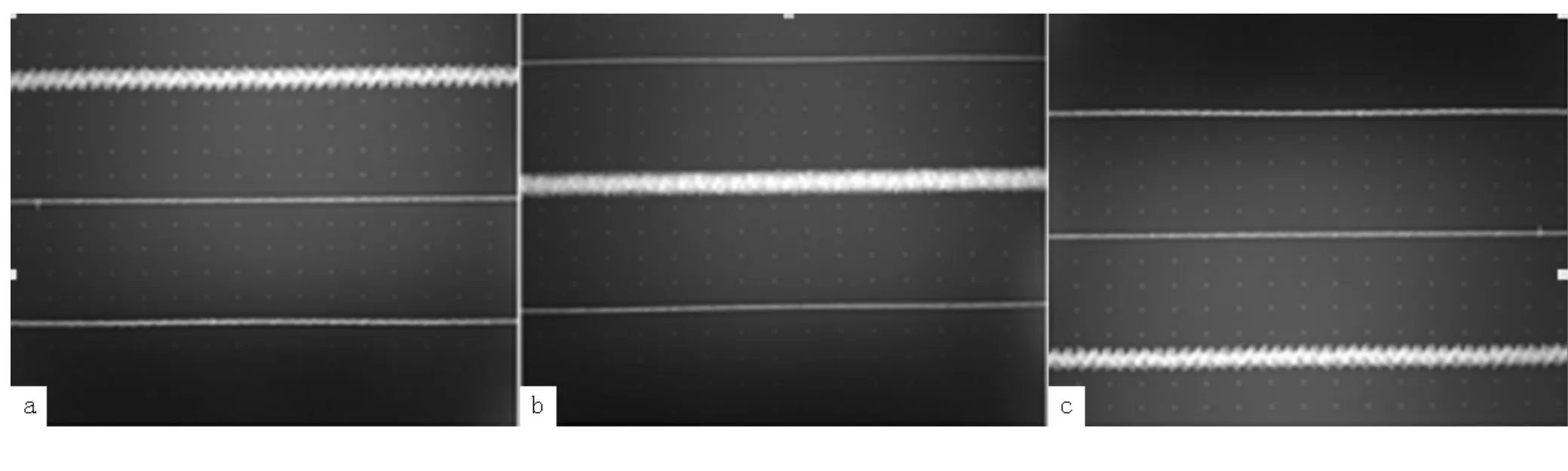
图2 高频电刺激三叉神经分支电位变化Figure 2 Trigeminal nerve branch potential changes by high-frequency electrical stimulation
射频针微调成功后,给予至少5 min面罩吸氧,静脉给予异丙酚(2 mg/kg)进行全身麻醉,70~75℃行射频热凝。
1.3.2药物治疗术后患者如无疼痛,可停用术前止痛药物,如有疼痛(需排除复发),继续服用术前止痛药物,依疼痛程度剂量可减半。术后麻木严重者可口服甲钴胺0.5 mg/次,3次/d,术后1个月停用。
1.3.3评估方法记录术后即刻、48 h疼痛视觉模拟评分(VAS)、麻木VAS及范围、并发症发生情况。如TN病变支定位准确以及限制热凝温度、时间的情况下,术后麻木范围应与术前病变支累及范围一致,否则判定麻木超出预期范围。分别于术后第1周及第1、3、6个月进行电话随访,记录疼痛VAS、麻木范围及复发情况。疼痛VAS评价前,患者需停药24 h。研究对象中9例因联系方式变更、错误,1例拒绝随访而失访,对照组和试验组分别完整随访53、47例。
1.4统计学方法采用SPSS 17.0统计软件进行统计分析,正态分布的计量资料以(±s)表示,组间比较采用t检验;非正态分布的计量资料以M(QR)表示,组间比较采用非参数检验;计数资料以相对数表示,组间比较采用χ2检验。以P<0.05为差异有统计学意义。
2 结果
2.1一般资料比较两组性别、年龄、病程、疼痛VAS、患侧及病变支分布比较,差异均无统计学意义(P>0.05,见表1)。

表1 两组一般资料比较Table 1 Comparison of general data between the two groups
2.2术后疼痛试验组术后即刻疼痛消失患者比例高于对照组,差异有统计学意义(P<0.05)。两组术后48 h、1周及1、3、6个月疼痛消失患者比例比较,差异无统计学意义(P>0.05,见表2)。
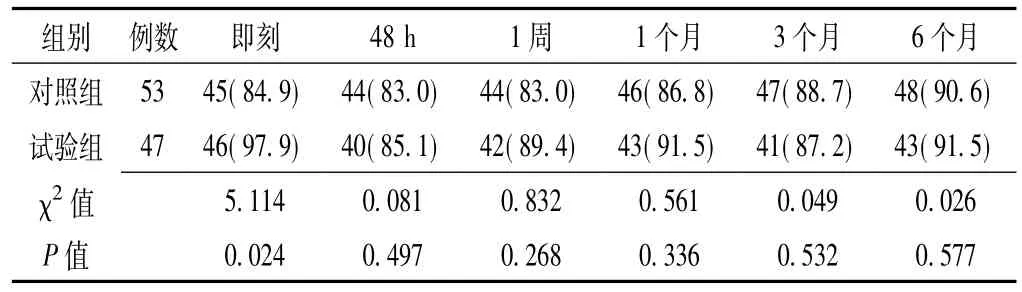
表2 两组术后各时间疼痛消失患者比例比较〔n(%)〕Table 2 Comparison of proportions of patients with postoperative pain disappearing at each time point after surgery between the two groups
2.3术后麻木试验组和对照组术后即刻麻木VAS分别为(7.3±1.4)、(8.5±1.5)分,差异有统计学意义(t=4.120,P<0.001)。对照组术后即刻、48 h、1周及1、3个月麻木超出预期范围患者比例高于试验组,差异有统计学意义(P<0.001)。两组术后6个月麻木超出预期范围患者比例比较,差异无统计学意义(P>0.05,见表3)。
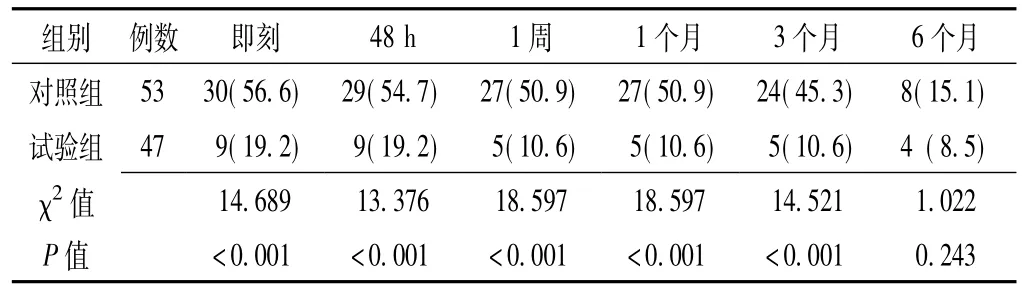
表3 两组术后各时间麻木超出预期范围患者比例比较〔n(%)〕Table 3 Comparison of proportions of patients with postoperative numbness outreaching range at each time point after surgery between the two groups
2.4并发症对照组术后48 h呕吐发生率高于试验组,差异有统计学意义(P<0.05)。两组眩晕、恶心、复视、皮肤麻木及咀嚼肌无力发生率比较,差异均无统计学意义(P>0.05,见表4)。
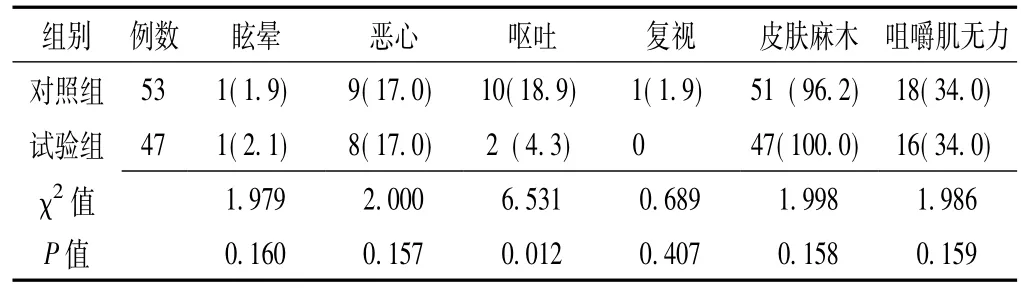
表4 两组术后48 h并发症发生率比较〔n(%)〕Table 4 Comparison of the incidence rates of complications 48 hours after surgery between the two groups
2.5复发情况对照组1例患者于术后2周复发,试验组随访期间无复发患者。两组复发率比较,差异无统计学意义(P>0.05)。
3 讨论
TN为一典型的、反复发作的、顽固的、非自愈性的神经病理性疼痛,治疗方法主要有药物、微创及开放手术。药物长期使用疗效不佳,且患者无法耐受其不良反应。经皮三叉神经半月节射频热凝术是被临床医生及患者普遍接受的微创治疗,该方法操作简单、安全、疗效较好,但仍存在发生术后麻木、角膜/结膜炎等并发症的风险。如何提高TN病变支定位准确性、避免或减少术后并发症的发生已成为临床亟待解决的问题。
早在1974年Sweet等[3]将射频热凝术用于TN的治疗。经皮三叉神经半月节射频热凝术治疗TN可有效控制温度和维持射频时间,选择性破坏半月神经节后无髓鞘的A-δ和C细神经纤维(司传导痛温觉),保留有髓鞘的A-α和β粗神经纤维(司传导触觉)。动物研究显示,A-δ和C细神经纤维在70℃和75℃时发生变性,而A-α和β粗神经纤维可耐受较高的温度[11]。因此,选择合适的射频热凝温度既可缓解TN,又可保留颜面部触觉,疗效达90%以上[4-7]。
在临床工作中,影响射频热凝术后疗效与并发症的关键为射频针穿刺和病变支定位。Lopez等[12]报道,徒手穿刺失败率约10%。若穿刺方向错误可导致颅神经损伤相关并发症,如角膜溃疡、失明、听力障碍、声音嘶哑和吞咽障碍等,甚至损伤大血管,刺入颈静脉孔刺激迷走神经,则引起心律失常[13-14]。反复穿刺可引发颅底血肿,进针深度不当则是术后头昏、恶心、呕吐的主要原因[15]。另外,TN也存在复发的风险,Tronnier等[16]报道射频热凝术治疗TN术后复发率约20%。
CT引导下可清晰识别卵圆孔,三维成像可指导穿刺方向,是目前多数临床医生所认可的穿刺引导方法[17-24]。但其费用高,且难以在基层医院普及。而X线也是引导穿刺到达卵圆孔的良好方法[25-28]。
上世纪80年代,有研究[29-31]开始探讨三叉神经半月节电刺激,于三叉神经三支皮肤分布区安置电极进行记录,观察波的潜伏期及峰值。在此基础上,有学者[32-33]将逆向电刺激应用到三叉神经半月节射频热凝术中分支定位。其中Li等[32]采用逆向电刺激行三叉神经热凝术中分支定位,结果显示电刺激分支记录阳性出现率与患者感知一致性较高,并且第Ⅲ支灵敏度高于第Ⅰ、Ⅱ支。
本研究为进一步探讨C型臂X光机引导下联合三叉神经半月节电刺激指导三叉神经半月节射频热凝术中分支定位准确性,设立以患者主诉定位为依据的对照组,比较两者术后疗效及并发症。若术中针尖位置不准确,遗留未处理神经纤维较多,而非病变支神经纤维处理较多,则出现复发或麻木超出预期范围[34-35]。本研究结果发现,对照组术后即刻、48 h、1周及1、3个月麻木超出预期范围的患者比例高于试验组,而两者术后6个月麻木超出预期范围的患者比例差异无统计学意义。分析原因可能为对照组患者术中损伤了部分非病变支,但在术后一定时间可自行修复。部分患者在术后即刻疼痛消失后再次出现疼痛,在术后6个月可恢复。其主要原因为部分患者射频热凝术后1~2周出现神经水肿,从而出现疼痛,待水肿恢复后疼痛即消失[36]。部分患者可能由于部分神经纤维未处理,射频热凝术后仍遗留疼痛,而术后神经修复或通过药物控制后疼痛消失。本研究两组患者术后即刻疼痛消失患者比例近90%,并可短期内维持疗效,且大部分患者术后无需服用镇痛药。麻木VAS超过8分者有50%服用甲钴胺,持续1个月。
与电刺激患者反应引导穿刺技术比较,C型臂X光机引导联合神经电生理指导射频卵圆孔穿刺,病变支定位准确性较好,术后麻木超出预期范围的风险降低。该技术避免了患者主观因素对确定针尖位置的影响,并降低由CT带来的医疗费用,尤其适于在高龄、有语言沟通障碍或听力障碍等不能合作的患者中进行推广。本研究随访时间短,患者长期疗效及复发风险可能存在一定偏倚,本研究结论尚需大样本、长期随访进一步证实。
[1]Koopman JS,Dieleman JP,Huygen FJ,et al.Incidence of facial pain in the general population[J].Pain,2009,147(1/3):122-127.
[2]吴升平,王文志,李世绰.中国六城市居民三叉神经痛的流行病学[J].中华神经外科杂志,1989,S1:1.
[3]Sweet WH,Wepsic JG.Controlled thermocoagulation of trigeminal ganglion and rootlets for differential destruction of pain fibers.1.Trigeminal neuralgia[J].J Neurosurg,1974,40(2):143-156.
[4]张秀双,杨立强,何明伟,等.CT引导下半月神经节射频热凝治疗术治疗三叉神经痛的远期疗效分析[J].中国康复医学杂志,2011,26(9):865-866.
[5]刘灵慧,黄仁辉.射频热凝术治疗三叉神经痛的并发症探讨[J].中国神经精神疾病杂志,2002,28(3):215-220.
[6]Singh S,Verma R,Kumar M,et al.Experience with conventional radiofrequency thermorhizotomy in patients with failed medical management for trigeminal neuralgia[J].Korean JPain,2014,27 (3):260-265.
[7]Wu CY,Meng FG,Liu YG,et al.Clinical experience and skill of selective percutaneous radiofrequecy thermocoagulation for the treatment of trigeminal neuralgia of 1936 cases[J].Chinese Journal of Pain Medicine,2005,11(1):15-21.(in Chinese)吴承远,孟凡刚,刘玉光,等.选择性射频热凝治疗三叉神经痛1936例临床分析与手术技巧[J].中国铁通医学杂志,2005,11(1):15-21.
[8]Silberstein SD,Olesen J,Bousser MG,et al.The International Classification of Headache Disorders,2nd Edition(ICHD-Ⅱ)-revision of criteria for 8.2 Medication-overuse headache[J].Cephalalgia,2005,25(6):460-465.
[9]Ni JX,Li CY,Xue JX,et al.Percutaneous puncture and chemical neurolysis of gasserrian ganglion under the guide of computerized tomography for the treatment of trigeminal neuralgia[J].Chinese Journal of Pain Medicine,2003,9(4):199-202.(in Chinese)倪家骧,李彩英,薛纪秀,等.CT引导和非引导下半月神经节毁损术治疗三叉神经痛[J].中国疼痛医学杂志,2003,9 (4):199-202.
[10]Tang YZ,Jin D,Bian JJ,et al.Long-term outcome of computed tomography-guided percutaneous radiofrequency thermocoagulation for classic trigeminal neuralgia patients older than 70 years[J].J Craniofac Surg,2014,25(4):1292-1295.
[11]Van Kleef M,Liem L,Lousberg R,et al.Radiofrequency lesion adjacent to the dorsal root ganglion for cervicobrachial pain:a prospective double blind randomized study[J].Neurosurgery,1996,38(6):1127-1131.
[12]Lopez BC,Hamlyn PJ,Zakrzewska JM.Systematic review of ablative neurosurgical techniques for the treatment of trigeminal neuralgia[J].Neurosurgery,2004,54(4):973-982.
[13]夏成雨,凌志培,牛朝诗.经皮穿刺三叉神经半月节射频热凝加甘油注射治疗原发性三叉神经痛(附85例报告)[J].立体定向和功能性神经外科杂志,2004,17(1):332-336.
[14]Egan RA,Pless M,Shults WT.Monocular blindness as a complication of trigeminal radiofrequency rhizotomy[J].Am J Ophthalmol,2001,131(2):237-240.
[15]Aryan HE,Nakaji P,Lu DC,et al.Multimodality treatment of trigeminal neuralgia:impact of radiosurgery and high resolution magnetic resonance imaging[J].JClin Neurosci,2006,13(2):239-244.
[16]Tronnier VM,Rasche D,Hamer J,et al.Treatment of idiopathic trigeminal neuralgia:comparison of long-term outcome after radiofrequency rhizotomy and microvascular decompression[J].Neurosurgery,2001,48(6):1261-1267.
[17]Gong WY,Huang QJ,Chen H,et al.3D-CT-guided percutaneous radiofrequency thermocoagulation in treatment of trigeminal neuralgia[J].Chinese Journal of Medical Imaging Technology,2008,24(12):2020-2025.(in Chinese)公维义,黄其健,陈华,等.三维CT引导下经皮射频热凝术治疗三叉神经痛[J].中国医学影像技术,2008,24(12): 2020-2025.
[18]Pan ZX.Effect of treatment of trigemjnaI neuraIgia using radiofrequency thermocoagulation[J].Journal of Hainan Medical College,2008,14(4):400-402.(in Chinese)潘在轩.射频温控热凝术治疗原发性三叉神经痛80例临床分析[J].海南医学院学报,2008,14(4):400-402.
[19]程福舟.CT引导下射频热凝术治疗三叉神经痛[J].中国基层医药,2009,16(9):1633-1635.
[20]Dun ZP,Ma CQ,Shang JR,et al.64-slice spiral CT assisted stereotactic puncture in treatment of trigeminal neuralgia[J].Journal of Medical Imaging,2011,21(1):8-13.(in Chinese)顿志平,马传青,尚景瑞,等.64排螺旋CT辅助立体定向穿刺治疗三叉神经痛[J].医学影像学杂志,2011,21(1):8-13.
[21]衣玉胜,刘传圣,徐风和,等.CT引导下半月神经节射频热凝术在三叉神经痛病人治疗中的临床应用[J].实用放射学杂志,2011,27(8):1253-1256.
[22]王晓志.CT引导射频热凝术治疗三叉神经痛临床分析[J].中国基层医药,2013,20(22):3430-3433.
[23]于勇,苏本玄,于骋,等.螺旋CT引导精确穿刺射频温控热凝术治疗经典型三叉神经痛的临床应用[J].徐州医学院学报,2013,33(10):628-635.
[24]张响,杨涛,华泽权,等.实时CT引导下的经皮半月神经节射频热凝术[J].临床口腔医学杂志,2014,30(11):646-649.
[25]Zhao XJ,He JW,Bai GH,et al.Study of DSA-guided percutaneous puncture location of foramen oval[J].Journal of Diagnostic Imaging and Interventional Radiology,2008,17(5): 200-204.(in Chinese)赵晓君,何家维,白光辉,等.DSA引导经皮穿刺卵圆孔定位技术的探讨[J].影像诊断与介入放射学,2008,17(5): 200-204.
[26]GrunertP,GlaserM,Kockro R,etal.An alternative projection for fluoroscopic-guided needle insertion in the foramen ovale:technical note[J].Acta Neurochir(Wien),2010,152(10):1785-1792.
[27]Xue TQ,Yang ZQ,Ding WB,et al.Radiofrequency therapy of intractablemaxillary neuralgia with the help of fine needle puncturing of foramen rotundum under X-ray guidance:a clinical study[J].Journal of Interventional Radiology,2011,20(10):765-769.(in Chinese)薛同庆,杨正强,丁文彬,等.X线导引下细针穿刺圆孔射频治疗顽固性上颌神经痛的临床研究[J].介入放射学杂志,2011,20(10):765-769.
[28]郑婧,张光志,董庆鹏,等.X线引导下穿刺针位于卵圆孔内不同深度射频治疗三叉神经痛疗效观察[J].中国疼痛医学杂志,2014,20(5):357-360.
[29]Cruccu G.Intracranial stimulation of the trigeminal nerve in man.Ⅰ.Direct motor responses[J].J Neurol Neurosurg Psychiatry,1986,49(4):411-418.
[30]Cruccu G,Bowsher D.Intracranial stimulation of the trigeminal nerve in man.Ⅱ.Reflex responses[J].J Neurol Neurosurg Psychiatry,1986,49(4):419-427.
[31]Cruccu G,InghilleriM,ManfrediM,etal.Intracranial stimulation of the trigeminal nerve in man.Ⅲ.Sensory potentials[J].J Neurol Neurosurg Psychiatry,1987,50(10):1323-1330.
[32]Li X,Yue J,Yang L,et al.Application of antidromic conduction monitoring in ganglion radiofrequency thermocoagulation for locating trigeminal branches in trigeminal neuralgia[J].Pain Pract,2015.doi:10.1111/papr.12286.
[33]Lin B,Lu X,Zhai X,et al.Use of sensory and motor action potentials to identify the position of trigeminal nerve divisions for radiofrequency thermocoagulation[J].Journal of Neurosurgery,2014,121(6):1497-1503.
[34]Feng BH,Zheng XS,Ying TT,et al.Anatomical study on posterior root fibers of trigeminal nerve using electrophysiological monitoring[J].Chinese Journal of Neurosurgery,2010,26 (12):1074-1077.(in Chinese)冯保会,郑学胜,应婷婷,等.电生理监测对三叉神经后根纤维的解剖学定位研究[J].中华神经外科杂志,2010,26 (12):1074-1077.
[35]Jin D,Li YH,Huang JL,et al.Different locating methods of radiofrequency thermocoagulation for trigeminal neuralgia on semilunar ganglion[J].InternationalMedicine and Health Guidance News,2010,16(16):1952-1956.(in Chinese)金丹,李云辉,黄建龙,等.三叉神经半月节射频热凝术不同定位方法比较[J].国际医药卫生导报,2010,16(16): 1952-1956.
[36]Ge PL,Liu RZ,Chen QX,et al.Cranial nerve complications after microsurgical treatment of trigeminal neuralgia[J].Chinese Journal of Neuromedicine,2005,4(11):1165-1166.(in Chinese)葛培林,刘仁忠,陈谦学,等.三叉神经微血管减压术后颅神经并发症[J].中华神经医学杂志,2005,4(11):1165-1166.
(本文编辑:吴立波)
App lication Value of Puncture Guided by C-arm X-ray M achine Com bining Nerve Electrophysiology Branch Positioning Technique in Trigem inal Sem ilunar Ganglion Radio Frequency Thermocoagulation
LIYan,ZUO Xin-lu,QIN Hong-jun,et al.Department of Pain Medicine,Xuanwu Hospital,Capital Medical University,Beijing 100053,China
Objective To investigate the effect of puncture guided by C-arm X-ray machine combining nerve electrophysiology in the treatment of trigeminal neuralgia(TN)by trigeminal semilunar ganglion radio frequency thermocoagulation.M ethods We enrolled 110 TN patients who underwent trigeminal semilunar ganglion radio frequency thermocoagulation with puncture guided by C-arm X-raymachine in Xuanwu Hospital,Capital Medical University from June 2013 to September 2014.By random number tablemethod,the subjectswere divided into trialgroup and controlgroup,with 55 patients in each group.Oval foramen was confirmed by the scan of C-arm X-raymachine,and the direction and depth of radio frequency needle were adjusted according to patients'pain reaction and X-ray image until the needle reached 3 mm inside ovalforamen.For control group,whether the needle tip was positioned in lesion branch was determined by whether strong pain or paresthesia appeared and muscle twitch when electrical stimulation was given.For trial group,percutaneous recording electrodes were connected at supraorbital foramen,infraorbital foramen and mental foramen,after which high-frequency electrical stimulation and low-frequency electrical stimulation given,and electric potential of each branch was recorded by multifunctional galvo-recorder;whether the needle tip was located in lesion branch was determined by whether the wave amplitude of a branch was evidently higher than other branches.The VAS pain score,the VAS numbness score,the range of numbness and the incidence rates of complicationswere recorded immediately and 48 hoursafter surgery.Telephone follow-up was conducted 1 week,1 month,3 months and 6 months after surgery,during which the VAS pain score,range of numbness and relapse were recorded.The number of patients who completed the follow-up was 53 for control group and 47 for trial group.Results Trial group was higher(P<0.05)than control group in the proportion of patients whose pain disappeared immediately after surgery.The two groups were not significantly different(P>0.05)in the proportions of patients whose pain disappeared 48 hours,1 week,1 month,3 months and 6 months after surgery.The VAS score of immediate numbness was(7.3±1.4)for trial group and(8.5±1.5)for control group(t=4.120,P<0.001).Control group was higher than trial group in the proportions of patients whose numbness outreached the expected range immediately,48 hours,1 week,1 month and 3 months after surgery were higher than trial group(P<0.001).Control group was higher(P<0.05)than trial in the incidence of emesis 48 hours after surgery.The two groups were not significantly different(P>0.05)in the incidence of dizziness,nausea,diplopia,skin numbness and masticatorymuscle weakness.One patient in control group relapsed after surgery,and no patient relapsed during follow-up in trialgroup.The two groupswere notsignificantly different in recurrence rate(P>0.05).Conclusion Compared with puncture guided by patients'response to electric stimulation,oval foramen puncture guided by C-arm X-ray machine combining nerve electrophysiology is more accurate in the positioning of lesion branch and leads to lower risk in numbness outreaching expected range after surgery.
Trigeminal neuralgia;Radiofrequency thermocoagulation;X-ray;Evoked potentials
R 745.11
A
10.3969/j.issn.1007-9572.2015.32.008
北京市科技计划课题(Z131107002213154)
100053北京市,首都医科大学宣武医院疼痛科(李艳,杨立强,武百山,岳剑宁,杨惠婕,倪家骧);承德护理职业学院(左欣鹭);北京电力医院放射科(秦红军)
倪家骧,100053北京市,首都医科大学宣武医院疼痛科;E-mail:nijiaxiang@263.net
2015-01-11;
2015-09-18)
猜你喜欢
中老年保健(2022年1期)2022-08-17
河南外科学杂志(2020年6期)2020-12-05
中华脑科疾病与康复杂志(电子版)(2020年6期)2020-04-22
医药前沿(2019年27期)2019-11-07
北方人(2019年18期)2019-09-20
中国中西医结合外科杂志(2019年4期)2019-08-19
装备制造技术(2017年7期)2017-09-23
中国临床医学影像杂志(2017年4期)2017-08-31
中国老年学杂志(2017年5期)2017-01-17
中国当代医药(2015年10期)2015-03-01
