
Wallstent双支架重叠技术治疗复杂内脏动脉瘤五例
2014-06-09 14:20任建庄张萌帆张凯黄郭灏段旭华李腾飞韩新巍
介入放射学杂志 2014年12期
任建庄,张萌帆,张凯,黄郭灏,段旭华,李腾飞,韩新巍
·血管介入Vascular intervention·
Wallstent双支架重叠技术治疗复杂内脏动脉瘤五例
任建庄,张萌帆,张凯,黄郭灏,段旭华,李腾飞,韩新巍
目的初步评价Wallstent双支架重叠技术治疗复杂内脏动脉瘤的安全性和疗效。方法回顾性分析2012年3月至2013年11月连续收治的5例内脏动脉瘤患者,包括1例脾动脉起始部梭形动脉瘤、1例脾动脉中段囊状动脉瘤、1例腹腔干囊状动脉瘤、1例肝总动脉囊状动脉瘤、1例肠系膜上动脉宽颈动脉瘤。瘤体平均直径(23.0±8.7)mm。5例内脏动脉瘤均行Wallstent双支架重叠植入治疗,术后给予抗血小板药物治疗,术后6个月、1年、2年行CTA(computed tomographic angiography)检查,观察动脉瘤闭塞情况,支架、载瘤动脉和侧支血管和穿支动脉通畅情况。结果5例患者支架均成功植入,术后30 d内1例腹腔干动脉瘤患者出现轻微腹痛,给予止痛、扩血管药物等对症处理后1周后症状消失,余患者无其他手术相关并发症发生。5例患者术后随访6~24个月(平均13个月),动脉瘤均较前均缩小或消失。其中1例肝总动脉囊状动脉瘤患者术后6个月CTA显示支架内轻度狭窄(狭窄<25%)同时合并部分穿支动脉闭塞,但无明显临床症状,余患者支架、侧支血管和穿支动脉均通畅。结论Wallstent双支架重叠技术植入治疗复杂内脏动脉瘤具有较好的技术成功率和疗效,侧支血管和穿支动脉长期通畅率较高。
内脏动脉瘤;Wallstent;介入放射学
内脏动脉瘤(visceral artery aneurysms)在腹内动脉瘤中发病率次于主、髂动脉瘤,居第3位,常发生于腹腔干、肠系膜上、肠系膜下动脉及其分支。内脏动脉瘤的临床意义主要与其破裂风险有关,其破裂率约25%,破裂后患者病死率可达20%~75%[1-2]。近年来,随着介入放射学的发展,介入治疗在内脏动脉瘤的治疗中也越来越多地得到应用并逐渐成为主要的治疗方式。其中,弹簧圈栓塞和支架辅助弹簧圈栓塞由于具有较好的疗效已广泛应用。但对于部分复杂的动脉瘤,例如梭形或宽颈动脉瘤,由于操作技术难度较高以及较高的瘤颈再通率限制了其远期疗效[2]。近年来,多种密网孔支架逐步研发,因其网孔直径较小,金属覆盖率较普通金属裸支架高,能够有效地改变载瘤动脉和瘤腔内血流动力学因素,在封闭动脉瘤和重建载瘤动脉、保持侧支血管的开通方面展现出极大的优越性[3-4],国外文献已报道并得到初步的应用。采取双自膨式金属裸支架重叠置入能最大限度增加支架的金属覆盖率,进而缩小支架网眼,或可最大限度地模拟密网支架[5]。我科自2012年3月至2013年11月连续收治了5例复杂内脏动脉瘤患者,应用Wallstent双支架重叠技术对其进行治疗,取得了较好的疗效,现报道如下。
1 材料与方法
1.1 临床资料
回顾性分析我科自2012年3月至2013年11月连续收治的5例复杂内脏动脉瘤患者的临床和影像学资料。患者男3例,女2例,年龄39~73岁。动脉瘤平均直径(23.0±8.7)mm。5例内脏动脉瘤中,2例脾动脉瘤(1例脾动脉起始部梭形动脉瘤、1例脾动脉中段囊状动脉瘤),1例腹腔干囊状动脉瘤,1例肝总动脉囊状动脉瘤,1例肠系膜上动脉宽颈动脉瘤。5例内脏动脉瘤患者均为体检时发现,所有患者术前均行彩色多普勒超声和CTA检查证实并明确动脉瘤的大小、瘤颈及与载瘤动脉关系。1.2方法
1.2.1 操作技术5例患者经右侧股动脉穿刺插管,导丝配合下RH导管(Cook,USA)或Croba导管(Cook,USA)超选至载瘤动脉造影并进一步证实动脉瘤的大小、瘤颈、载瘤动脉直径及二者位置关系。而后交换7 F或8 F导引导管(Cook,USA)超选至载瘤动脉开口处,椎动脉导管(Codis,USA)或Croba导管(Cook,USA)配合260 cm泥鳅加硬导丝(Cook,USA)经导引导管跨越瘤颈至远端正常血管。根据血管直径、动脉瘤颈长短、及长度选择合适的Wallstent(Boston Scientific Corporation,USA)支架。沿导丝送入支架输送器及支架,使得支架成功跨越动脉瘤两端。再次经导引导管证实无误后释放。同样方法跨越第1枚支架放置第2枚支架。5例内脏动脉瘤共置入10枚支架,术中即刻造影显示支架管腔通畅、动脉瘤显影浅淡或基本不显影、穿支动脉未受累及(临床资料见表1)。
所有患者术前服用双联抗血小板聚集药物阿司匹林肠溶片300 mg/d、氯吡格雷75 mg/d,3 d;术中给予全身肝素化术后均给予低分子肝素40 mg,每12小时1次皮下注射至少72 h;术后继续给予双联抗血小板聚集药物6个月。

表1 动脉瘤发生部位和造影表现
1.2.2 随访方法所有患者术后3、6个月,1年和1年后每年行CTA(computed tomographic angiograph)检查,观察动脉瘤闭塞情况,支架和载瘤动脉以及穿支动脉通畅情况。
2 结果
2.1 近期(30 d)疗效
5例患者支架均成功植入,1例腹腔干动脉瘤患者术后出现轻微腹痛,给予止痛、扩血管药物等对症处理后1周后消失,无其他手术相关并发症发生。所有患者术后2周行CTA检查,无支架移位、夹层、无支架内血栓形成。5例患者30 d内无发生动脉瘤破裂和死亡等并发症。
2.2 中、远期疗效和并发症
5例内脏动脉瘤患者术后随访6~24个月(平均13个月),1例肝总动脉囊状动脉瘤患者术后6个月CTA显示支架内轻度狭窄(狭窄<25%)同时合并部分穿支动脉闭塞,但无明显临床症状。余患者动脉瘤较前均缩小或消失,支架、侧支血管和穿支动脉均通畅(图1、2)。所有患者随访过程中均未观察到药物相关出血并发症。
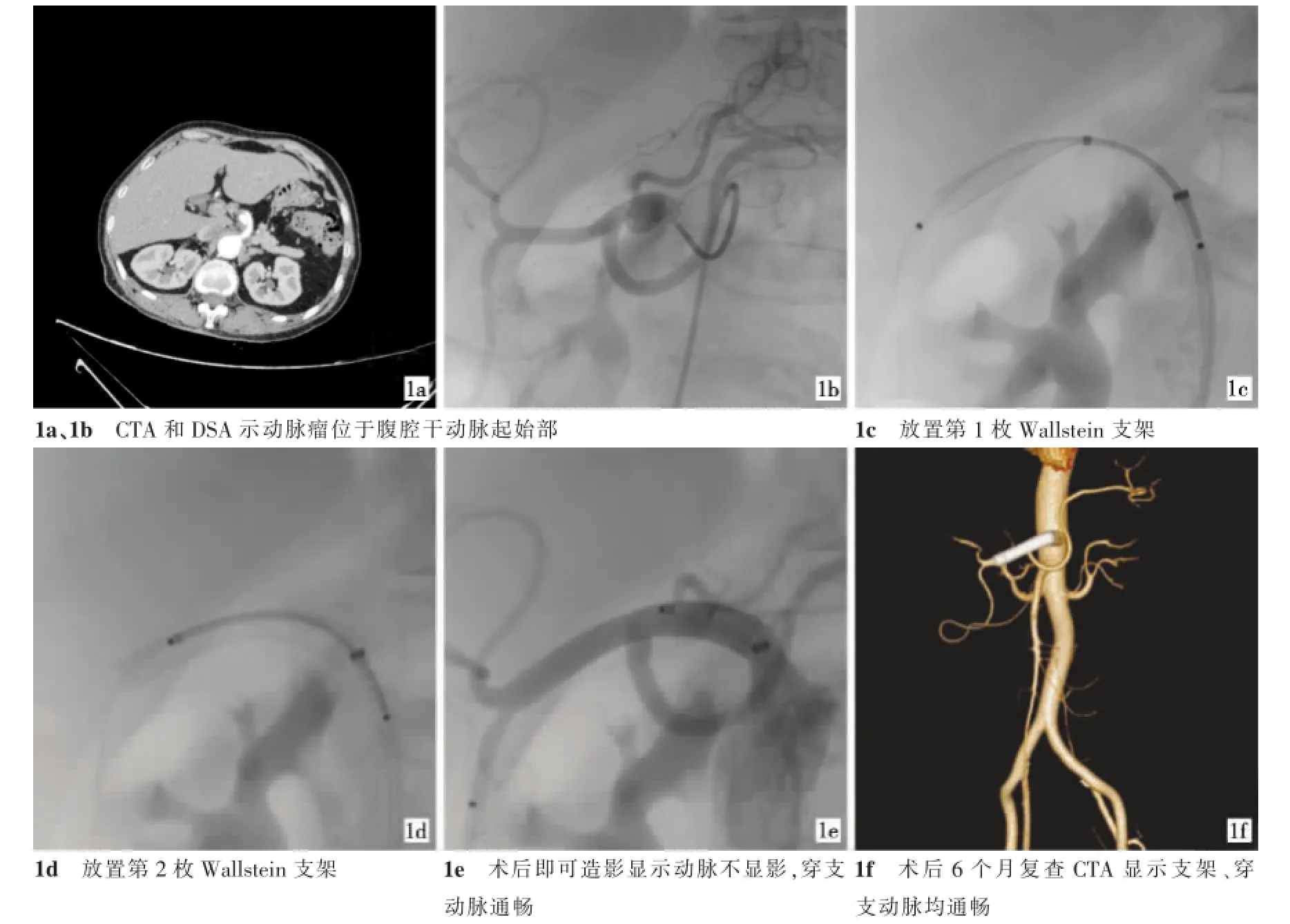
图1 腹腔干起始部动脉瘤治疗前后图像
3 讨论
内脏动脉瘤的病因目前尚不明确,可能与以下因素有关:动脉粥样硬化、动脉壁中膜退变/发育不良、腹部创伤、感染和炎性疾病、结缔组织病(Marfan综合征、Ehlers-Danlos综合征等)和高流量状态(门脉高压和妊娠等)[1,6-7]。由于其破裂率和病死率较高,需要积极的干预治疗。综合文献,适应证包括:动脉瘤破裂或患者有症状;动脉瘤直径大于20mm;动脉瘤直径每年至少增加5 mm;育龄期、妊娠以及接受原位肝移植患者;假性动脉瘤则一经发现,应积极干预[6-8]。
内脏动脉瘤介入治疗方式包括弹簧圈栓塞、支架植入和“Onyx胶”或微粒填塞、注射凝血酶,以及多种方式的配合。这些方法因效果显著又损伤较小而得到越来越多应用,其中弹簧圈直接栓塞以及支架辅助弹簧圈栓塞在内脏动脉瘤中的治疗较为常用[1,9-11]。弹簧圈直接栓塞动脉瘤,特别是瘤颈较宽的动脉瘤,部分病例远期可发生瘤颈再通;栓塞载瘤动脉流入段和流出段,适用于宽颈或梭形动脉瘤以及假性动脉瘤,但部分患者存在终端脏器坏死风险[12-13]。覆膜支架植入见于少量报道,理论上可以完全隔绝动脉瘤,但多数覆膜支架柔顺性较差,常受限于载瘤动脉的解剖因素,此外当内脏动脉瘤的载瘤动脉存在重要的侧支血管和穿支动脉时,不宜应用[3,14-15]。
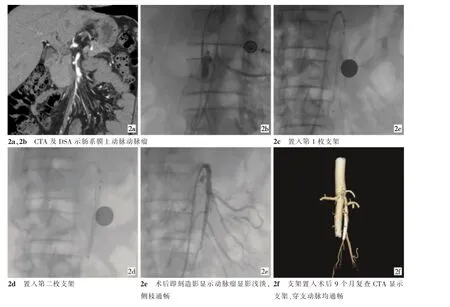
图2 肠系膜上动脉动脉瘤介入治疗前后图像
近年来,一种新的裸支架——密网孔支架,由于具有较好的血流导向功能已在动脉瘤的治疗中得到初步的应用。早期的金属裸支架主要目的是为了稳固弹簧圈,为提高支架的柔顺性多采用低金属覆盖率的大网孔设计。但Augsburger等[16]发现,高金属覆盖率的自膨式裸支架重叠植入后能将动脉瘤内血液流速降低48%~77%,进而提高瘤腔内血栓形成的概率。通过增加支架的金属覆盖率,缩小网眼,能够改变载瘤动脉和瘤腔血流动力学,减弱瘤腔血流量、涡流和血管壁剪切力,同时支架的“柵栏”作用可促进动脉瘤的内皮化,从而在修复和重建载瘤动脉的同时保持侧支血管的开通[3-4]。我科收治的5例复杂内脏动脉瘤共植入10枚Wallstent支架,术后造影显示动脉瘤显影浅淡或基本不显影,同时穿支动脉未受累及。1例腹腔干动脉瘤患者术后出现轻微腹痛,可能与支架置入后的血管痉挛有关,给予止痛、扩血管药物等对症处理后1周后消失。长期随访中,仅1例肝总动脉囊状动脉瘤患者术后6个月CTA显示支架内轻度狭窄(狭窄<25%)同时合并部分穿支动脉闭塞,但无明显临床症状,余患者无支架内血栓、狭窄等并发症,且随访中CTA图像上动脉瘤较前均缩小或消失,载瘤动脉侧支血管和穿支动脉都保持开通,疗效显著。
本组病例均应用闭环结构的Wallstent支架,相较于开环的Precise、Acculink等支架,Wallstent网眼较小但顺应性差,其优点是当支架部分释放时仍可回收并调整位置,且重叠植入后支架总体金属覆盖率较高,但其植入后膨胀过程中易缩短并撑直血管,可能导致迟发的动脉狭窄,临床应用中选用的支架长度至少应覆盖瘤颈两端超过1 cm,且支架直径应稍大于载瘤动脉内径,此外在成角或重度迂曲的载瘤动脉应用开环结构的支架或可减少操作技术难度[17-19]。尽管重叠的裸支架能够模拟血流导向支架的疗效,但Canton等[20]发现重叠植入的裸支架孔率(支架中网孔面积与总面积之比)的下降与血流动力学改变效能并非呈简单的线性关系,2枚以上金属裸支架的重叠置入能否更有效地改变血流动力学因素,尚无较多的证据支持。此外在急性动脉瘤破裂、部分巨大型和梭形动脉瘤中,应用弹簧圈辅助支架成形术或许是更为稳妥的选择[21]。
结合我们的经验,Wallstent双支架重叠植入治疗内脏动脉瘤具有较高的技术成功率,动脉瘤血栓形成和治愈率以及侧支血管和穿支动脉的长期开通率也满意。但由于样本量较少,其结果尚需要更大样本的研究证实。
[1]Balderi A,Antonietti A,Ferro L,et al.Endovascular treatment of visceral artery aneurysms and pseudoaneurysms:our experience[J].Radiol Med,2012,117:815-830.
[2]Koganemaru M,Abe T,Nonoshita M,et al.Follow-up of true visceral artery aneurysm after coil embolization by threedimensional contrast-enhanced Mr angiography[J].Diagn Interv Radiol,2014,20:129-135.
[3]杨鹏飞,刘建民,黄清海,等.新型血流导向装置Tubridge治疗颅内动脉瘤的初步经验[J].介入放射学杂志,2011,20: 357-362.
[4]Ruffino MA,Rabbia C,Italian Cardiatis Registry Investigators Group.Endovascular repair of peripheral and visceral aneurysms with the Cardiatis multilayer flow modulator:one-year results from the Italian Multicenter Registry[J].J Endovasc Ther,2012,19:599-610.
[5]Zhang L,Yin CP,Li HY,et al.Multiple overlapping bare stents for endovascular visceral aneurysm repair:a potential alternative endovascular strategy to multilayer stents[J].Ann Vasc Surg,2013,27:606-612.
[6]Cordova AC,Sumpio BE.Visceral artery aneurysms and Pseudoaneurysms-Should they all be managed by endovascular techniques?[J].Ann Vasc Dis,2013,6:687-693.
[7]ACC/AHA 2005 Practice Guidelines for the Management of Patients With Peripheral Arterial Disease(Lower Extremity,Renal,Mesenteric,and Abdominal Aortic)[J].Circulation,2006,113(11):e463-e465.
[8]Mohan IV,Stephen MS.Peripheral arterial aneurysms:open or endovascular surgery?[J].Prog Cardiovasc Dis,2013,56:36-56.
[9]Sakakibara K,Shindo S,Matsumoto M,et al.Splenic artery aneurysm of the hepatosplenomesenteric trunk[J].Ann Vasc Dis,2013,6:730-733.
[10]Kulkarni CB,Moorthy S,Pullara SK,et al.Endovascular treatment of aneurysm of splenic artery arising from splenomesentric trunk using stent graft[J].Korean J Radiol,2013,14:931-934.
[11]Cochennec F,Riga CV,Allaire E,et al.Contemporary management of splanchnic and renal artery aneurysms:results of endovascular compared with open surgery from two European vascular centers[J].Eur JVasc Endovasc Surg,2011,42:340-346.
[12]Tulsyan N,Kashyap VS,Greenberg RK,etal.The endovascular management of visceral artery aneurysms and pseudoaneurysms[J].JVasc Surg,2007,45:276-283;discussion 283.
[13]Ikeda O,Nakasone Y,Tamura Y,et al.Endovascular management of visceral artery pseudoaneurysms:transcatheter coil embolization using the isolation technique[J].Cardiovasc Intervent Radiol,2010,33:1128-1134.
[14]朱悦琦,李明华,方淳,等.应用Willis覆膜支架治疗脑池段动脉瘤的临床对照研究和长期随访结果[J].介入放射学杂志,2010,19:275-280.
[15]Sfyroeras GS,Dalainas I,Giannakopoulos TG,et al.Flowdiverting stents for the treatmentof arterial aneurysms[J].JVasc Surg,2012,56:839-846.
[16]Augsburger L,Farhat M,Reymond P,et al.Effect of flow diverter porosity on intraaneurysmal blood flow[J].Klin Neuroradiol,2009,19:204-214.
[17]Myouchin K,Takayama K,Taoka T,et al.Carotid wallstent placement difficulties encountered in carotid artery stenting[J]. Springerplus,2013,2:468.
[18]Müller-Hülsbeck S,Schäfer PJ,Charalambous N,et al. Comparison of carotid stents:an in-vitro experiment focusing on stent design[J].JEndovasc Ther,2009,16:168-177.
[19]Pierce DS,Rosero EB,Modrall JG,et al.Open-cell versus closed-cell stent design differences in blood flow velocities after carotid stenting[J].J Vasc Surg,2009,49:602-606;discussion 606.
[20]Canton G,Levy DI,Lasheras JC,et al.Flow changes caused by the sequential placement of stents across the neck of sidewall cerebral aneurysms[J].JNeurosurg,2005,103:891-902.
[21]Jeon P,Kim BM,Kim DI,et al.Reconstructive endovascular treatment of fusiform or ultrawide-neck circumferential aneurysmswithmultiple overlapping enterprise stents and coiling[J].AJNR,2012,33:965-971.
Safety and efficacy of dual-W allstent stenting in managing complicated visceral aneurysms:initial experience in 5 cases
REN Jian-zhuang,ZHANGMeng-fan,ZHANG Kai,HUANGGuo-hao,DUAN Xu- hua,LI Teng-fei,HAN Xin-wei.Department of Interventional Radiology,First Affiliated Hospital of Zhengzhou University,Zhengzhou,Henan Province 450052,China
REN Jianzhuang,E-mail:rjzjrk@126.com
ObjectiveTo evaluate the safety and efficacy of overlapped dual Wallstent stents technique in managing complicated visceral artery aneurysms.M ethods During the period from March 2012 to Nov.2013,5 patients with complicated visceral artery aneurysmswere admitted to authors’hospital.The lesions included fusiform aneurysm at the sp lenic arterial origin(n=1),sac-form aneurysm at themiddle segmentof splenic artery(n=1),sac-form aneurysm at celiac trunk artery(n=1),sac-form aneurysm at common hepatic artery(n=1)and wide-necked aneurysm of superiormesenteric artery(n=1).The clinical data and the imagingmaterialswere retrospectively analyzed.Themean diameter of the aneurysmswas(23± 8.7)mm.Overlapping stenting with 2Wallstent stents was carried out in all patients,and postoperative antiplatelet therapy was employed.CT angiography was performed at 6 months,one year and 2 years after the treatment to evaluate the obstruction condition of the aneurysms,the patency situation of the parent arteries,side branches and perforator arteries,etc.Results Stent implantation was successfully accomplished in all 5 cases.One patient with aneurysm at celiac trunk artery developed m ild abdominal pain 30 days after the treatment,which was relieved by administration of vasodilators and analgesic in 1 week.No procedure-related complications occurred in other patients.All the patients were followed up for 6-24months(mean of 13 months).Shrinkage or disappearance of aneurysms was observed in all the 5 cases.Asymptomaticmild in-stent stenosis(less than 25%)of parent artery and occlusion of several perforator arteries wereobserved in one patientwith sac-form aneurysm of common hepatic artery 6 months after the treatment.In the remaining patients the stents,side branches and perforator arteries remained patent.Conclusion For the treatment of complicated visceral artery aneurysms,overlapped dualWallstent stents technique has excellent efficacy and higher technical success rate,besides,long-term patency rate of side branches and perforator arteries is also very high.(J Intervent Radiol,2014,23:1036-1040)
visceral aneurysm;Wallstent;interventional radiology
R543.4
A
1008-794X(2014)-12-1036-05
2014-06-09)
(本文编辑:李欣)
10.3969/j.issn.1008-794X.2014.12.004
450052郑州大学第一附属医院介入放射科,郑州大学介入研究所,河南省介入治疗与临床研究中心
任建庄E-mail:rjzjrk@126.com
猜你喜欢
医学概论(2022年4期)2022-04-24
临床神经外科杂志(2021年6期)2021-07-02
散文诗世界(2019年6期)2019-09-10
中国临床医学影像杂志(2019年6期)2019-08-27
意林·全彩Color(2019年7期)2019-08-13
中国脑血管病杂志(2019年11期)2019-05-30
介入放射学杂志(2018年12期)2018-12-27
浙江医学(2018年4期)2018-02-28
恋爱婚姻家庭·养生版(2016年7期)2016-07-05
西南医科大学学报(2015年1期)2015-08-22
