胃旁路术与胆胰转流术治疗2型糖尿病机制的研究
2011-11-22 01:26:45狄建忠韩晓东张宏玮杜贻豹汪昱郑起张频
中华胰腺病杂志 2011年5期
狄建忠 韩晓东 张宏玮 杜贻豹 汪昱 郑起 张频
·论著·
胃旁路术与胆胰转流术治疗2型糖尿病机制的研究
狄建忠 韩晓东 张宏玮 杜贻豹 汪昱 郑起 张频
目的比较胃旁路术(GBP)与胆胰转流术(BPD)对非胰岛素依赖性糖尿病大鼠的治疗效果,探讨其机制。方法40只糖尿病GK大鼠按数字表法随机分为GBP组、BPD组、饮食控制组和对照组,每组10只。GBP组、BPD组分别行GBP及BPD手术;饮食控制组大鼠每天给予基础饲料15 g,自由进水;对照组不限食量。记录手术时间、死亡率。每周测空腹体重。检测治疗前及治疗后1、2、3、4、8、16周的空腹血糖、瘦素、胰岛素样生长因子-1(IGF-1)水平。结果GBP组平均手术时间为(25±4)min,BPD组为(35±6)min;GBP组大鼠死亡1只,BPD组死亡3只,两组差异均有统计学意义(P值均<0.01)。治疗前各组大鼠血糖、瘦素及IGF-1水平无统计学差异。治疗后对照组大鼠血糖及瘦素均无明显变化。饮食控制组大鼠治疗后2周起血糖及瘦素水平开始下降,第4周时显著降低,并持续至16周(P<0.05),但血IGF-1水平无明显变化。GBP组与BPD组大鼠治疗后2周起血糖及瘦素水平开始下降,而血IGF-1水平开始升高,并持续至16周[血糖:(6.8±1.0)、(6.3±0.8)mmol/L比(13.9±2.6)、(14.1±2.4)mmol/L;瘦素:(16.1±3.3)、(17.2±3.2)pg/ml比(29.4±3.9)、(29.4±3.9)pg/ml ;IGF-1:(166.1±8.3)、(142.2±8.2)ng/L比(119.4±8.8)、(109.8±7.9)ng/L,P值均<0.01],但这两组的血糖及瘦素水平无统计学差异;而GBP组大鼠血IGF-1水平较BPD组升高更显著(P<0.05)。结论GBP和BPD均能较好地控制糖尿病大鼠的血糖水平,其机制可能与瘦素的降低及IGF-1的升高有关。GBP在手术时间、死亡率及增加血IGF-1水平等方面优于BPD。
糖尿病,2型; 胃旁路术; 胆胰转流术
糖尿病是严重危害人类健康的慢性疾病,全球患者在1.5亿以上,且患病率逐年增加,其中2型糖尿病(T2DM)占85%左右。近年来国外对病理性肥胖症手术治疗的临床资料分析发现,治疗病理性肥胖症的胃转流术(gastric bypass,GBP)和胆胰转流术(biliopancretic diversion,BPD)对并存的T2DM治愈率达83%~86%,对并存的高血压病治愈率达66%~69%,为T2DM治疗提供一种全新方法。而有关GBP与BPD降糖效果及机制的基础研究甚少。本研究比较二种术式对雄性Goto-Kakizaki大鼠糖尿病模型的降糖效果,探讨其机制。
材料和方法
一、动物模型制备及分组
40只健康清洁级糖尿病GK大鼠购于上海斯莱克实验动物有限责任公司,适应性饲养1周。按数字表法随机分为GBP组、BPD组、饮食控制组和对照组,每组10只。GBP组和BPD组大鼠术前禁食不禁水24 h,0.5%戊巴比妥钠(50 mg/kg)腹腔内注射麻醉后上腹正中切口进腹。GBP组大鼠在贲门下方弧形切断胃近端形成20%小胃囊,封闭远端胃,距Treitz韧带10 cm处切断空肠,远端与近端小胃囊吻合,距胃肠吻合口远端20 cm处行空肠侧侧吻合。BPD组大鼠切除远端胃,封闭十二指肠盲端,在距回盲瓣2.5 cm处切断小肠,保留的20%残胃与远端小肠吻合,近端空肠在距回盲瓣20 cm处与回肠吻合。两组大鼠术后禁食6 h,不禁水,术后24 h自由进基础饲料。饮食控制组大鼠每天给予基础饲料15 g,自由进水。对照组大鼠自由进食基础饲料,自由进水。每周测空腹体重。
二、检测指标
1.血糖:术前及术后1、2、3、4、8、16周晨8:00抽取尾静脉血1.5 ml,置入加有DPPIV inhibitor 209l的EDPA抗凝冰冷真空管中,立即4℃ 4000 r/min离心10 min,取血浆,置-70℃保存。应用强生One Touch Ultra血糖仪测定空腹血糖。
2.血瘦素:应用血浆瘦素放免测定盒(北京北方生物技术研究所)测定血浆瘦素含量,由上海交通大学医学院放免中心按说明书操作。
3.血胰岛素样生长因子-1(IGF-1):应用IGF-1放免测定盒(北京北方生物技术研究所)测定血浆瘦素含量,由上海交通大学医学院放免中心按说明书操作。
三、统计学分析
结 果
一、一般情况
GBP组平均手术时间为(25±4)min,BPD组为(35±6)min,两组差异有统计学意义(P<0.01)。GBP组大鼠死亡1只,BPD组死亡3只,差异亦有统计学意义(P<0.01)。
GBP组、BPD组、饮食控制组大鼠治疗后1周体重均较对照组明显下降(P<0.01)。治疗后2周起饮食控制组大鼠体重始终明显低于GBP组、BPD组及对照组(P<0.05)。治疗后2周起GBP组与BPD组大鼠体重逐渐恢复,4周后体重与对照组无明显差异,而GBP组和BPD组大鼠体重在各时间点的差异均无统计学意义(图1)。
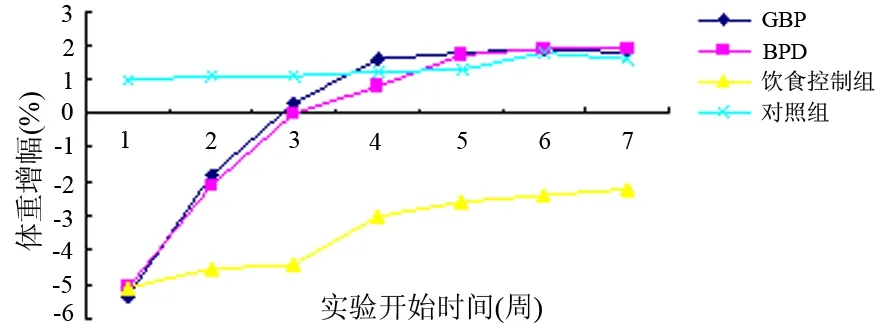
图1 各组大鼠体重的变化
二、大鼠空腹血糖、瘦素及IGF-1的变化
术前各组大鼠血糖、瘦素及IGF-1水平无统计学差异。对照组大鼠治疗后空腹血糖及瘦素无明显变化。饮食控制组大鼠治疗后2周起血糖及瘦素水平开始下降,第4周较治疗前显著降低,并持续至16周(P<0.05),但治疗后血IGF-1水平无明显变化。GBP组与BPD组大鼠治疗后2周起血糖及瘦素水平开始下降,而血IGF-1水平开始升高,治疗第4周起与治疗前比较有统计学差异,并持续至16周(P值均<0.01)。治疗后4周起GBP组与BPD组大鼠血糖及瘦素水平较饮食控制组显著降低(P值均<0.05),但GBP组与BPD组间差异无统计学意义(表1)。而GBP组大鼠血IGF-1水平从治疗后4周起较BPD组升高更显著(P<0.05,表1)。

表1 各组大鼠空腹血糖、瘦素及IGF-1的变化
注:与治疗前比较,aP<0.05,bP<0.01;与饮食控制组比较,cP<0.05;与BPD组比较,dP<0.05
讨 论
GBP与BPD都是有效的减肥手术[1]。总结其减肥效果的回顾性分析时发现其能治疗或治愈2型糖尿病,但其确切机制至今尚不明确,各种外科手术疗效及风险未得到系统评估,对适应证的把握也有分歧,故限制了外科手术治疗T2DM的推广应用进程。
本研究应用GBP与BPD两种术式治疗T2DM大鼠,术后第2周血糖开始下降,术后4周较对照组显著降低,并持续下降至16周,说明GBP与BPD均能有效控制T2DM大鼠的血糖。GBP与BPD二种术式的降糖效果均无统计学差异,提示2种手术的疗效无差异。而饮食控制组在4周内血糖明显下降,此后未进一步下降,说明饮食控制不能将血糖控制到理想的水平。
研究认为,体重减轻对糖尿病特别是伴肥胖症者血糖控制有重要作用。它可以引起肌肉内胰岛素受体表达增加和脂连素水平增高,反过来增加胰岛素敏感性,从而改善B细胞的功能[2]。本结果显示,转流组大鼠术后血糖下降均明显,但体重无明显下降,显示进食量减少及体重减轻不是转流术治疗T2DM的根本所在。
研究证实,瘦素、IGF-1与T2DM的发生、进展关系密切[3-5]。本研究GBP与BPD组术后空腹血浆瘦素变化与术后血糖变化趋势相似,说明术后瘦素水平的下降可能与血糖的降低具有一定相关性。GBP与BPD组术后血浆IGF-1上升,且持续升高至第16周,而饮食控制组和对照组的IGF-1无明显变化。Sarr等[4]报道,术后IGF-1的明显升高仅见于T2DM患者,非2型糖尿患者无变化。提示IGF-1的变化可能是胃旁路术后T2DM大鼠血糖变化的主要机制。
GBP术比BPD手术操作步骤少,操作相对简单,故手术时间短,死亡率低,生存率高。所以GBP术较BPD术具有安全、操作简单优点。由于观察时间短,长期疗效对比有待进一步观察。
[1] Rubino F.Bariatric surgery:effects on glucose homeostasis.Curt Opin Clin Nutr Metab Care,2006,9:497-507.
[2] Ballantyne GH,Gumbs A,Modlin IM.Changes in insulin resistance following bariatric surgery and the adipoinsular axis:role ofthe adipocytokines,leptin,adiponectin and resistin.Obes Surg,2005,15:692-699.
[3] Hanusch-Enserer U,Cauza E,Brabant G,et al.Plasma ghrelin in obesity before and after weight loss after laparoseopical adjustable gastric banding. J Clin Endoerinol Metab,2004,89:3352-3358.
[4] Sarr MG.Open Roux-en-Y gastric bypass:indications and technique.J Gastrointest Surg,2004,8:390-392.
[5] Rubino F,Gagner M. Potential of surgery for curing type 2 diabetes mellitus. Ann Surg,2002,236:554-559.
2011-08-02)
(本文编辑:屠振兴)
Gastricbypassandbiliopancrticdiversioninthetreatmenttype2diabetes
DIJian-zhong,HANXiao-dong,ZHANGHong-wei,DuYi-bao,WANGYu,ZHENGQi,ZHANGPin.
DepartmentofGeneralSurgery,ShanghaiSixthPeople′sHospital,ShanghaiJiaotongUniversity,Shanghai200233,China
ZHANGPin,Email:zpdjzhxd@yahoo.com.cn
ObjectiveTo compare the treatment effects of gastric bypass (GBP) and biliopancrtic diversion (BPD) in non-insulin dependent diabetes mellitus rats, and investigate the mechanism.MethodsForty GK rats with diabetes mellitus were randomly allocated into four groups: GBP group; BPD group; food restriction group (FR group) and control group with 10 rats in each group. Rats in GBP group and BPD group
GBP and BPD procedures respectively. Rats in FR group were fed with basic feed of 15 g and free access to water. There was no food restriction in rats in control group. The operation time, mortality was recorded. The fasting body weight was measured every week. The plasma glucose, insulin-like growth factor-1 (IGF-1), and leptin concentrations, were measured before treatment and 1, 2, 3, 4, 8, 16 week after treatment.ResultsThe mean operation time was (25±4) min in GBP group and (35±6) min in BPD group; one rat died in GBP group and 3 rats died in BPD group, and the difference between the two groups was statistically significant (P<0.01). The levels of plasma glucose, IGF-1 and leptin were not statistically significant among these groups before treatment. There was no significant difference in plasma glucose and leptin concentrations in the control group. The levels of plasma glucose and leptin in rats in FR group began to decrease 2 weeks later, at the 4th week, the levels of plasma glucose and leptin was significantly lower than that before treatment, and it lasted for the 16 th week, but the level of IGF-1 were significantly different. The levels of plasma glucose and leptin in rats in GBP group and BPD group began to decrease and IGF-1 began to increase 2 weeks after operation, and it lasted for the 16th week, [plasma glucose:(6.8±1.0), (6.3±0.8)mmol/Lvs. (13.9±2.6), (14.1±2.6)mmol/L; leptin: (16.1±3.3), (17.2±3.2)pg/mlvs. (29.4±3.9)pg/ml, (29.4±3.9); IGF-1: (166.1±8.3), (142.2±8.2)ng/Lvs. (119.4±8.8), (109.8±7.9)ng/L,P<0.01], but the levels of plasma glucose and leptin was not statistically different between the two groups. The level of IGF-1 in GBP group was significantly higher than that in BPD group (P<0.05).ConclusionsBoth GBP and BPD can effectively control plasma glucose concentration for rats with diabetes. The possible mechanism is related to decreased leptin and increased IGF-1. Group GBP had a better outcome in operation time, mortality and increasing IGF-1 than those in group BPD.
Diabetes mellitus,type 2; Gastvic bypass; Biliopancrtic diversion
10.3760/cma.j.issn.1674-1935.2011.05.017
200233 上海,上海交通大学附属上海第六人民医院普外科
张频,Email:zpdjzhxd@yahoo.com.cn
猜你喜欢
中老年保健(2021年2期)2021-08-22 07:30:48
昆明医科大学学报(2021年3期)2021-07-22 07:39:52
今日农业(2020年17期)2020-12-15 12:34:28
青少年科技博览(中学版)(2019年7期)2019-10-11 04:13:55
文教资料(2019年31期)2019-01-14 02:32:05
特别健康(2018年4期)2018-07-03 00:38:14
现代检验医学杂志(2016年4期)2016-11-15 02:01:02
文理导航·科普童话(2016年5期)2016-07-14 23:24:48
校园英语·中旬(2016年8期)2016-07-09 21:25:53
中国民族医药杂志(2016年6期)2016-05-09 08:52:55