
Bariatric surgery in old age:a comparative study of laparoscopic Roux-en-Y gastric bypass and sleeve gastrectomy in an Asia centre ofexcellence
2015-01-09 11:51ChihKunHuangAmitGargHsinChihKuaoPoChihChangMingCheHsin
Chih-Kun Huang,Amit Garg,Hsin-Chih Kuao,Po-Chih Chang,Ming-Che Hsin
1Bariatric&Metabolic International(B.M.I)Surgery Centre,E-Da Hospital,Kaohsiung,Taiwan,China;
2Department of Health Management,I-Shou University,Kaohsiung,Taiwan,China.
Bariatric surgery in old age:a comparative study of laparoscopic Roux-en-Y gastric bypass and sleeve gastrectomy in an Asia centre ofexcellence
Chih-Kun Huang1,✉,Amit Garg1,Hsin-Chih Kuao2,Po-Chih Chang1,Ming-Che Hsin1
1Bariatric&Metabolic International(B.M.I)Surgery Centre,E-Da Hospital,Kaohsiung,Taiwan,China;
2Department of Health Management,I-Shou University,Kaohsiung,Taiwan,China.
Bariatric surgery hasbeen proved to be the safestand efficientprocedure in treating morbid obese patients,butdata is stilllacking in the elderly population.The aim of our study was to compare the safety and efficacy of laparoscopic Roux-en-Y gastric bypass(LRYGB)and sleeve gastrectomy(LSG)in patientsaged more than 55 years.We performed a retrospective review ofa prospectively collected database.Allpatients with body mass index(BMI)≥32 kg/m2and aged more than 55 years undergoing LRYGB or LSG in BMISurgery Centre,E-Da Hospitalbetween January 2008 and December2011 with atleastone year of follow up were included for the analysis.Demography,peri-operative data,weightloss and surgicalcomplications were allrecorded and analyzed.Mean age and BMIofthese 68 patients (22 malesand 46 female)were 58.8 years(55-79 years)and 39.5 kg/m2(32.00-60.40 kg/m2).LRYGB wasperformed in 44 patientsand LSG in 24 patients.The two groups were comparable in theirpreoperative BMI,American Society of Anaesthesia(ASA)score and gender distribution.LSG patients were significantly older than patients receiving LRYGB.The proportion of type 2 diabetes preoperatively was significantly higherin LRYGB patients as compared to LSG patients(88.63%vs.50%;P<0.01).The prevalence of other co-morbidities was similar and comparable between the groups.Mean BMI in the LRYGB and LSG groups at the end of 1 year were 28.8 kg/m2and 28.2 kg/m2,respectively,and there wasno statistically significantdifference in mean percentage ofexcessweightloss (%EWL)at1 year.The percentage ofresolution ofdiabeteswassignificantly higherin LRYGB(69.2%)ascompared to LSG(33.3%).On the otherhand,there wasno statisticaldifference in the percentage ofresolution ofhypertension, hyperlipidemia and fatty liverhepatitis.The overallmorbidity and re-operation rate washigherin LRYGBpatients.In morbidly elderly patients,both surgeriesachieved good weightlossand resolution ofcomorbidities.LRYGBissuperiorto LSG in terms ofdiabetes remission butcarries highercomplication rates even athigh volume centres.
obesity,metabolic surgery,Roux-en-Y gastric bypass,laparoscopic,sleeve gastrectomy,effiacy,safety
Introduction
Concurrent with the pandemic of obesity,we are experiencing a phenomenon of global ageing with a marked increase in the population of elderly obese people.Bariatric surgery has been proved as the most effective treatment of morbid obesity and associated co-morbidities.However,old age is still a relativecontraindication for bariatric surgery.Elderly patients have more associated co-morbidities>which give rise to a higher operative risk and postoperative complications.Previous studies have demonstrated a higher morbidity and mortality as well as decreased excess weight loss following bariatric surgery in older subjects[1].NIH consensus conference had setage ofmore than 55 years as the upper limitfor surgery[2].
Severalstudies have shown that,with the evolution and advance of minimally invasive surgery in recent few years,bariatric surgery in elderly patients achieved significant weight reduction and resolution of comorbidities[3,4,5].The improvement in surgical techniques and perioperative management has led to decreased morbidity,which is comparable to younger patients,especially in high volume centres with experienced surgeons[6].Laparoscopic Roux-en-Y gastric bypass(LRYGB)is the mostfrequently performed bariatric procedure,providing significantand sustained weightloss atlong-term follow-up and severalinvestigators have published their results regarding the safety and efficacy of LRYGB in older patients[7,8].
Laparoscopic sleeve gastrectomy(LSG),which was developed as the firststage of the BPD-DS(biliopancreatic diversion with duodenal switch)in high risk morbidly obese patients,has now been established as a standalone bariatric procedure.In a comparative study of LSG and LRYGB in the younger age group, the percentage of excess weight loss(%EWL)and comorbidity resolution was comparable for both procedures[9,10].Though a number of studies have demonstrated the safety and efficacy of various bariatric procedures in the elderly population,comparative data are stilllacking.The aim of our study was to compare the safety and efficacy of LRYGB and LSG in elderly patients aged more than 55 years.
Materials and methods
We performed a retrospective review of the prospectively collected database.All patients aged more than 55 years undergoing LRYGB or LSG in a high surgical volume centre,E-Da Hospital,between January 2008 and December 2011,with at leastone year of follow up were included for the analysis.The operative criteria were based on the Asia-Pacific guidelines for bariatric surgery,i.e.body mass index (BMI)≥32 kg/m2in the presence of comorbidities and BMI≥37 kg/m2with or without comorbidities. Allthe operationswere performed by the same surgical team.The patients received LRYGB or LSG according to our surgeonsˊsuggestion and their preference. Otherwise,surgeons intended to suggest LSG in older aged patient to avoid nutritional complications and suggest LRYGB in diabetic patients to expectbetter remission result of diabetes.Vitamin and mineral supplementation was prescribed to both LRYGB and LSG patients in a uniform manneraccording to the ASMBS Guidelines/Surgery for Obesity and Related Diseases 4 (2008)S73-S108[11].
Demographics of these patients included age,gender,body weight,BMI and American Society of Anaesthesia(ASA)score.The data regarding major comorbid illnesses,namely,diabetes mellitus,hypertension,hyperlipidaemia and fatty liver hepatitis,was recorded.The operative variables including the type of surgery,operative time,length of hospital stay, postoperative complications were recorded and analysed.Complications were classified according to the Bariatric Analysis and Reporting Outcome System (BAROS)as major and minor[12].The patient follow up visits were scheduled at 1,3,6,9 and 12 months following the surgery atwhich the BMIand percentage of EWL was calculated and the remission of comorbid illnesses was noted.Resolution of comorbidites was based on cessation of medicine taken and normalization of laboratory values.
Statistical analysis
Statistical analysis was done using the software packages SPSS,version 17(SPSS Inc.,Chicago,IL, USA).The continuous variables were expressed as mean and standard deviation and compared using Studentˊs t test while categorical variables were expressed as percentages and analysed using the Fischer exacttest.Allstatisticaltests were two tailed and P value of<0.05 was considered as statistically significant.
Results
A total of 68 patients aged more than 55 years between January 20 08 an d December 2011were included in this study.The mean age was 58.88 years (55-79 years)and the mean preoperative BMI was 39.5 kg/m2(32.00-60.40 kg/m2).There were 22 males and 46 female patients.LRYGB was performed in 44 patients and LSG in 24 patients.The two groups were comparable in their preoperative BMI,ASA score and gender distribution.The patients undergoing LSG were significantly older than LRYGB(Table 1).The percentage of associated type 2 diabetes preoperatively wa s significa ntly hig her in LRYGB pa tie nts as compared to LSG patients(88.63%vs.5 0%; P<0.01).However,there was no significantdifference in the mean duration of diabetes(80.3 vs.84 months;P=0.860),preoperative FBS(149.46 vs.132.3 mg/ dL;P=0.416),HbA1c(7.79 vs.7.86 gram%;P= 0.859)and C-peptide levels(3.32 vs.3.54;P= 0.709)between the two groups.The prevalence ofother co-morbidities was similar and comparable among the groups(Table 1).Mean BMIin the LRYGB and LSG groups at the end of 1 year were 28.8 kg/m2and 28.2 kg/m2,respectively;otherwise,there was no statistically significantdifference in mean%EWL at1 year between the two groups.The percentage of resolution of diabetes(Hb A1c<6.5%and FBS<100 mg/dl) was significantly higher in the LRYGB patients (69.2%)as compared to LSG patients(33.3%),P<0.001.The glycemia parameters and C-peptide levels were also lower after LRYGB than LSG,but did not reach a statistically significantlevel.Allthe comorbidities were significantly reduced afterboth operations one year postoperatively.Additionally,on comparison of resolution of other comorbidities among both groups, there was no statisticaldifference in percentage of resolution of hypertension(56%vs.60%;P=286),hyperlipidemia(81.2%vs.75%;P=0.792)and fatty liver hepatitis(76.9%vs.62.5%;P=0.347)(Table 2). Further analysing the relation of weight loss and the diabetic remission,we found thatthe diabetes remission group(DR)had a significantly higher%EWL compared with diabetes non remission group(DNR). Moreover,8 patients receiving LSG even reached 65.01%EWL in average;they stillcould notachieve remission ofdiabetes(Table 3).
The mean operative time was significantly higher in LRYGB than LSG(103.97 vs.70.04 minutes;P= 0.0015).However,there was no significantdifference in the mean length of hospital stay(2.54 vs.2.21 days;P=0.834).The overall morbidity and reoperation rate was 14.71%and 11.8%,respectively.It was 20.45%and 15.9%for LRYGB and 4.2%and 4.2%for LSG patients.There was only one mortality from gastrojejunostomy leakage in patients undergoing LRYGB.There was no statistically significantdifference in these parameters(Table 4).In the LRYGB group,there were 9 complications(6 early and 3 late), 7 of which required re-operation.Totally,3 patients (6.8%)had anastomotic leakage from gastrojejunostomy and all were repaired laproscopically.One of them developed a re-leak after repair,and progressed to septic shock and expired because of multi-organ failure after 30 days.Two patients(4.6%)developed intestinal obstruction.One patient had adhesions of the small bowel into the para-rectal space due to previous hysterectomy and was managed by adhesiolysis. The second patient had incarceration of the small bowel into the port site defect which required reduction of the small bowel and repair of the defect.One patient(2.3%)developed jejunojejunostomy stricture causing bilio-pancreatic limb obstruction,was relieved by gastrostomy,resection and re-do of the jejunojejunostomy stricture.
Of the late complications,2 patients(4.6%)developed gastrojejunostomy ulcer with a stricture.One patient responded well to endoscopic balloon dilatations and another required laparoscopic revision of gastrojejunostomy.One patient(2.3%)had a minor complication of marginal ulcer and responded toconservative treatment.Among the LSG group,only one patient developed adhesion induced stricture in incisura area of the stomach.On re-laparoscopy,it was relieved by adhesiolysis.
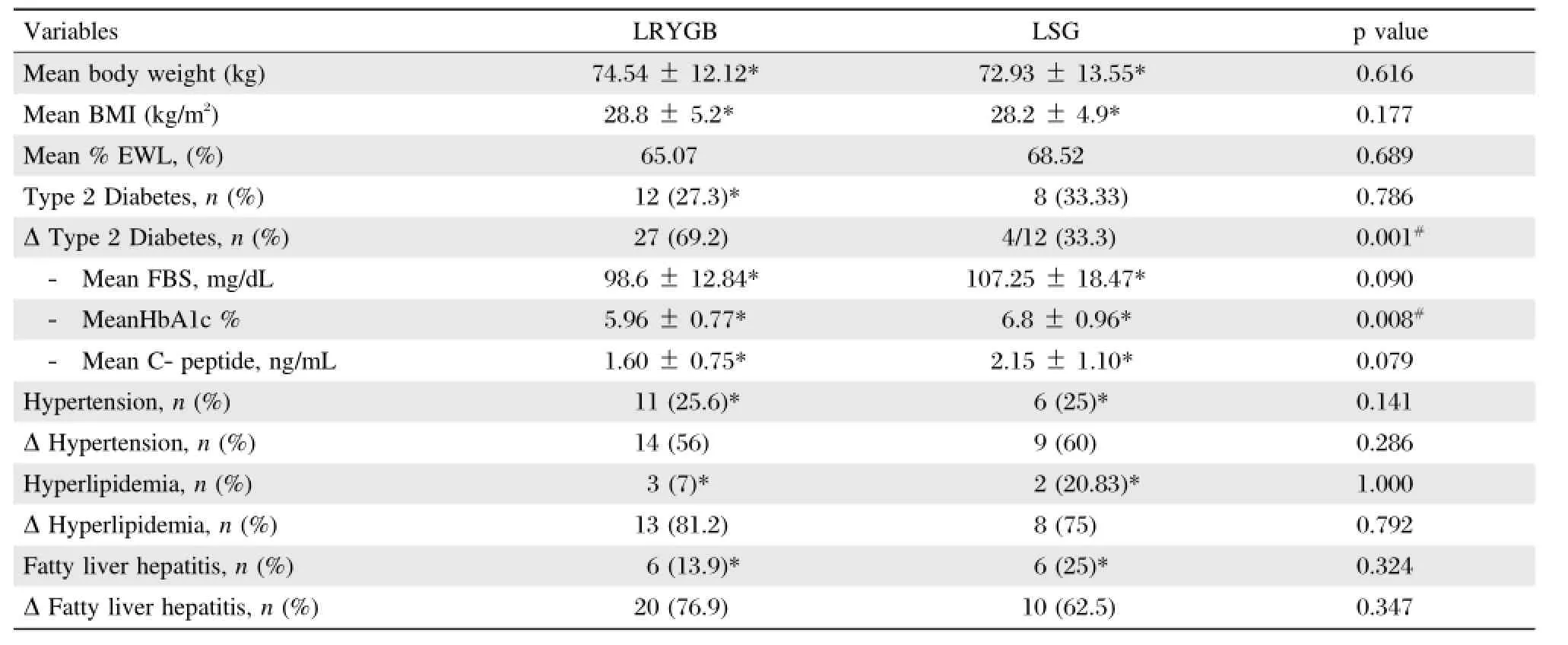
Table 2 Results of LRYGB vs.LSG at 1 year follow up
Discussion
The increased prevalence of obesity together with longer life expectancy brings more elderly obese patients requiring bariatric surgery now and in the future.The NIH guidelines which established age>55 years as a relative contraindication was based on earlier studies showing a high morbidity and mortality and decreased efficacy in older patients,particularly afteropen bariatric surgery[13].However,recentreports have demonstrated that laparoscopic bariatric surgery in old age is not only safe,but also very effective in remission of obesity associated disease and improvement in quality of life[14-16].Numerous comparative studies have demonstrated that the efficacy and safety of LRYGB in old age patients is similar to their younger counterparts[17,18].Reports on LSG in old age patientshave shown significant%EWL and comorbidity reduction,although comparative data with LRYGB are lacking[19].
In the presentstudy,we had 47%patients with ASA score 3 and 75%patients with diabetes,indicating less favourable operative risk profile in old age.In ourprevious study[20],the incidence of diabetes reported in young morbidly obese undergoing LRYGB with mean age of32.1 years was only 46%whereas in the present study 88.6%patients undergoing LRYGB were diabetic.This may contribute to the higher complication rates.Moreover,between procedures,LSGtruly has much fewer complication rates than LRYGB.Additionally, LSG is a technically less demanding procedure and required significantly less operative time than LRYGB. LSG proved to be equally effective as LRYGB forthe remission of old age comorbidities except diabetes.

Table 3 Correlation between%EWL and diabetes remission
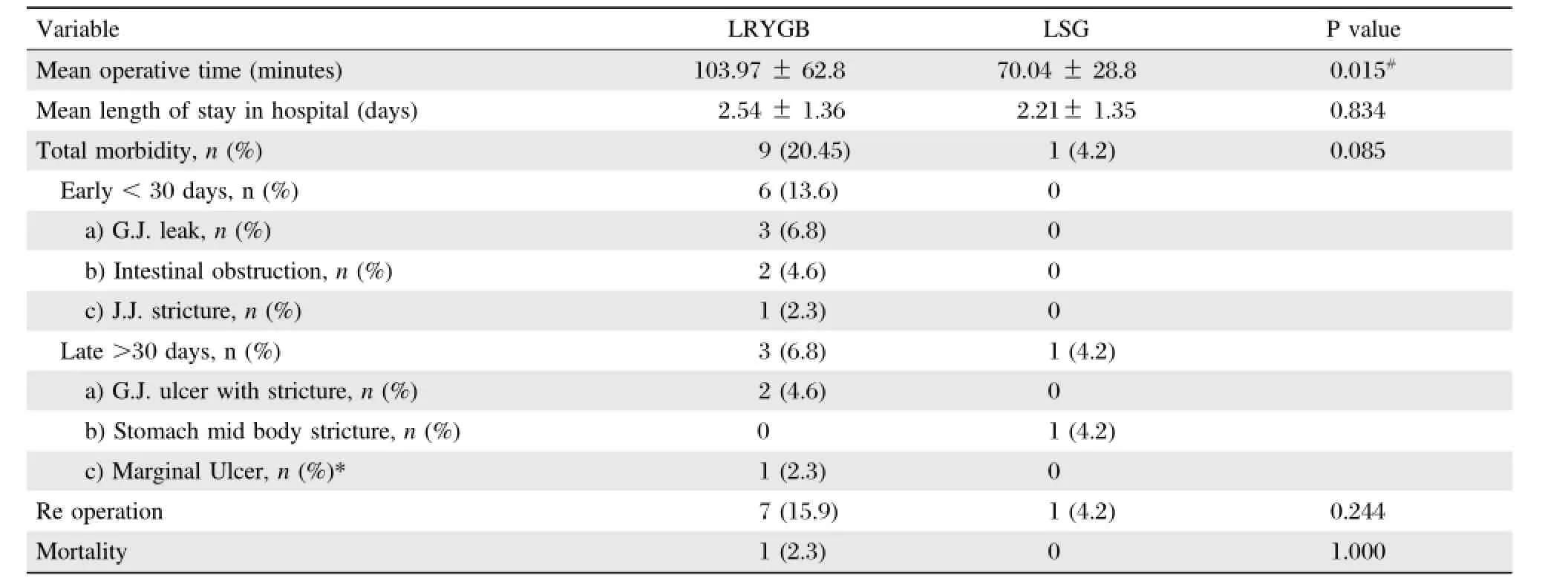
Table 4 Operative parameters and postoperative morbidity after LRYGB and LSG
Arthur in a cohort study of 9000 patients observed %EWL of 60%and 69%after LRYGB and LSG, respectively[21].Despite a comparable weight loss between our two study groups,diabetes remission was significantly higher after LRYGB than those who had LSG(Table 2).66.67%patients after LSG failed to getdiabetes remission despite of significant weightloss(65.01%).Jian-Fang Li[22]in his meta-analysis ofrandomized controlled trials also showed similar results.However,in contrastto our study,they reported higherweightlossafterLRYGB than LSGand concluded thatdifference in remission was related to the degree of weightloss.We also observed significantly betterweight loss in diabetes remission group when looking into individualprocedure(Table 3).Itrevealed thatweightlossis an important factor in remitting diabetes but also some other mechanism needed to be explored,such as the role of duodenal exclusion.Lower C-peptide level after LRYGBin our series seemed provoked the clues of better decreased insulin resistance compared with LSG.As Bikman and colleagues[23]found that improved insulin sensitivity after gastric bypass may be due to duodenal exclusion effect along with weight loss.
The patients undergoing LRYGB seemed to experience more complications,reoperations and mortality than LSG,although thisdifference did notreach statistical significance probably due to the limited sample size.Anastomotic leaks are the most dreaded and potentially devastating complication after LRYGB with a mortality rate of 6%-14.7%[24].The incidence of leak in our study is similar to the incidence rates reported in the literature,which range from 1.0%-5.6%[24].In our 3 GJ leak patients,2 of them were found to have chronic renal insufficiency or secondary Cushingˊs syndrome.Zeigler etal.[25]in their study of 5123 patients reported that preoperative steroid use led to increased rates of anastomotic leak in diabetic patients.He also found that diabetic patients who had an anastomotic leak had more than a 4-fold higher mortality compared with non diabetic patients.
In our study,2 patients developed intestinal obstruction.The reported incidence ofintestinalobstruction due to port site hernia mentioned in the previous studies ranges from 1%and 6%[26].In addition to raised intra-abdominalpressure in morbidly obese patients, lax and lowertone of abdominalmuscles may predispose them to developmentofportsite hernia in elderly patients[27].In our study,the incidence of GJ stricture was 4.6%;however,in the literature it is reported to range from 3 to 27%[28].Although,previous studies have suggested old age,hypertension,sleep apnoea and gastroesophageal reflux as the factors that are important in gastrojejunostomy stricture formation after LRYGB[30].However,ourpatients with gastrojejunostomy ulcer had no other predisposing factor exceptdiabetes and hypertension,which along with old age may have led to tissue ischaemia and ulcerformation.
Elderly patients have more associated comorbidities which may account for the higher surgical risk and increased postoperative morbidity,and these patients have much decreased physiologicalreserves to tolerate, resulting in increased mortality after such events. Livingston et al.[29]demonstrated a three times higher mortality for patients over the age of 55 years as compared to young patients.Otherwise,in a study of 71 obese patients of age>55 years receiving LRYGB, Papasavas et al.[30]reported perioperative morbidity and mortality of 16.8%and 1.4%,respectively.Flumetal.[31]reported a higher mortality rate of 4.8%.He concluded thatthe higherrisk is strongly associated with an older age,male gender and low volume centres.We observed an overallmortality rate of1.5%,which may be due to the factthatallprimary surgeriesand reoperations in ourcentre were undertaken by the laparoscopic approach,which may have contributed to a fasterrecovery.The rapid propagation of minimally invasive approach and comprehensive perioperative care would make bariatric surgery in elderly patients feasible and safer in the near future.
In presentstudy,though there wasselection bias that patients were not randomized to two different surgeries,this study is stillvery worthwhile because itis the first study to report the bariatric surgical result in old-age Asian patients,and showed good weight loss and comorbidity resolution after surgery.
In morbid elderly patients,both surgeries achieved good weight loss and resolution of comorbidities. LRYGB is superiorto LSG in terms ofdiabetes remission butcarries higher complication rates even athigh volume centres.
[1]Sugerman HJ,DeMaria EJ,Kellum JM,et al.Effects of bariatric surgery in older patients.Ann Surg 2004;240(2): 243-247.
[2]NIH Consensus Development Panel.Health implications of obesity.National Institutes of Health Consensus Development Conference Statement.Ann Int Med 1985; 103(6(Pt 2)):1073-1078.
[3]OˊKeefe KL,Kemmeter PR,Kemmeter KD.Bariatric surgery outcomes in patients aged 65 years and older at an American Society for Metabolic and Bariatric Surgery Center of Excellence.Obes Surg 2010;20(9): 1199-1205.
[4]Wittgrove AC,Martinez T.Laparoscopic gastric bypass in patients 60 years and older:early postoperative morbidity and resolution of comorbidities.Obes Surg 2009; 19(4):1472-1476.
[5]Livingston EH,Huerta S,Arthur D,etal.Male genderis a predictor of morbidity and age a predictor of mortality for patients undergoing gastric bypass surgery.Ann Surg 2002;236(5):576-582.
[6]Lynch J,Belgaumkar A.Bariatric surgery is effective and safe in patients over 55:a systematic review and metaanalysis.Obes Surg 2012;22(9):1507-1516.
[7]Dolores Frutos M,Lujan J,Hernandez Q,et al.Results of laparoscopic gastric bypass in patients>55 years old. Obes Surg 2006;16(4):461-464.
[8]Hazzan D,Chin EH,Steinhagen E,et al.Laparoscopic bariatric surgery can be safe for treatmentof morbid obesity in patients older than 60 years.Surg Obes Relat Dis 2006;2(6):613-616.
[9]Deitel M,Gagner M,Erickson AL,et al.Third international summit:Current status of sleeve gastrectomy. Surg Obes Relat Dis 2011;7(6):749-759.
[10]Hutter MM,Schirmer BD,Jones DB,et al.First report from the American Colleg e of Surgeons Bariatric Surgery Center Network:laparoscopic sleeve gastrectomy has morbidity and effectiveness positioned between the band an d the bypass.An n Su rg 201 1;2 54(3): 410-420.
[11]Linda Aills,Jeanne Blankenship,Cynthia Buffington, et al.ASMBS Allied Health Nutritional Guidelines for the Surgical Weight Loss Patient Allied Health Sciences Section Ad Hoc Nutrition Committee.Surg Obes Relat Dis 2008;4(5 Suppl):S73-S108.
[12]Oria HE,Moorehead MK.Bariatric analysis and reporting outcome system(BAROS).Obes Surg 1998;8(5):487-499.
[13]Printen KJ,Mason EE.Gastric bypass for morbid obesity in patients more than fifty years of age.Surg Gynecol Obstet 1977;144(2):192-194.
[14]Rand CSW,Macgregor AMC.Age,obesity surgery,and weight loss.Obes Surg 1991;1(1):47-49.
[15]Macgregor AMC,Rand CSW.Gastric surgery in morbid obesity:Outcome in patients aged 55 years and older. Arch Surg 1993;12810:1153-1157.
[16]Murr MM,Siadati MR,Sarr MG.Results of bariatric surgery for morbid obesity in patients older than 50 years. Obes Surg 1995;5(4):399-402.
[17]Sosa JL,Pombo H,Pallavicini H,et al.Laparoscopic gastric bypass beyond age 60.Obes Surg 2004;14(10): 1398-1401.
[18]Frutos MD,Lujan J,Hernandez Q,et al.Results of laparoscopic gastric bypass in Patients>or=55 Years Old.Obes Surg 2006;16(4):461-464.
[19]P.W.J.van Rutte Sleeve gastrectomy in older obese patients;Surg Endosc DOI 10.1007/s00464-012-2703-8
[20]Chen W,Chang CC,Chiu HC,et al.Use of individual surgeon versus surgicalteam approach:surgicaloutcomes of laparoscopic Roux-en-Y gastric bypass in an Asian Medical Center.Surg Obes Relat Dis 2012;8(2):214-219.
[21]Carlin AM,Zeni TM,English WJ,etal.The comparative effectiveness of sleeve gastrectomy,gastric bypass,and adjustable gastric banding procedures for the treatment of morbid obesity.Ann Surg 2013;257(5):791-797.
[22]Li JF,Lai DD,Ni B,et al.Comparison of laparoscopic Roux-en-Y gastric bypass with laparoscopic sleeve gastrectomy for morbid obesity or type 2 diabetes mellitus: a meta analysis of randomized controlled trials.Can J Surg 2013;56(6):E158-64.
[23]Bikman BT,Zheng D,Pories WJ,et al.Mechanism for improved insulin sensitivity after gastric bypass surgery. J Clin Endocrinol Metab 2008;93(12):4656-63.
[24]Carucci LR,Turner MA,Conklin RC,et al.Roux-en-Y gastric bypass surgery for morbid obesity:evaluation of postoperative extraluminal leaks with upper gastrointestinal series.Radiology 2006;238(1):119-127.
[25]Ziegler MA,Catto JA,Riggs TW,et al.Risk factors for anastomotic leak and mortality in diabetic patients undergoing colectomy:analysis from a statewide surgicalquality collaborative.Arch Surg 2012;147(9):819.
[26]Di Lorenzo N,Coscarella G,Lirosi F,et al.Port-site closure:a new problem,an old device.JSLS 2002;6(2): 181-183.
[27]Eid GM,Collins J.Application of a trocar wound closure system designed for laparoscopic procedures in morbidly obese patients.Obes Surg 2005;15(6):871-873.
[28]Blackstone RP,Rivera LA.Predicting stricture in morbidly obese patients undergoing laparoscopic Roux-en-Y gastric bypass:A logistic regression analysis.J Gastrointest Surg 2007;11(4):403-409.
[29]Livingsto n EH,Langert J.The impact o f age and Medicare status on bariatric surgical outcomes.Arch Surg 2006;141(11):1115-1120.
[30]Papasavas PK,Gagne DJ,Kelly J,et al.Laparoscopic Roux-en-y gastric bypass is a safe and effective operation for the treatment of morbid obesity in patients older than 55 years.Obes Surg 2004;14(8):1056-1061.
[31]Flum DR,Salem L,Elrod JA,etal.Early mortality among Medicare beneficiaries undergoing bariatric surgical procedures.JAMA 2005;294(15):1903-1908.
✉Corresponding author:Chih-Kun Huang,Bariatric&Metabolic International(B.M.I)Surgery Centre,E-Da Hospital,Kaohsiung, Taiwan,China,E-mail:dr.ckhuang@hotmail.com.
Received 19 July 2014,Revised 12 January 2015,Accepted 24 January 2015,Epub 05 March 2015
The authors reported no conflict of interests.
©2015 by the Journal of Biomedical Research.All rights reserved.
10.7555/JBR.29.20140108
 THE JOURNAL OF BIOMEDICAL RESEARCH2015年2期
THE JOURNAL OF BIOMEDICAL RESEARCH2015年2期
- THE JOURNAL OF BIOMEDICAL RESEARCH的其它文章
- Recent advances in bariatric/metabolic surgery:appraisalof clinical evidence
- Metabolic bariatric surgery and type 2 diabetes mellitus:an endocrinologistˊs perspective
- Roux-en-Y gastric bypass for Chinese type 2 diabetes mellitus patients with a BMI<28 kg/m2:a multi-institutionalstudy
- Maternalinheritance of severe hypertriglyceridemia impairs glucose metabolism in offspring
- Osthole inhibits proliferation of human breast cancer cells by inducing cell cycle arrest and apoptosis
- Quercetin attenuates the development of 7,12-dimethylbenz(a) anthracene(DMBA)and croton oil-induced skin cancer in mice