A review and meta-analysis: molecular prevalence and subtypes distribution of Blastocystis sp. isolated from the symptomatic and asymptomatic populations of China
2024-04-12 02:29DENGTingLIXiaoboLIJuan
赣南医学院学报 2024年2期
DENG Ting,LI Xiao-bo,LI Juan
(1.School of Basic Medicine of Gannan Medical University; 2.Information Technology and Network Management Center of Gannan Medical University; 3.School of Public Health and Health Management of Gannan Medical University,Ganzhou, Jiangxi 341000)
Abstract : Objective : To estimate the prevalence and subtypes distribution of Blastocystis isolated from the symptomatic and asymptomatic populations of China. Methods : A systematic search in English and Chinese databases was performed using Mesh subject and free terms, including "Blastocystis" "Blastocystis hominis" "Blastocystis infection""epidemiology" "prevalence" "occurrence" "subtype(s)" "subtyping" "genotype(s)", and "China". The heterogeneity index was measured by estimating Cochran's Q test and the I2 index of Stata 14. Results : In total, 16 selected studies were considered for the research. The overall molecular prevalence of Blastocystis was 10% (95%CI: 0.07-0.12). The prevalence of Blastocystis was higher in the asymptomatic population 14% (95%CI: 0.08-0.19) than that in the symptomatic population 7% (95%CI: 0.05-0.09). ST3 was identified as the most common strain of Blastocystis,showing a molecular prevalence of 7% (95%CI: 0.04-0.09) in the asymptomatic population and 3% (95%CI: 0.02-0.04)in the symptomatic population. ST3 was followed by ST1 with a molecular prevalence of 2% (95%CI: 0.01-0.04) in the asymptomatic population and 2% (95%CI: 0.01-0.03) in the symptomatic population. Conclusion : The pathogenicity of Blastocystis is not subtype-specific, and the asymptomatic population has a higher prevalence of Blastocystis infection.
Key words : Blastocystis sp.; Prevalence; Subtypes; Asymptomatic population; Symptomatic population; China
Blastocystisis a single-celled anaerobic protozoan that resides in the gut of humans, mammals, birds,reptiles, amphibians, and insects[1]. The life cycle ofBlastocystisis not well understood. It has diverse morphology, including vacuolar, granular, amoeba, and cysts forms. Thick-walled cysts ofBlastocystisthat are present in feces are the major source of infection through in vitro transmission. Amoeba is the pathogenic stage[2]. In addition to fecal transmission, food, water, human-to-human, human-to-animal, and animalto-human transmissions have also been reported[3].Contaminated food and water, poor personal hygiene,poor sanitation, host immunological conditions, and animal contact are the causable factors forBlastocystisinfection[4-5]. This infection is distributed worldwide but is mainly recorded in tropical areas and developing countries. The prevalence ofBlastocystis hominisvaries greatly among different countries, ranging from 0.5% to 70.00%[2,6], however the prevalence is similar in males and females[6].
There is an ongoing debate about the commensal or pathogenic nature ofBlastocystissp.[7].Blastocystissp. present in the feces of asymptomatic people are symbiotic in nature[8-9]. But some studies suggested thatBlastocystisinfection can cause various clinical manifestation including diarrhea, abdominal pain,convulsion, nausea, and non-specific gastrointestinal symptoms (urticaria) in certain population[10-11]. Clinical manifestations ofBlastocystis hominisinfection vary in severity.
In 2007, Stensvold CR proposed a standardized nomenclature forBlastocystisbased on its different subtypes (STs). According to the classification system,26 subtypes (ST) have been reported, out of which 17 classic subtypes were confirmed before 2013, and 9 new subtypes were named after 2013[2]. At present, a total of 10Blastocystisprotozoa subtypes (ST1-ST9 and ST12) have been identified in humans, where subtypes ST1 to ST4 are commonly found subtypes in humans and ST5 to ST9 are rarely found subtypes in humans[1,12]. Some zoonotic subtypes have also been identified in animals, such as ST5 in pigs, and ST6 and ST7 in birds. These animals are the potential hosts for the transmission of zoonotic subtypes ofBlastocystis. ST3 is the most common subtype causing gastrointestinal symptoms[13]. Variation ofBlastocystisinfection with age, sex, and immune status in China is still not clear. Also, no information is available on the pathogenicity of different strains, where some subtypes ofBlastocystismay be parasitic on specific hosts.Many studies have been reported onBlastocystisoccurrence in both symptomatic and asymptomatic populations of China, where the prevalence rate ofBlastocystisranges from 1.41% to 32.64%[13]. Overall, subtypes ST1 to ST7 and ST12 from humans have been identified in the populations of China[14]. The highest prevalence ofBlastocystisinfection has been reported in immunocompromised patients, where individuals living in Guangxi and Yunnan regions were infected majorly with this infection[14]. ST1 to ST3 are dominant humanBlastocystissubtypes found in China, with mixed subtypes such as ST1/ST3, ST1/ST2, and ST2/ST3, which have also been identified[14]. This systematic review and meta-analysis aim to elucidate the weighted molecular prevalence and subtype distribution ofBlastocystissp. isolated from the symptomatic and asymptomatic populations of China.
1 Methods
The study was designed and conducted in 2021 according to the preferred reporting items for systematic reviews and meta-analysis (PRISMA) checklist.
1.1 Data sources and search strategyComprehensive and systematic search was performed in Medline/PubMed, Ovid, Scopus, Embase, web of science, Wangfang, CNKI, VIP, and Sinomed databases. Different combinations of search terms were used such as ("Blastocystis" or "Blastocystis hominis" or"Blastocystis infection") and ("epidemiology" or "prevalence" or "occurrence") and("subtype(s)" or "subtyping" or "genotype(s)") and China. Retrieved papers were added to EndNote X9 software, and duplicate papers were removed automatically as well as manually. Articles were screened by their title, abstract,and full text, respectively. The bibliography of each paper was also searched manually for obtaining relevant literature.
1.2 Inclusion criteria, study screening, and data collectionThe total molecular prevalence of Blastocystis infection in China was estimated on the basis of observational studies, including cross-sections and case controls published before December 31, 2021.These studies have reported the prevalence of human Blastocystis infection using molecular methods. Culture and microscopy-based studies and animal investigations were completely excluded. For studies in the subgroups (symptomatic and asymptomatic) examined in China, only studies with accurate sample size and subtypes reported for each subgroup with equal numbers of positive cases and sequenced isolates were included in this systematic review. Two of the authors conducted screening of the study and three authors performed the data extraction, quality assessment, and data analysis. Further, potential contradictions were resolved by the corresponding author. The pre-designed checklist was utilized to extract the information regarding author name, year of publication, sample size, city/county of the conducted study, diagnostic methods, molecular prevalence, evaluated individuals/patients, and detected subtypes.
1.3 Data-analysisForest plots were used to estimate the pool effect size and 95% confidence interval(CI) effect for each study, illustrating the visual summary of data. The heterogeneity index among studies was assessed by Cochran's Q test and I2index. In the case of heterogeneity, the random-effects model was utilized with the DL method, whereas in the absence of heterogeneity, the fixed-effects model was applied.All analyses were performed using Stata 14 software,and publication bias was evaluated using Egger's test.
2 Results
2.1 Systematic search outputAn initial search of databases resulted in the retrieval of 386 records. After the removal of duplicates, 281 records were subjected to screening on the basis of title and abstract.One hundred ninety-seven records were filtered after the title and abstract screening. Based on full-text accessibility, only 16 records were finally subjected to meta-analysis (Table 1). Major reasons for literature exclusion were reviews or meta-analyses, unrelated topics, animal studies, microscopy and culture-based studies, unrelated populations, not reported total/subtotal sample size or subtyping, and duplicated studies.The flowchart of the included studies for this systematic review is shown in Fig.1.
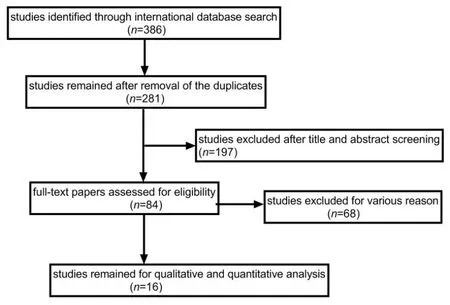
Fig.1 Flowchart of the included ellgible studies in systematic review
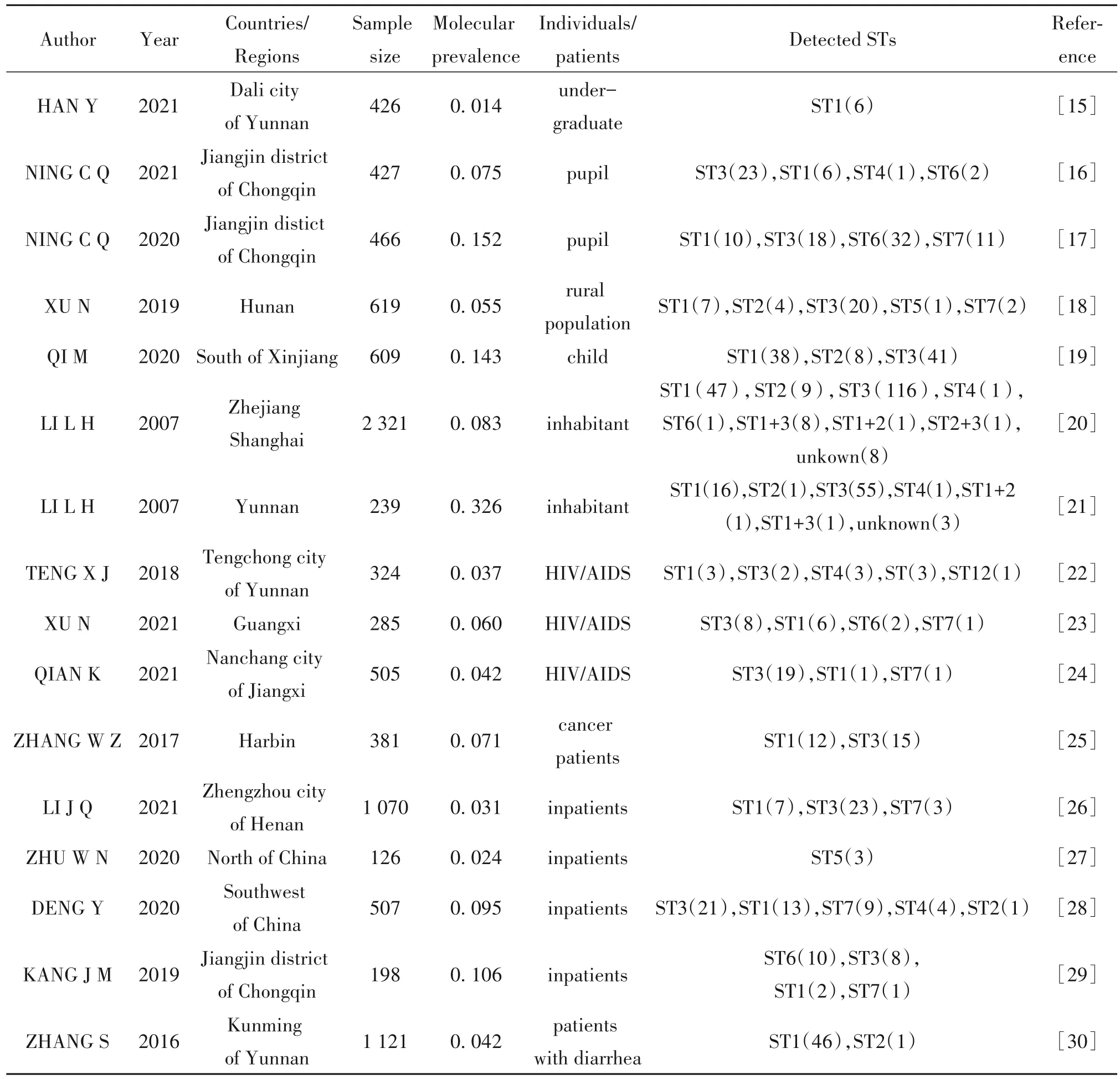
Table 1 Characteristics of 16 studies subjected to meta-analysis
2.2 Quality assessmentThe studies included in the review were cross-sectional reports; hence the risk of bias was estimated by the agency for healthcare research and quality (AHRQ) scale. The evaluation criteria included 11 items, with a score of 1 for "yes", 0 for "no" or "unclear", 0-3 for low-quality literature,4-7 for medium quality literature, and 8-11 for highquality literature[31]. Studies with a score of ≤ 3 were excluded for further consideration. Sixteen studies were selected on the basis of quality assessment. The evaluation results were 7 high-quality literature, 9 medium-quality literature.
2.3 Heterogeneity testSixteen articles selected for the study were analyzed, and the total population was divided into two subgroups: the asymptomatic group and the symptomatic group. In the heterogeneity test, the I2value was 97.3% in the asymptomatic group and 78.8% in the symptomatic group. Also, in the inter-subgroup heterogeneity test, P<0.01, indicating a significant difference that suggested a higher fluctuation of Blastocystis infection prevalence in the asymptomatic group than that in the symptomatic group. In the Q test, the I2value was found to be 94.7%, which is more than 70%, and P<0.10, indicating significant heterogeneity among the selected literature. Hence, a sensitivity analysis was performedto investigate the cause of this high degree of heterogeneity.
2.4 Sensitivity analysisSensitivity analysis, conducted on 16 records of the study, concluded no interference with the results of a meta-analysis. Sensitivity analysis indicated that this study has good stability(Fig.2).

Fig.2 Chart of sensitivity analysis of 16 Blastocystis studies
2.5 A meta-analysis of random effectsA metaanalysis based on random effects showed that the effect size of 16 studies was 10% with a 95%CIof 0.07-0.12,which was found to be statistically significant (Z=7.68,P<0.05). Asymphtom group represented asymptomatic normal residents with an effect size of 14%.95%CIwas 0.08-0.19,Z=5.88, andP<0.05. Symphtom group represented patients with AIDS, cancer,or diarrhea, with an effect size of 7%. 95%CIwas 0.05-0.09,Z=6.88,P<0.05). The results indicated thatBlastocystisinfection existed in asymptomatic populations as well as symptomatic populations. Infection prevalence was found to be higher in the asymptomatic populations than that in the symptomatic populations (Fig. 3). ST3 was observed as the dominant strain, with infection prevalence of 7% and 3% in the asymptomatic population and symptomatic population,respectively. Also, 95%CIfor the asymptomatic population was 0.04-0.09, and for the symptomatic population was found to be 0.02-0.04 (Fig. 4). ST3 was followed by ST1 with infection prevalence of 2% in the asymptomatic population and symptomatic population,respectively. 95%CIfor the asymptomatic population was 0.02-0.04, and for the symptomatic population was found to be 0.01-0.03(Fig. 5). Other epidemic strains included ST2, ST4, ST5, ST6, ST7, and ST12, and the mixed infection of ST1 and ST3, ST1 and ST2, and ST2 and ST3 were also observed. For these strains, the infection rate of the asymptomatic population and the symptomatic population was found to be 5% and 2%, respectively, and 95%CIwere 0.03-0.07 and 0.01-0.03, respectively (Fig.6).

Fig.3 Forest plot of pooled molecular prevalence of Blastocystis sp. in the human population of China

Fig.4 Forest plot of pooled molecular prevalence of Blastocystis ST3 in the human population of China

Fig.5 Forest plot of pooled molecular prevalence of Blastocystis ST1 in the human population of China

Fig.6 Forest plot of pooled molecular prevalence of other Blastocystis sp. in the human population of China
2.6 Bias testA funnel plot was used to investigate the publication bias in the study. A symmetrical funnel plot was observed. Further, Egger's symmetry test was performed in Fig. 7. The estimatedP-value was found to be 0.441, which was greater than 0.05, indicating a symmetrical funnel plot. These results showed that there was no publication bias in the literature taken for the study.

Fig.7 Funnel plot of pooled studies of Blastocystis sp. in the human population of China
3 Discussion
Blastocystisis the most common protozoan present in the human gastrointestinal tract[1]. To our knowledge, this is the first review and meta-analysis of the molecular prevalence ofBlastocystissubtypes in the symptomatic and asymptomatic population of China.In our study, the overall prevalence ofBlastocystisinfection in the Chinese population was found to be 8%.The prevalence ofBlastocystis hominisvaries among different countries, such as 3.2% in Britain, 0.7%in Venice, 12.25% in California, 8% in Canada,0.5%-1% in Japan, 17.37% in Nepal, 17.5% in Saudi Arabia, and 14.1% in Yugoslavia[2]. The overall prevalence ofBlastocystisinfection in China is relatively low as compared to other countries. But early studies showed that the prevalence ofBlastocystisinfection in China ranged from 8.2% to 32.6%[19-20]. It is peculated that the results is related to the improvement of sanitary conditions and test methods of Chinese residents in recent years.Blastocystis hominishas a global distribution, the prevalence of infection varies with age, occupation, local climate, sanitary conditions,nutritional status, immune status, testing season and methods.
Due to the vast variation in pathogenicity ofBlastocystis, the prevalence and subtype distribution analysis ofBlastocystisin populations with and without clinical symptoms is of particular importance. In this study, the molecular prevalence ofBlastocystisinfection in the asymptomatic and symptomatic population of China was observed as 11% and 5%, respectively.This suggests thatBlastocystisinfection was more common in the asymptomatic population than that in the clinically symptomatic population. As concluded from the results,Blastocystismay be one of the intestinal microbiota of humans, which is consistent with the results of Tito's study[8].Blastocystisbehavior in the host-parasite relationship appears to be a beneficial protist in the gut, shaping bacterial populations profiles associated to healthy intestinal microbiota rather than a pathogenic organism[9]. Previous reports support the hypothesis thatBlastocystisisolated from asymptomatic and symptomatic patients may exhibit distinct strains/species with different pathogenicity and different molecular clades[32]. ST3 was found to be the most common subtype causing clinical symptoms, with the molecular prevalence of 7% and 3% in the asymptomatic and symptomatic populations, respectively. It was found to be distributed more in the asymptomatic population than that in the symptomatic population. ST1 was observed as the second most popular subtype in China, with a prevalence of 2% in the symptomatic and asymptomatic populations, respectively. Other endemic strains were ST2, ST4, ST5, ST6, ST7, and ST12,and coinfection with ST1 and ST3, ST1 and ST2, and ST2 and ST3 with a prevalence of 5% and 2% in the asymptomatic population and in the symptomatic population, respectively were also observed.
The results of this study are highly heterogeneous, which may be due to the fact that the data are derived from cross-sectional studies, and that the prevalence ofBlastocystisinfections is affected not only by health status, but also by age, region, sanitary conditions, detection conditions and methods, and other factors.
4 Conclusion
The pathogenicity ofBlastocystiswas not subtype specific, and the prevalence ofBlastocystisinfection was higher in the healthy population.