
Ultrasonic diagnosis and vasoactive substances examination in patients with cirrhosis
2014-03-23 01:27:30MeiFanChunSuLinLuJunChangQinPeiLiJiaYingYuan
Mei Fan, Chun Su, Lin Lu, Jun-Chang Qin, Pei Li, Jia-Ying Yuan
1Department of Sonography, The First Affiliated Hospital of Zhengzhou University, Zhengzhou, China
2Department of Gynaecology and Obstetrics, the Fifth Affiliated Hospital of Zhengzhou University, Zhengzhou, China
3Department of Radiology, the Third Affiliated Hospital of Zhengzhou University, Zhengzhou, China
4Department of Pathophysiology, College of Basic Medical Sciences,Zhengzhou University,Zhengzhou,China
5Department of Sonography, the Affiliated Hospital of Henan Military Region, Zhengzhou, China
Ultrasonic diagnosis and vasoactive substances examination in patients with cirrhosis
Mei Fan1, Chun Su2, Lin Lu3, Jun-Chang Qin1, Pei Li4*, Jia-Ying Yuan5*
1Department of Sonography, The First Affiliated Hospital of Zhengzhou University, Zhengzhou, China
2Department of Gynaecology and Obstetrics, the Fifth Affiliated Hospital of Zhengzhou University, Zhengzhou, China
3Department of Radiology, the Third Affiliated Hospital of Zhengzhou University, Zhengzhou, China
4Department of Pathophysiology, College of Basic Medical Sciences,Zhengzhou University,Zhengzhou,China
5Department of Sonography, the Affiliated Hospital of Henan Military Region, Zhengzhou, China
Objective: To investigate hemodynamic change of patients with cirrhosis by using Color Doppler ultrasound technique and to explore the significance of change in the content of vasoactive substances-plasma endothelin-1 (ET-1) and calcitonin gene-related peptide (CGRP). Methods: A total of 178 cases with cirrhosis were regarded as study groups, and were divided into three degrees: A, B and C according to child-pugh and meanwhile 60 cases were regarded as normal control group. Portal vein and splenic vein of patients were explored by adopting Color Doppler ultrasound technique, related indexes were recorded and the blood flow as well as their ration in the two groups was calculated. Radio immunoassay was adopted to detect the content of plasma ET-1 and CGRP in both study group and contrast group. Results: Compared with the healthy cases in the contrast group, there was abnormal hemodynamics in the system of portal vein of patients with cirrhosis and the content of plasma ET-1 and CGRP was increased obviously. In the Child-Pugh liver function grades, the content of ET-1 and CGRP was increased as the degree of cirrhosis became more and more serious. There was no significant difference in the comparison between those without ascites and those in contrast group (P>0.05), the content of plasma ET-1 and CGRP in patients without ascites was increased remarkably. Besides, there was positive correlation between the content of plasma ET-1 and CGRP and Dpv, Dsv and Qsv. Conclusion: Detection of abnormal hemodynamics of portal vein and splenic vein by Color Doppler ultrasound technique can be one of the means for diagnosis of hypertension. Plasma ET-1 and CGRP of patients with cirrhosis reflect the serious degree of the damage in live function and play an important role in the formation and development of portal hypertension.
ARTICLE INFO
Article history:
Received 10 December 2013
Received in revised form 15 January 2014
Accepted 15 February 2014
Available online 20 April 2014
Cirrhosis
Color Doppler ultrasound technique
Venous hemodynamics
ET-1
CGRP
1. Introduction
Color Doppler ultrasound technique is a important way to diagnose cirrhosis and the standard of diagnosis of cirrhosis is that the diameters of the portal vein (PV) and splenic vein (SV) are respectively more than 13 mm and 8 mm[1]. Vasoactive substances mediate and participate in the formation of cirrhosis portal hypertension and the correlation between the content of vasoactive substances and cirrhosis as well as portal hemodynamics attracts a lot of attention[2]. Abnormal hemodynamics of cirrhosis is related to multiple vasoactive substances such as tumor necrosis factor, substance-P, vasoactive intestinal peptide, prostacyclin, endothelin (ET) and nitric oxide (NO) and so on[3]. Among these substances, ET is a kind of polypeptide consisting of 21 amino acids with a strong function of vascular contraction. ET-1 is synthesized by vascular endothelial cells[4] and plays an important biological role in liver and the portal system. The application of ET receptor antagonists can reduce the portal pressure[5]. Calcitonin gene-related peptide (CGRP) and calcitonin (Cal) come from a same gene and CGRP, consisting of 37 amino acids, isa kind of vasoactive peptide and can dilate the peripheral vessel remarkably[6]. Hemodynamic change of parameters in liver of patients with cirrhosis was detected by Color Doppler ultrasound technique and the change in the contents of vasoactive substances ET-1 and CGRP was checked by radioimmanoassay.
2. Materials and Methods
2.1. General Materials
A total of 178 patients who came to our hospital during Sep. 2009 to Sep. 2011 and were diagnosed with cirrhosis were chosen as study group, among whom there were 128 male cases and 50 female cases in the range of age 20-62 years old with the average age of (37.8±17.5) years. According to child-pugh grade of liver function, there were 55 cases with grade A, 89 cases with grade B and 34 cases with grade C. There were 106 cases with ascites and 72 cases without ascites. There were 144 cases with hepatitis cirrhosis, 13 cases with schistosomiasis cirrhosis, 8 cases with alcoholic cirrhosis and 13 cases with mixed cirrhosis. A total of 60 healthy persons were chosen as control group and they matched with the study group in terms of characters such as age fabric.
2.2. Ultrasonic diagnosis
Cases should be on fasting for 12 h before examination and be in resting in supine position. Toshiba Aplio500 Color Doppler ultrasound diagnostic apparatus was used with probe frequency 2.5-4.0 MHz to measure the diameter of portal vein (Dpv), velocity of portal vein (Vpv), diameter of splenic vein (Dsv), velocity of splenic vein (Vsv), quantity of portal vein (Qpv), quantity of splenic vein (Qsv). The calculation formula of venous quantity was Q=Vmin×(D/2)2×π×60 (Q was short for blood quantity, D symbolized the diameter of portal vein and Vmin symbolized the average velocity of blood).
2.3. Detection of vasoactive substances in serum
After cases who received examination finished their fast of 12 h, 8 mL blood was collected from them with empty stomach in the morning. And 4 mL was sent to be checked for liver function and the rest was divided into halves, stored in two test tubes respectively. Each tube contained 0.3 M anticoagulant EDTA-Na2 20 μL, 0.32 M dimercaprol dimercaptopropanol 10 μL and 0.34 M 8- hydroxyquinoline sulfate 20 μL. After they were fully mixed, the solution was centrifugal for 10 min at 2 000 rpm. The separated plasma was kept at -20 ℃ to detect ET-1 and CGRP. Radioimmunoassay kits of ET-1 and CGRP were bought from Beijing S & P Weiye Biological Technology Co. Ltd. and the operations were strictly under the guidance of instructions.
2.4. Statistical analysis
Software MATLAB 7.0 was used to analyze the statistics. Measurement data were symbolized by the means±standard deviations. The comparison of the differences in means of different samples was analyzed by variance and checked byt, regarding α=0.05 as checking standard. The difference was statistically meaningful when P<0.05.
3. Results
3.1. Results of color Doppler ultrasound diagnosis
Considering the final analyzed results, the Dpv and Dsv was wider than that in healthy group (P<0.05), Vsv was increased but the difference was not significant (P>0.05), Qsv was increased significantly (P<0.01) and the value of Qsv/Qpv was significantly larger than that in control group. From the perspective of Child-Pugh grade of liver function which reflected the degree of cirrhosis, in an ascending order A, B and C, Dpv and Dsv were increased gradually and there was significantly difference between adjacent groups (P<0.05). Vpv was gradually decreased (P<0.05). The change of Vsv in different groups wasn’t significant (P>0.05). The difference of Qpv between adjacent groups wasn’t significant either (P>0.05). Qsv was significantly in a increasing trend (P<0.01) and so it was same with the value of Qsv/Qpv, and the differences among groups were significantly (P<0.01) (Table 1).
3.2. Detection of ET-1 and CGRP
Radioimmunoassay was used to detect the content of ET-1 and CGRP in serum. The results showed the levels of them in study group were significantly higher than that in control group (P<0.01), the levels of them in group with ascites were significantly higher than that in group without ascites (P<0.05 or P<0.01). The difference between the levels of ET-1 and CGRP in group without ascites and that in control group wasn’t significant (P>0.05) (Table 2).
3.3. Relation between the degree of damage to liver function and the levels of ET-1 and CGRP in plasma
The detected results showed that there was no significantdifference between the levels of ET-1 and CGRP in group with liver function damage in grade A and that in control group (P>0.05) and there were significant differences among groups with liver function damage in groups with grade A, B and C (P<0.05). The levels of ET-1 and CGRP increased significantly as the damage to liver function aggravated (Table 3).

Table 1 Index results of hemodynamics of portal and splenic vein by color doppler ultrasound diagnosis.

Table 2 Expression level of ET-1 and CGRP in serum (ng/L).
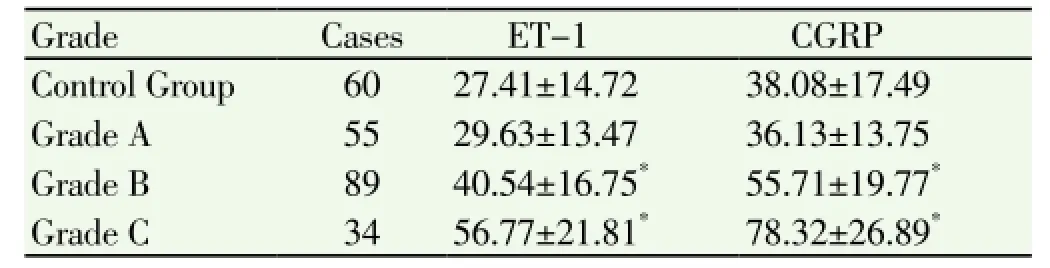
Table 3 Levels of ET-1 and CGRP in plasma of patients in different Child-Pugh Grades (ng/L).
3.4. Relation between levels of ET-1 and CGRP and venous hemodynamics of patients with cirrhosis
The levels of ET-1 and CGRP were in positive relation to the diameters of portal and splenic veins and quantity of splenic vein. The difference was statistically significant (P<0.01) (Table 4).

Table 4 Analysis of relation between vasoactive substances and hemodynamics of venous system.
4. Discussions
Hemodynamics in human body can change abnormally in the process of cirrhosis and such a change is relevant with two currently popular hypotheses-hypothesis of backward flow and hypothesis of forward flow[8, 9], both of which play an important role in the formation of cirrhosis portal hypertension[10,11]. So far, as to the measure of the blood flow of portal venous system, Color Doppler detection is of large value. In the study, through the detection of hemodynamics of portal vein by Color Doppler technique, it was found that as the Child-Pugh integral of liver function increased, the diameters of portal and splenic veins had the trend to dilate gradually while the blood flow in portal vein slowed down gradually and there were significantly differences in the degree of dilation among grade A, B and C. This is not totally same with the research results by Liu Mingtao and his colleagues[12]. In their study, they found that there were no remarkable differences in the degree of dilation of portal veins among grade A, B and C. Given the results that the values of Qsv/Qpv in group with cirrhosis in different grades were all higher than that in control group, the increase of blood flow in splenic vein plays an important role in the formation of portal hypertension of patients with cirrhosis. Therefore, the change in hemodynamics can be the index to assess the degree of hepatic parenchymal lesions as well as the effective index to diagnose portal hypertension[13,14].
Some studies showed that the level of plasma ET-1 in patients with cirrhosis increased remarkably[15,16]. Our study results also indicated that the level of plasma ET-1 grew remarkably with the increase of child-pugh grade (P<0.05), suggesting that the level of plasma ET-1 was related to the serious degree of cirrhosis-growing gradually with the aggravation of the damage in liver function. The increase of ET-1 in patients with cirrhosis can raise the intra-hepatic vascular resistance and the portal pressure[17,18]. The level of plasma ET-1 is significantly related to the diameters of portal and splenic vein, indicating that it plays a certain role in the formation of portal hypertension. In addition, the studyfound that the level of CGRP is similar to that of ET-1 and the content in patients with cirrhosis is obviously higher than that in control group. The increase of CGRP may contribute to hyper-dynamic circulatory state, resulting in the increase of splanchnic blood flow and portal pressure[19]. The dilation of peripheral vessel and the abnormal distribution of blood volume lead to water-sodium retention, which is consistent with related reports[20,21]. The result that the level of ET-1 and CGRP in patients with ascites is remarkably higher than that in cases without ascites indicates that high ET-1 and CGRP levels in patients with cirrhosis can lead to ascites through the dilation of peripheral vessels or the increase f portal pressure. Meanwhile, the level of CGRP is also related to the Child-Pugh grades of liver function. The above results show that ET-1 and CGRP may participate in the formation and maintenance of cirrhosis portal hypertension at the same time.
Conflict of interest statement
We declare that we have no conflict of interest.
[1] Plestina S, Pulanić R,Kralik M, Samarzija M. Color Doppler ultrasonography is reliable in assessing the risk of esophageal variceal bleeding in patients with liver cirrhosis. Wien Klin Wochenschr 2005; 117(19-20): 711-717.
[2] Malvasi A, Tinelli A, Cavallotti C, Morroni M, Tsin DA, Nezhat C, et al. Substance P (SP) and vasoactive intestinal polypeptide (VIP) in the lower uterine segment in first and repeated cesarean sections. Peptides 2010; 31(11): 2052-2059.
[3] Laleman W. Role of vasoactive substances and cellular effectors in the pathophysiology of cirrhotic portal hypertension:the past,the present and the future-Geores Brohee lecture. Acta Gastroenterol Belg 2009; 72(1): 9-16.
[4] Zhu HJ, Lu S, Su W, Gong SY, Zhang ZB, Li P, et al. Effect of Liandouqingmai Recipe on life quality and vascular endothelial injury in patients wirh coronary heart disease. J Trad Chin Med 2012; 32(4): 529-533.
[5] Takashimizu S, Kojima S, Nishizaki Y, Kagawa T, Shiraishi K, Mine T, et al. Effect of endothelin A receptor antagonist on hepatic hemodynamics in cirrhotic rats. Implications for endothelin-1 in portal hypertension. Tokai J Exp Clin Med 2011; 36(2): 37-43.
[6] Durham PL. Calcitonin gene-related peptide (CGRP) and migraine. Headache 2006; 46(Suppl 1): S3-S8.
[7] Brockmöller J, Thomsen T, Wittstock M, Coupez R, Lochs H, Roots I. Pharmacokinetics of levetiracetam in patients with moderate to severe liver cirrhosis (Child-Pugh classes A,B,and C): characterization by dynamic liver function tests. Clin Pharmacol Ther 2005; 77(6): 529-541.
[8] Heffernan KS, Yoon ES, Sharman JE, Kim EJ, Jung SJ, Jae SY. Resistance exercise training reduces arterial reservoir pressure in older adults with prehypertension and hypertension. Hypertens Res 2013; 36(5): 422-427.
[9] Tan YW, Yu XJ, Yin YM. Clinical significance examining the portal system hemodynamics of portal hypertension in patients with cirrhosis by color Doppler ultrasound. Chin J Ultrasonography 2001; 10(3): 151-153.
[10] Ramazan K, Ibrahim K, Ahmet A, Tamer B, Ahmet S, Alpay A, et al. Quantitative Doppler evaluation of the splenoportal venous system in various stages of cirrhosis: difference between right and left portal veins. J Clin Ultrasound 2002; 30(9): 537-543.
[11] Katsuta Y, Zhang XJ, Ohsuga M, Akimoto T, Komeichi H, Shimizu S, et al. Hemodynamic features of advanced cirrhosis due to chronic bile duct ligation. J Nippon Med Sch 2005; 72(4): 217-225.
[12] Liu MT, Han GH, Wang JH, Wu KC, Fan DM. Study on the relationship between portal vein pressure and portal hemodynamics in patients with portal hypertension of cirrhosis. Chin J Hepatol 2004; 12(8): 504-505.
[13] Yan GZ, Duan Y, Ruan LT, Cao TS, Yuan LJ, Yang YL. Noninvasive quantitative testing of liver function using ultrasonography in patients with cirrhosis. Hepato Gastro Enterol 2006; 53(67): 15-20.
[14] Vogt W. Value of ultrasound and Doppler sonography in chronic hepatitis and liver cirrhosis. Schweiz Rundsch Med Prax 2005; 94(16): 639-643.
[15] Uehara H, Akahoshi T, Kawanaka H, Hashimoto N, Nagao Y, Tomikawa M, et al. Endothelin-1 derived from spleen-activated Rho-kinase pathway in rats with secondary biliary cirrhosis. Hepatol Res 2012; 42(10): 1039-1047.
[16] Tsiakalos A, Hatzis G, Moyssakis I, Karatzaferis A, Ziakas PD, Tzelepis GE. Portopulmonary hypertension and serum endothelin levels in hospitalized patients with cirrhosis.Hepatobiliary Pancreat Dis Int 2011; 10(4): 393-398.
[17] Zhai Y, Zhang J, Shang HW, Lu SC,Wang ML,You H, et al. Octreotide decreases portal pressure: Hepatic stellate cells may play a pivotal role. African J Biotechnol 2010; 9(12): 1833-1838.
[18] Rockey DC, Weisiger RA. Endothelin induced contractility of stellate cells from normal and cirrhotic rat liver: implications for regulation of portal pressure and resistance. Hepatology 1996; 24(1): 233.
[19] Blanco-Rivero J, Márquez-Rodas I, Sastre E, Cogolludo A., Pérez-Vizcaíno F, del Campo L, et al. Cirrhosis decreases vasoconstrictor response to electrical field stimulation in rat mesenteric artery:role of calcitonin gene-related peptide. Exp Physiol 2011; 96: 275-286.
[20] Gattinoni L, Carlesso E.Supporting hemodynamics: what should we target ? What treatments should we use? Crit Care 2013; 17(Suppl 1): S4.
[21] Han GH, Yan Y. Level changes of endothelin-1 (ET 1) and calcitonin gene related peptide (CGRP) in patients with cirrhosis. Chin J Gerontol 2006; 8: 1023.
ment heading
10.1016/S1995-7645(14)60050-X
*Corresponding author: Pei Li, M.D. Basic Medical College of Zhengzhou University, Zhengzhou, China.
Jia-Ying Yuan, M.M., Department of Ultrasonography, Directly Affiliated Hospital of Henan Military Area, Zhengzhou 450003, Henan Province,China.
E-mail: peter_mails@126.com
Foundation project: The paper is supported by a grant of New Century Excellent Talents in University,Ministry of Education China(No.NCET-11-0949)
 Asian Pacific Journal of Tropical Medicine2014年4期
Asian Pacific Journal of Tropical Medicine2014年4期
- Asian Pacific Journal of Tropical Medicine的其它文章
- Effect of bone marrow mesenchymal stem cells on the Smad expression of hepatic fibrosis rats
- Correlation of expression of STAT3, VEGF and differentiation of Th17 cells in psoriasis vulgaris of guinea pig
- Effect of anesthesia on cognitive status and MMP-2 expression in rats
- Effect of low intensity pulsed ultrasound on repairing the periodontal bone of Beagle canines
- Effect of RSCs combined with COP-1 on optic nerve damage in glaucoma rat model
- Expression of PI3-K, PKB and GSK-3β in the skeletal muscle tissue of gestational diabetes mellitus