尼可地尔在三支血管病变冠心病患者中的应用价值
2015-04-13 12:01刘先霞
海南医学 2015年11期
赵 勇,刘先霞
(海南省农垦总医院心内科,海南 海口 570311)
尼可地尔在三支血管病变冠心病患者中的应用价值
赵 勇,刘先霞
(海南省农垦总医院心内科,海南 海口 570311)
目的 探讨尼可地尔治疗三支血管病变冠心病患者的临床效果。方法随机选取2011年7月至2014年7月我院收治的冠心病三支血管病变患者84例,随机数表法分组,其中42例常规治疗者为对照组,42例加用尼可地尔治疗者为观察组。疗程为3个月,3个月后观察两组患者每日心绞痛发作次数及持续时间、硝酸甘油服用量、心梗等心脑血管事件发生情况,并根据SF-36量表对患者生活质量进行评估。结果治疗3个月后,两组患者的每日心绞痛发作次数、持续时间、硝酸甘油服用量均有所减少,且观察组明显优于对照组,各指标比较差异均具有统计学意义(P<0.05);治疗期间两组并发症均较少,观察组和对照组发生率分别为4.8%和10.4%,差异具有统计学意义(P<0.05);治疗后两组生活质量均有所改善,且观察组明显优于对照组,其差异具有统计学意义(P<0.05)。结论尼可地尔治疗冠心病三支病变者的临床效果较好,可明显改善心绞痛症状,提高患者生活质量,且并发症较少。
尼可地尔;冠心病;三支病变
冠状动脉三支血管病变是冠心病的类型之一,较单支、双支病变相比,病变数目更多、损伤更重[1]。临床上常采用的治疗方案有多种,如基因及细胞促血管再生治疗、非侵入性干细胞移植治疗,或经皮左心室-冠状动脉搭桥术、原位冠状动脉旁路术等外科治疗,但由于三支病变血管破坏严重,加之一些新技术不成熟,给临床治疗增加了困难[2-5]。目前药物保守治疗仍是临床的首选。尼可地尔是一种具有类硝酸酯类作用的ATP敏感的K+通道激活剂,其在减少心绞痛发作次数,改善心功能,减少恶性心律失常及猝死的发生率,以及预防经皮冠状动脉介入(PCI)手术缺血再灌注损伤等方面的价值,得到广泛认可。我院对42例三支病变的冠心病患者予以尼可地尔治疗,发现其临床治疗效果较好,现报道如下:
1 资料与方法
1.1 一般资料 选取2011年7月至2014年7月来我院就诊的冠心病患者84例,随机数字表法分组,42例常规治疗者作为对照组,42例加用尼可地尔进行治疗者作为观察组。所有入选患者均满足以下条件[6-8]:(1)半年内由冠脉造影术检查示冠状动脉三支病变,包括无症状心肌缺血、稳定及不稳定心绞痛、非ST段抬高心肌梗死及ST段抬高心肌梗死;(2)由于远端血供差无法行血管搭桥手术或患者家属拒绝外科治疗;(3)经抗心肌缺血治疗后仍有胸闷胸痛等症状出现;(4)心功能均小于Ⅲ级,EF>30%;(5)心肌酶谱未升高;(6)无肝肾功能不全、恶性肿瘤、严重免疫系统疾病及血液系统疾病者。观察组患者中男性22例,女性20例;年龄45~89岁,平均(67.3±8.2)岁;冠心病史1~35年,平均(1.8±1.1)年;急性/亚急性心梗13例,不稳定型心绞痛14例,稳定型心绞痛9例,缺血性心肌病6例。对照组患者中男性24例,女性18例;年龄42~90岁,平均(69.7±7.5)岁;冠心病史1~37年,平均(2.1±1.3)年;急性/亚急性心梗15例,不稳定型心绞痛12例,稳定型心绞痛10例,缺血性心肌病5例。两组患者的年龄、性别、病程等临床资料比较差异均无统计学意义(P>0.05),具有可比性。
1.2 方法 对照组予以常规治疗。即按照冠心病常规降压(美托洛尔、培哚普利、盐酸地尔硫卓)、降脂(阿托伐他丁钙片)、扩管(单硝酸异山梨酯)、抗血小板凝集(阿司匹林、氯吡格雷)、改善心肌代谢(盐酸曲美他嗪)治疗。观察组在对照组治疗的基础上加用尼可地尔进行治疗。尼可地尔片(浙江惠松制药有限公司,国药准字H33021862)1片/次,3次/d。疗程3个月。若患者在治疗过程中有胸闷胸痛发作,予以硝酸甘油片(哈药集团制药六厂,国药准字H23021574)1片(0.5 mg)舌下含服。
1.3 观察指标 在服药3个月后随访,观察两组患者每日心绞痛发作次数及持续时间(min),硝酸甘油服用量(片),心梗等心脑血管事件发生情况及治疗期间不良反应。并参考SF-36量表[9-10]对患者生活质量进行评估。
1.4 统计学方法 应用SPSS13.0软件进行数据统计分析,计量数据以均数±标准差(±s)表示,其组间比较采用t检验,计数资料比较采用χ2检验,以P<0.05为差异具有统计学意义。
2 结果
2.1 两组患者每日心绞痛发作次数、持续时间及硝酸甘油服用量比较 治疗后两组患者每日心绞痛发作次数、持续时间、硝酸甘油服用量均有所减少,且观察组明显优于对照组,治疗后各指标比较差异均具有统计学意义(P<0.05),见表1。
表1 两组患者每日心绞痛发作次数、持续时间及硝酸甘油服用量比较(±s)
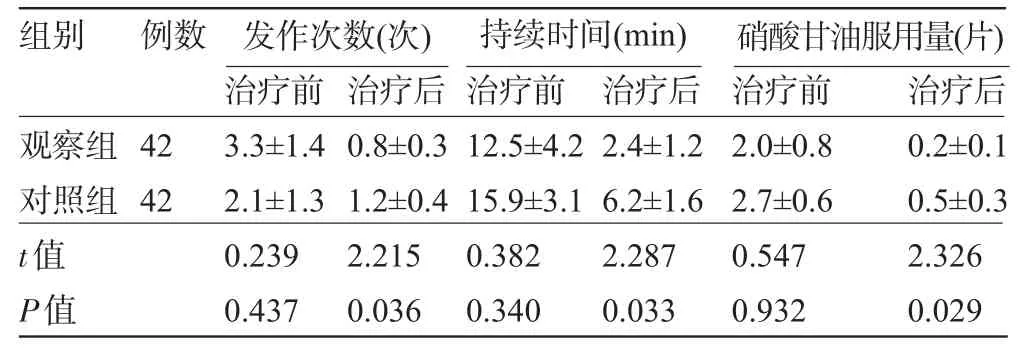
表1 两组患者每日心绞痛发作次数、持续时间及硝酸甘油服用量比较(±s)
例数组别观察组对照组42 42 3.3±1.4 2.1±1.3 0.8±0.3 1.2±0.4 12.5±4.2 15.9±3.1 2.4±1.2 6.2±1.6 2.0±0.8 2.7±0.6 0.2±0.1 0.5±0.3t值P值发作次数(次) 持续时间(min) 硝酸甘油服用量(片)治疗前0.239 0.437治疗后2.215 0.036治疗前0.382 0.340治疗后2.287 0.033治疗前0.547 0.932治疗后2.326 0.029
2.2 两组心血管事件发生情况比较 治疗期间观察组出现急性心梗1例,脑梗0例,死亡1例;对照组出现急性心梗2例,脑梗1例,死亡2例,发生率分别为4.8%和10.4%,结果比较差异具有统计学意义(χ2=8.374,P<0.05)。
2.3 两组治疗前后生活质量评分比较 治疗后两组患者的生活质量均有所改善,且观察组明显优于对照组,差异具有统计学意义(P<0.05),见表2。
表2 两组患者治疗前后的生活质量比较(±s,分)
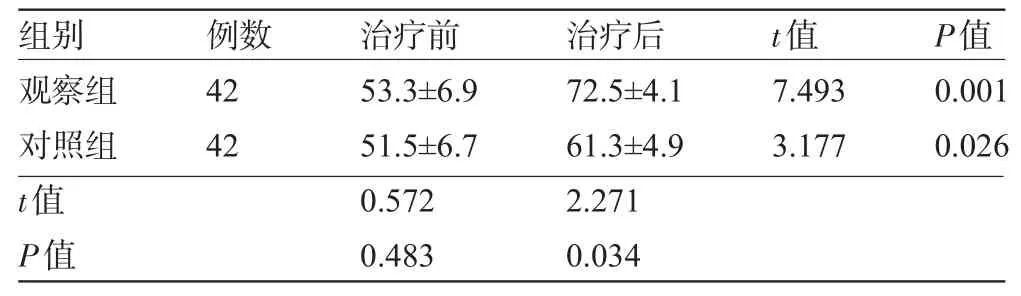
表2 两组患者治疗前后的生活质量比较(±s,分)
组别 例数 治疗前 治疗后t值P值观察组对照组t值P值42 42 53.3±6.9 51.5±6.7 0.572 0.483 72.5±4.1 61.3±4.9 2.271 0.034 7.493 3.177 0.001 0.026
2.4 两组不良反应比较 观察组出现腹泻1例,头痛2例;对照组出现腹泻2例,恶心呕吐1例,头痛2例,发生率为7.1%和11.9%,结果比较差异具有统计学意义(χ2=3.897,P<0.05)。
3 讨 论
随着社会发展,人们生活习惯的改变,冠心病的发病率逐年增加。冠心病主要是由于冠状动脉发生动脉血管粥样硬化而引起血管腔狭窄或阻塞,出现心肌缺血、缺氧或坏死等病变。冠状动脉多支血管病变(MVD)是其十分严重的一种类型[11]。临床上将至少两支主要冠状动脉或其分支直径狭窄大于50%定义为MVD,可分为二支病变、三支病变、LM病变等[12]。多支病变具有弥漫性、复杂性,常伴有心功能降低。由于血管损伤严重,给冠脉搭桥术等外科治疗增大了难度,同时远期预后也较单支病变者差,并发症多。国内关于冠状动脉三支病变研究的报道较少,国外报道较多,Mohammadi等[13]和Komiyama等[14]曾比较过PCI与CABG的效果,二者均能有效恢复心肌的血供,但仍不可避免冠脉闭塞及再狭窄的可能性。因此大多医生倾向于采取内科保守治疗。以往的保守治疗多为降压、降脂、扩管、抗血小板凝集、改善心肌代谢及对症支持治疗。
近年来,有报道称尼可地尔在MVD的治疗中有不错的效果[15]。尼可地尔具有双重药理学机理,既有如硝酸酯类药物扩血管功能,也有ATP敏感的K通道(KATP)激活作用,表明其同时具有扩张动静脉血管的作用[16]。扩张动脉能有效减轻心脏后负荷,增加心脏射血功能;而扩张静脉则可改善充血,增加静脉系统血容量。尼可地尔由Kir和SUR两种亚基组成。Kir亚基为内向整流钾离子通道,是一种离子通道;SUR是ATP结合蛋白,为依赖ATP的钾离子通道[17-18]。
本研究中,我们发现在加用尼可地尔进行治疗的组别中,心肌梗死等心肌缺血明显得到改善。在治疗期间观察组出现急性心梗(AMI)1例,脑梗0例,死亡1例;对照组出现急性心梗2例,脑梗1例,死亡2例,发生率分别为4.8%和10.4%,结果比较差异具有统计学意义(P<0.05),与相关研究结果一致。Li等[19]在研究中敲除了编码心肌表明KATP通道的基因kir6.2,观察在结扎冠状动脉前降支前后心电图的改变,结果显示被敲除基因的小鼠ST段明显压低,而野生鼠却为抬高状态,可见冠脉结扎导致心肌血供不足时,KATP通道具有十分关键的作用。本研究中,我们发现治疗前后两组患者每日心绞痛发作次数、持续时间、硝酸甘油服用量均有所减少,观察组明显优于对照组,治疗后各指标比较,差异显著具有统计学意义(P<0.05)。可见,尼可地尔有效改善了心绞痛的症状。硝酸甘油片一般在心绞痛较为严重时舌下含服,可快速扩张冠状动脉及外周小动脉,改善心肌缺血[20]。
在治疗期间药物不良反应大小是衡量治疗效果的关键。我们发现,观察组的不良反应发生率明显低于对照组,差异具有统计学意义(P<0.05)。此外,我们评价了患者治疗前后的生活质量,SF-36量表共有9个维度和36个条目,分别可以反映生理功能、生理职能、身体疼痛、总体健康、活力、社会功能、情感职能、精神健康及健康变化。各条目得分越高,说明生活质量越高。两组治疗前后生活质量评分结果比较,治疗后两组生活质量均有所改善,观察组明显优于对照组,差异具有统计学意义(P<0.05)。
综上所述,尼可地尔治疗冠心病三支病变者的临床效果较好,可明显改善心绞痛症状,提高患者生活质量,且并发症较少,值得临床推广。
[1]Kovacic JC,Limaye AM,Sartori S,et al.Comparison of six risk scores in patients with triple vessel coronary artery disease undergoing PCI:competing factors influence mortality,myocardial infarction,and target lesion revascularization[J].Catheter Cardiovasc Interv,2013,82(6):855-868.
[2]Zhao M,Stampf S,Valina C,et al.Role of euroSCOREⅡin predicting long-term outcome after percutaneous catheter intervention for coronary triple vessel disease or left main stenosis[J].Int J Cardiol,2013,168(4):3273-3279.
[3]Su PX,Gu S,Liu Y,et al.Partial sternotomy coronary surgery with triple-vessel disease in dextrocardia and situs inversus totalis[J].Interact Cardiovasc Thorac Surg,2013,17(1):213-215.
[4]Buxton BF,Shi WY,Tatoulis J,et al.Total arterial revascularization with internal thoracic and radial artery grafts in triple-vessel coronary artery disease is associated with improved survival[J].J Thorac Cardiovasc Surg,2014,148(4):1238-1243
[5]Buxton BF,Hayward PA.The art of arterial revascularization-total arterial revascularization in patients with triple vessel coronary artery disease[J].Ann Cardiothorac Surg,2013,2(4):543-551.
[6]Ojeda D,Le Rolle V,Harmouche M,et al.Sensitivity analysis and parameter estimation of a coronary circulation model for triple-vessel disease[J].IEEE Trans Biomed Eng,2014,61(4):1208-1219.
[7]Dou K,Xu B,Yang Y,et al.Comparison of procedural and long-term outcomesbetween transradialand transfemoralapproach in one-stage intervention for triple vessel coronary artery disease[J].J Interv Cardiol,2014,27(2):108-116.
[8]Prabhavathi R,Reddy NP,Sekhar TsC,et al.A case of triple vessel disease posted for buccal mucosal graft urethroplasty under low dose spinal anaesthesia with dexmedetomedine[J].Indian J Anaesth,2013,57(4):428-429.
[9]Ojeda D,Le Rolle V,Drochon A,et al.Multiobjective patient-specific estimation of a coronary circulation model for triple vessel disease[J].Conf Proc IEEE Eng Med Biol Soc,2013,2013:3877-80.
[10]Tazaki J,Shiomi H,Morimoto T,et al.Three-year outcome after percutaneous coronary intervention and coronary artery bypass grafting in patients with triple-vessel coronary artery disease:observations from the CREDO-Kyoto PCI/CABG registry cohort-2[J].EuroIntervention,2013,9(4):437-445.
[11]Malkin CJ,George V,Ghobrial MS,et al.Residual SYNTAX score after PCI for triple vessel coronary artery disease:quantifying the adverse effect of incomplete revascularization[J].EuroIntervention, 2013,8(11):1286-1295.
[12]Kim YR,Park JH,Lee HJ,et al.The effect of doubling the statin dose on pro-inflammatory cytokine in patients with triple-vessel coronary artery disease[J].Korean Circ J,2012,42(9):595-599.
[13]Mohammadi S,Kalavrouziotis D,Dagenais F,et al.Completeness of revascularization and survival among octogenarians with triple-vessel disease[J].Ann Thorac Surg,2012,93(5):1432-1437.
[14]Komiyama K,Tejima T,Ashikaga T,et al.A case of severe aortic valve stenosis including triple-vessel ischemic heart disease in which multidisciplinary percutaneous coronary intervention and balloon aortic valvuloplasty relieved low cardiac output syndrome[J]. Cardiovasc Interv Ther,2014[Epub ahead of print]
[15]Serruys PW,Morice MC,KapPetein AP,et al.Pereutaneous coronary intervention versus coronary-artery bypass grafting for severe coronary artery disease[J].N Engl J Med,2009,360(10):961-972.
[16]Rademacher W,Lauten A,Lauten A,et al.Postpartum unmasking of a severe triple-vessel-disease with acute myocardial infarction [J].Clin Res Cardiol,2010,99(7):463-466.
[17]Sivalingam SK,Parthasarathy HK,Choong CK,et al.Severe triple vessel coronary artery disease and aneurysms in a young white man:disease progression of childhood Kawasaki disease[J].J Cardiovasc Med(Hagerstown),2009,10(2):170-173.
[18]Navia D,Vrancic M,Vaccarino G,et al.Total arterial off-pump coronary revascularization using bilateral internal thoracic arteries in triple-vessel disease:surgical technique and clinical outcomes[J]. Ann Thorac Surg,2008,86(2):524-530.
[19]Li RA,Leppo M,Miki T Molecular basis of electrocardiographic ST-segment elevation[J].Circulation Research,2000,87(10):837-839.
[20]Ota K,Tsutsumi T,Kawachi K,et al.Time-frequency analysis of QRS complex with wavelet transform in patients with triple-vessel disease[J].Anadolu Kardiyol Derg,2007,7(1):133-134.
Value of Nicorandil in patients with triple-vessel coronary heart disease.
ZHAO Yong,LIU Xian-xia.Department of Cardiology,Hainan Provincial Nongken General Hospital,Haikou 570311,Hainan,CHINA
ObjectiveTo explore the clinical value of Nicorandil in patients with triple-vessel coronary heart disease.MethodsEighty-four patients with triple-vessel coronary heart disease in our hospital from July 2011 to July 2014 were divided into two groups by random number table.The 42 patients in control group received conventional treatment,while the 42 patients in the observation group added Nicorandil for treatment based on the control group.All the patients were treated for 3 months.Then the daily frequency and duration of angina pectoris,nitroglycerin dose,myocardial infarction and other cardiovascular and cerebrovascular events were observed.The quality of life of patients was assessed according to SF-36 questionnaire.ResultsAfter treatment,the daily frequency and duration of angina pectoris,nitroglycerin dose in the two groups were all declined,and the improvement was significantly better in the observation group than the control group,with statistically significant difference between the two groups(P<0.05). The incidence of complications of both groups were low,with 4.8%in the observation group and 10.4%in the control group,showing statistically significant difference between the two groups(P<0.05).Quality of life scores after treatment were improved in both group,and the improvement in the observation group was significantly better(P<0.05).ConclusionNicorandil has great effect on triple-vessel coronary heart disease.It can improve the angina symptoms significantly and improve the quality of life of patients,and results in less complications,which is worthy of promotion.
Nicorandil;Coronary heart disease;Triple-vessel
R541.4
A
1003—6350(2015)11—1573—03
10.3969/j.issn.1003-6350.2015.11.0563
2014-11-13)
海南省卫生厅科学研究课题(编号:琼卫2012PT-92)
赵 勇。E-mail:zhaoyong19771@163.com
猜你喜欢
中老年保健(2022年1期)2022-08-17
中国典型病例大全(2022年11期)2022-05-13
中华养生保健(2020年9期)2021-01-18
中华养生保健(2020年3期)2020-11-16
大众健康(2020年11期)2020-11-13
爱你(2019年5期)2019-11-14
祝您健康(2019年10期)2019-10-18
家庭科学·新健康(2018年11期)2018-11-16
中国循证心血管医学杂志(2018年2期)2018-01-16
老年医学与保健(2017年6期)2017-02-06