
Neuroimaging in atypical normal tension glaucoma:debating routine implementation in the absence of classic neurological findings
2024-03-20 06:33UmayGvenGlizarDemirokGnerneySelmaUzman
Umay Gven, Glizar Demirok, Gner ney, Selma Uzman
Ophthalmology Department, Ankara Training and Research Hospital, Ankara 06230, Turkey
Abstract
● KEYWORDS: normal tension glaucoma; neuroimaging;atypical visual field defects
INTRODUCTION
Normal tension glaucoma (NTG) is defined as a condition where the intraocular pressure (IOP) is within normal limits, there is optic disc cupping and visual field (VF) loss similar to that seen in other chronic forms of glaucoma, and these changes cannot be attributed to a clear cause[1].Given that optic disc cupping is not pathognomonic of glaucoma, the diagnosis of NTG is actually a diagnosis of exclusion.
Similar optic disc changes can also be seen in ischemic neuropathy, hereditary anomalies, and compressive neuropathies.Distinguishing glaucomatous and nonglaucomatous optic disc cupping is often difficult during clinical examination.It has been reported that intracranial lesions can mimic glaucomatous optic disc changes and cause confusion in diagnosis.Tumors that affect the optic nerve and optic chiasm, especially those that compress them, can also create VF defects similar to those seen in glaucoma[2].In addition, compression of the optic nerve can make the disc susceptible to glaucomatous changes even at normal pressures, leading to the patient being evaluated only as NTG.Although it may be apparent in abnormal NTG cases with neurological findings, it may be difficult to distinguish compressive optic neuropathy from classical NTG[3-4].
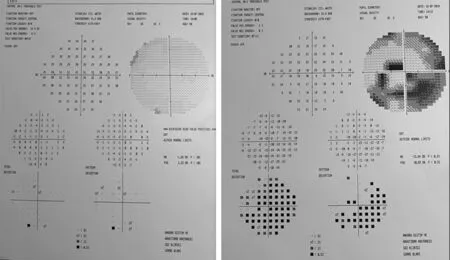
Figure 1 Visual field test of an unilateral normal tension glaucoma, asymmetry in visual field defect.
Presently, the use of routine cranial magnetic resonance imaging (MRI) or computed tomography (CT) scanning to aid in ruling out probable intracranial lesions in NTG is controversial.When encountered with a patient presenting with NTG with neurologic signs, or if doubt exists as to the nature of the visual loss or disc changes, is generally accepted that neuroimaging should be obtained.However, the patient presenting with NTG without classic neurologic signs raises the question as to whether neuroimaging should be performed.There are different reports regarding the prevalence of intracranial mass lesions in NTG.Some advocate for routine scanning in NTG, while another study suggested that routine neuroimaging may have very little clinical value and that compressive optic neuropathy can only be diagnosed with clinical justification, thus arguing that routine neuroimaging is not necessary in NTG[2-5].The first step in determining the value of a screening test (such as neuroimaging in NTG) is to determine the prevalence of the lesion(s) in the relevant patient population.The purpose of this study is to evaluate the frequency of pathologies observed in neuroimaging of NTG patients without typical glaucoma findings and to discuss the necessity of neuroimaging in this patient group.
SUBJECTS AND METHODS
Ethical ApprovalThe study was designed as a retrospective one-centre study in the Department of Glaucoma in Ankara Training and Research Hospital (Turkey) with the approval number E-22-1139.The study protocol underwent thorough review by the Institute’s Review Board, ensuring compliance with all principles outlined in the Declaration of Helsinki(1964) and its subsequent amendments.
Patients were diagnosed with NTG based on specific criteria,which included the presence of glaucomatous neuroretinal rim loss in at least one eye, confirmation of an open angle through gonioscopy, IOP measuring below 21 mm Hg, and the absence of any atypical findings or non-glaucomatous VF defects initially.The progression rate was calculated according to clinical method by counting the difference between mean deviation (MD) indicators from 2 reliable VF from the time of the diagnosis and the time of inclusion to the study.Then, this difference was calculated for one year of observation, and in case the result was higher than 1.5 dB/y.
We retrospectively analysed the results of totally 90 patients who were followed up with a diagnosis of NTG between 2015 and 2022 and neuroimaging was requested because of atypical findings: 1) unilateral NTG with asymmetry in optic disc appearance or VF, 2) fast VF progression (1.5 dB per year or more) assessed according to at least 3 reliable VF results, 3) headache of sufficient severity and frequency to require neuroimaging, 4) scotoma restricted by a vertical line(hemianopia, quadrantanopia, and bitemporal defect), 5) the damage in the VF inconsistent with optic disc appearance,6) Optic disc excavation accompanied by pallor (Figures 1 and 2).Importantly, participants had no suspicious evidence of causes other than NTG at the initial diagnosis but developed suspicious signs later on, leading to the subsequent requests for neuroimaging.
If there were no contraindications, cranial MRI were acquired with contrast administration.However, if there were conditions such as renal insufficiency that posed a limitation to the administration of contrast agents, the images were obtained without contrast.It is important to note that this study was retrospective in nature, and therefore, the images could not be standardized.
Patients who discontinued their glaucoma follow-ups,diagnosed with secondary open or angle closure glaucoma during follow-ups, and who underwent any intraocular surgery were excluded from the study.

Figure 2 Visual field defect which is incompatible with glaucoma: vertical scotoma.
Demographic characteristics of the patients such as age,gender, marital status, comorbidities, family history;date of presentation, IOP measurements (with Goldmann applanation tonometer), detailed anterior and posterior segment examination findings (biomicroscopic examination);accompanying ocular findings, retinal nerve fibre layer thickness(RNFLT) analyses with optical coherence tomography (OCT,Heidelberg Spectralis, Germany), VF examination (Humphrey Field Analyzer 3 from ZEISS) results, central corneal thickness(CCT) values, medical and/or surgical treatments and followup period, radiological images (cranial MRI) and reports were recorded.
Statistical AnalysisThe statistical analyses were performed using SPSS version 21.The normal distribution of variables was examined through visual inspection (histograms and probability plots) and analytical methods (Kolmogorov-Smirnov test).Descriptive analyses were provided using mean and standard deviation for normally distributed variables,median and interquartile range (IQR) for non-normally distributed variables, and frequency tables for nominal variables.Between-group comparisons were conducted using the Student’st-test for normally distributed variables, Mann-WhitneyUtest for non-normally distributed variables, oneway ANOVA for comparisons involving more than two groups with normally distributed variables, and Kruskal-Wallis test for comparisons involving non-normally distributed variables.In cases where significant differences were found among groups,pairwise post-hoc comparisons were performed.The results of post-hoc analyses were reported using either the Tukey or Tamhane test, depending on the homogeneity of variances.The frequencies of categorical variables were presented using contingency tables.The Chi-square test, Fisher’s exact test(when assumptions for the Chi-square test were not met), or Fisher-Freeman-Halton test (for tables larger than 2×2 when assumptions for the Chi-square test were not met) were utilized to determine whether there were significant differences in frequencies between groups.Bonferroni correction was applied for multiple post-hoc comparisons.AP-value less than 0.05 was considered statistically significant.
RESULTS
A retrospective analysis was conducted on 90 patients who were followed up with a diagnosis of NTG and underwent cranial MRI due to atypical findings.Of these patients,38.9% (n=35) were male and 61.1% (n=55) were female.The mean age of 87 of the total 90 patients was 58.74±13.99y with a mean age of 60.21±12.91 (35-85)y for females and 56.54±12.92 (18-80)y for males.There was no statistically significant difference between age groups by gender (P>0.05).The mean CCT was 537.34±45.05 (427.5-628) µm, mean IOP was 16.84±3.8 (8-27) mm Hg.The median cup/disc(C/D) ratio was 0.6 (IQR=0.3), median RNFLT was 88.5(IQR=18.13) in the first visit, median RNFLT final value was 84.25 (IQR=17.63) µm, median VF-MD value was -4.78(IQR=5.51), and median VF pattern standard deviation(VF-PSD) value was 4.27 (IQR=4.46).
Of the patients, 45.6% (n=41) had imaging requested due to optic disc appearance or asymmetry in VF, 11.1% (n=10)had rapid progression, 17.8% (n=16) had severe and frequent headaches requiring neuroimaging, 20% (n=8) had scotoma restricted by a vertical line, 2.2% (n=2) had damage in the VF inconsistent with optic disc appearance, and 3.3% (n=3)had optic disc excavation accompanied by pallor.Among the patients, 33.3% (n=30) had normal radiology results, while pathology was detected in 66.7% (n=60).The results of 30%(n=27) of patients showed gliosis, 2.2% (n=2) had sequelae of cerebrovascular event, 4.4% (n=4) had meningioma, 3.3%(n=3) had pituitary adenoma, 2.2% (n=2) had pineal cyst,3.3% (n=3) had vascular malformations such as aneurysm,venous angioma, 4.4% (n=4) had asymmetrical gliosis,5.6% (n=5) had pseudotumor cerebri (PTC), 8.9% (n=8) had encephalomalacia, 1.1% (n=1) had arachnoid cyst, and 1.1%(n=1) had demyelinating disease (Table 1).
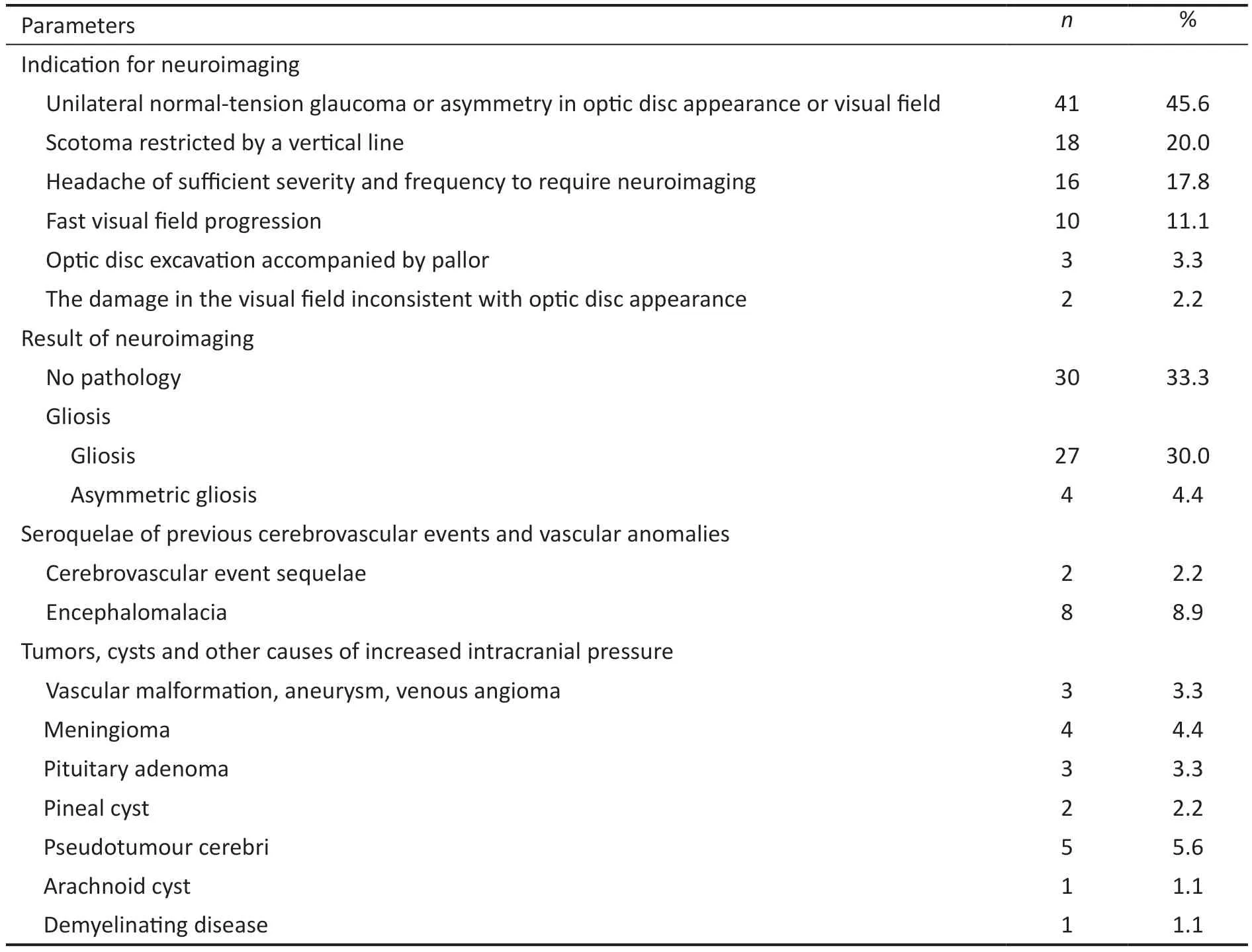
Table 1 Evaluation of patients in terms of neuroimaging indication and results n=90
Among the patients, while a glaucomatous VF defect was detected in 20% (n=18), an asymmetric VF defect was found in 48.9% (n=44), and a VF defect incompatible with glaucoma was detected in 17.8% (n=16).In 13.3% (n=12) of patients,no defect was detected in the VF.When patients with normal and abnormal neuroimaging results were compared in two groups, a significant difference was observed in terms of VF defect patterns.Post-hoc analyses were performed with pairwise comparisons to determine which group the difference originated from (using Bonferroni correction,P=0.0083), and it was found that the difference was due to the relationship between the third and fourth groups.In other words, cranial pathology was more frequently detected in patients with nonglaucomatous VF defects (Table 2).
When patients with normal and abnormal radiology results were compared in terms of mean IOP, median C/D ratio, initial and final RNFLT averages, and median MD and PSD of the VF tests, no significant differences were observed between the two groups.However, there was a statistically significantage difference between the groups, with a median age of 55y(range 35-70y) for the normal group and 65 (range 18-85y)for the abnormal radiology group.The mean age of the abnormal radiology result group was higher than that of the normal radiology result group (P=0.021; Table 3).
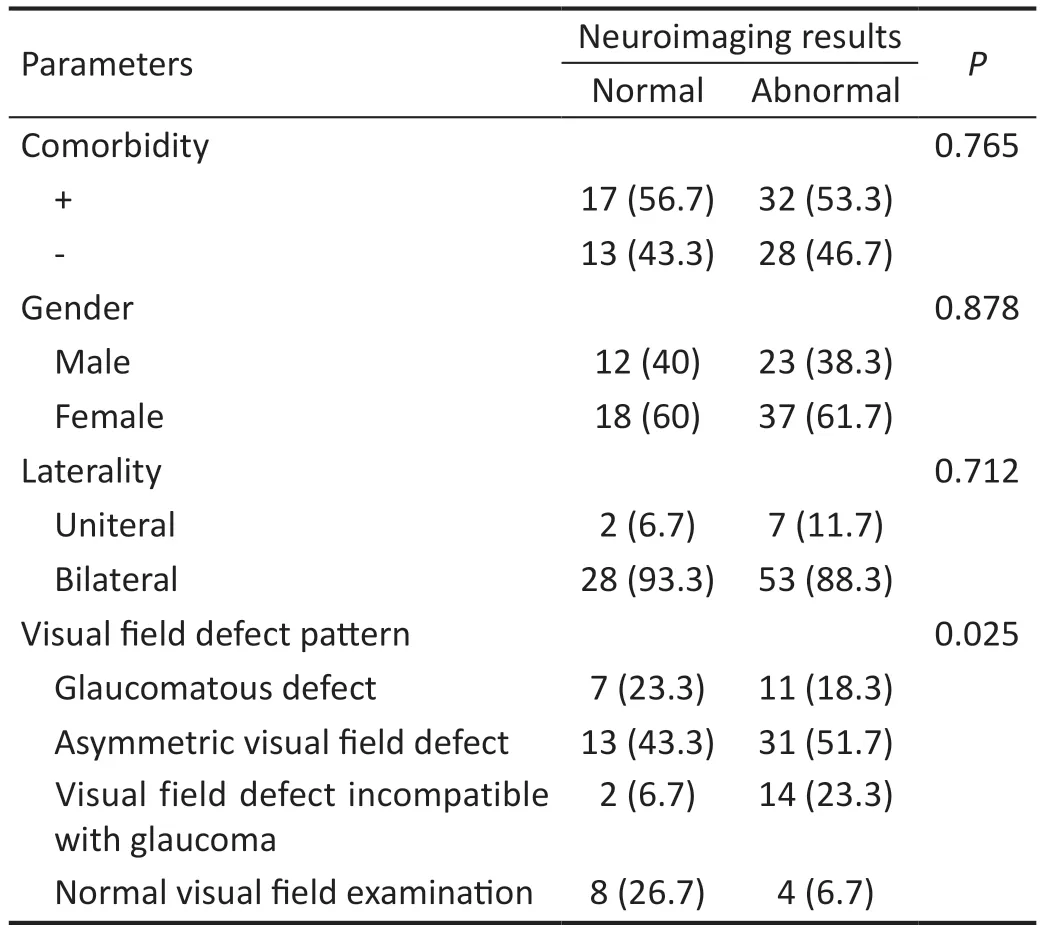
Table 2 Comparison of patients with and without normal radiological results in terms of comorbidity, gender, laterality, and visual field defects n (%)
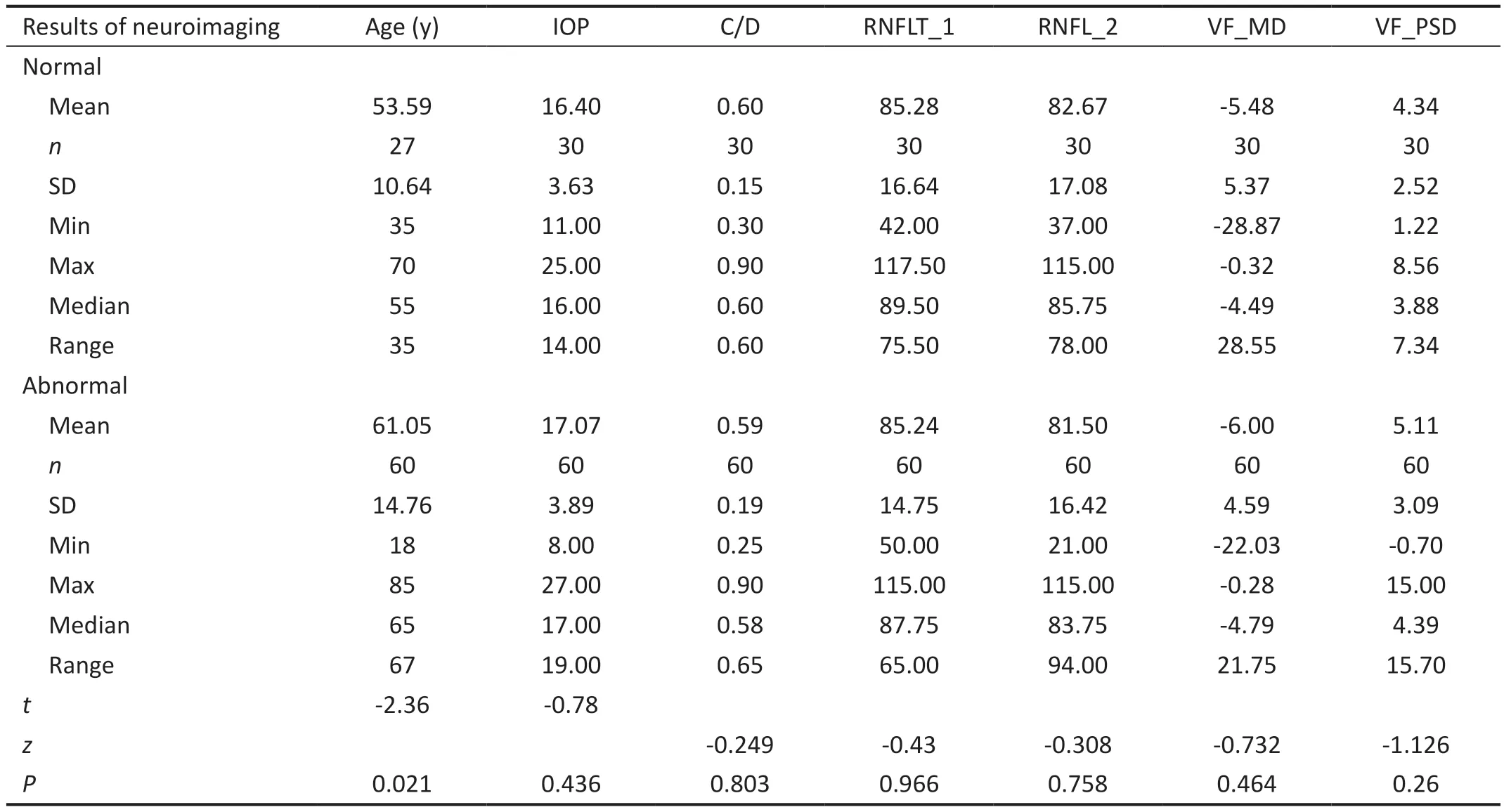
Table 3 Evaluation of patients with and without normal radiological results in terms of age, intraocular pressure, cup to disc ratio, retinal nerve fiber layer thickness values and visual field parameters
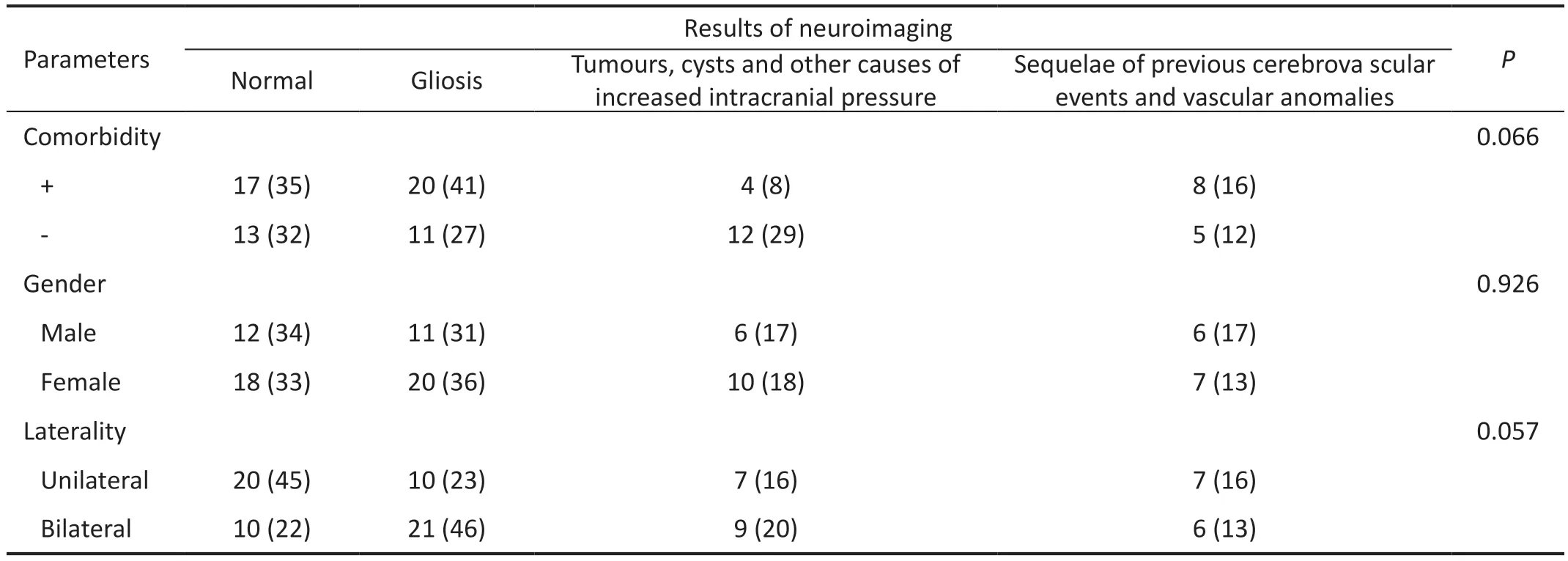
Table 4 Comparison of patients with and without normal radiological results in terms of comorbidity, gender and laterality n (%)
In order to make a comparison, PTC and demyelinating disease group, which had a low frequency, were included in the tumour and cyst group and compared again.No significant relationship was found between the radiology groups in terms of gender, presence of comorbidity, and laterality (Table 4).According to the radiology results, there was no statistically significant relationship in terms of IOP, visual acuity (VA),C/D ratio, RNFLT, CCT, and VF MD and PSD values at a significance level of 5%.However, a significant difference was observed in the age average between the groups.Posthoc analyses revealed that the difference stemmed from the comparison between the 2ndand 3rdgroups (P=0.003).Thus, it was observed that gliosis findings were more commonly seen in older ages, while tumors, cysts, and pseudotumors were significantly more common at a younger age (Table 5).
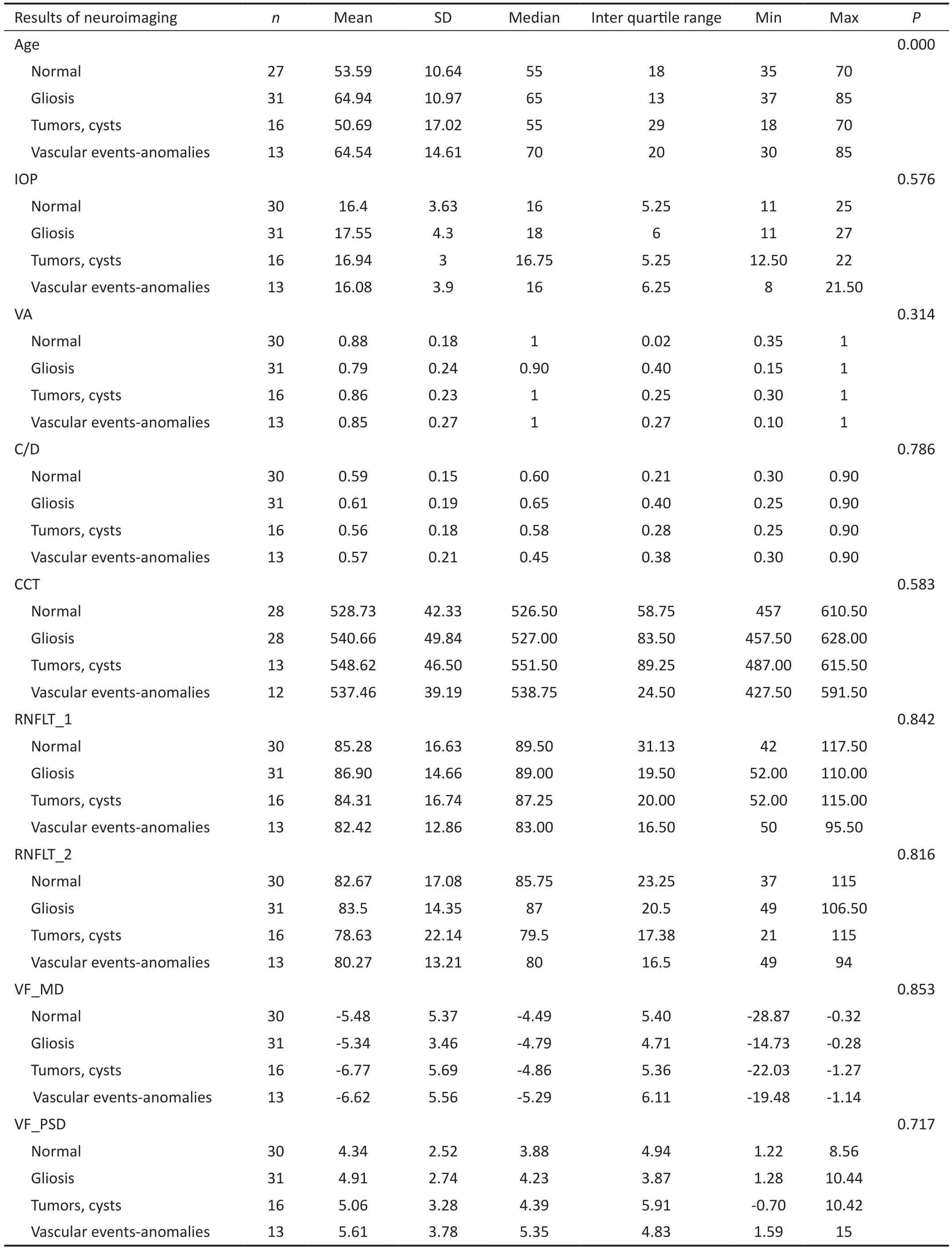
Table 5 Comparison of patients with and without normal radiological results in terms of age, IOP, VA, RNFLT, CCT, VF test parameters
DISCUSSION
In the management of NTG, there is a general consensus regarding the importance of neuroimaging when patients present with neurological findings or when there is uncertainty surrounding the nature of vision loss or optic disc changes.However, the question of whether neuroimaging should be routinely conducted in patients without classic neurological manifestations remains unresolved.This study highlights that cranial MRI may detect intracranial pathology more frequently in patients with NTG and atypical VF defects which are incompatible with glaucoma.Furthermore, the study emphasizes the importance of cranial imaging in NTG cases, especially in older patients, to prevent misdiagnosis and unnecessary lifelong medication use in the absence of underlying vital conditions.
Our study found that the most common reasons for recommending neuroimaging in patients was due to asymmetry in optic disc appearance or VF, or unilateral NTG cases,which accounted for 45.6% of cases.This is consistent with a recent study, where asymmetry was also identified as the primary indication for suspicion of atypical NTG[6].However,a different study reported that only 25% of NTG patients had unilateral VF defects at the time of diagnosis, which suggests that asymmetry is not an unusual finding in NTG.NTG patients can have asymmetric VF defects, IOP values, or ocular blood flow changes[7-8].
According to our results, patients with intracranial pathologies detected by neuroimaging are significantly those who have incompatible VF defects with glaucoma.Another study confirmed that vertical VF defects were associated with brain pathology in 71.4% of cases, worsening of VF-MD in 50%of cases, and optic disc pallor in 18.1% of cases.The study emphasized that patients with NTG and these symptoms clearly need neuroimaging[4-6].
Several studies have reported that the average age of patients with NTG is around 60, which is consistent with the findings of our study[9].We found that the average age of patients with normal neuroimaging results was significantly lower than that of patients with abnormal results, suggesting that neuroimaging may be particularly important in older age groups.In fact, a study found that no significant neurological pathology was detected in NTG patients under the age of 50[6].This suggests that the prevalence of NTG in younger patients, including those with unilateral involvement, may be a typical course of NTG.Furthermore, our study found that gliosis was more commonly observed in older patients, while tumors, cysts, and pseudotumors were more prevalent in younger patients.
The presence of ischemic foci in different regions of the brain was the most common and significant abnormality detected in our NTG patient group.This result was also reported in a study by Kosior-Jareckaet al[6].Since we did not have a control group matched for age, we cannot determine the frequency of ischemic foci in this particular age group.However, studies have shown that ischemic changes in the brain are more frequent in NTG patients than in control groups and can occur in up to 40% of cases, indicating a link between central nervous system vascular insufficiency and NTG pathogenesis[10].Some authors have suggested that brain ischemic lesions may be associated with VF damage and progression in NTG patients to some extent[11-12].Therefore, these gliotic changes can be interpreted not as a different diagnosis, but as cranial changes accompanying the diagnosis of NTG.Despite our findings related to age, it might be more prudent to make a decision regarding cranial imaging based on VF, optic disc appearance,and progression rate.
We identified 16 patients with compressive lesions such as tumors, cysts, and other causes of increased intracranial pressure.Some clinicians believe that optic atrophy resulting from compression of the anterior visual pathways associated with glaucoma-related optic disc cupping can be distinguished clinically.However, in a study where assessments were performed using color fundus photographs and VF examinations, it was demonstrated that even though the evaluations were carried out solely by glaucoma specialists,accurate diagnosis was achieved in 88.1% of glaucoma cases and 75% of optic neuropathy cases[2].
Compressive lesions affecting the anterior visual pathway can lead to optic disc cupping.Portney and Roth[13]described an intracranial aneurysm in a 51-year-old woman with suspected early-stage glaucomatous optic disc findings.Generally, optic atrophy caused by these lesions does not resemble glaucoma as the accompanying cupping is usually absent, and the optic disc appears excessively pale.However, in some cases of compressive optic neuropathy, the optic nerve may lack pallor and appear to be cupped to such a degree that it raises suspicion of non-glaucomatous cupping[1,9,14-15].In a study conducted by Trobeet al[16], a misdiagnosis of glaucomatous optic disc cupping was accidentally made in 8 out of 30 eyes (27%) with compressive optic neuropathy.In another study they conducted, 13 out of 29 eyes (44%) with nonglaucomatous optic atrophy were incorrectly diagnosed as“glaucoma”[17].
Five patients in our study were found to have PTC upon undergoing neuroimaging.It is established that PTC can lead to optic nerve and VF changes that resemble those of glaucoma,even in cases where cerebrospinal fluid pressure is normal[18].The optic chiasm is supplied by the posterior communicating arteries, which loop around the infundibulum above the pituitary gland.Any mechanical changes in the vicinity of the pituitary or sella turcica can lead to ischemic changes in the optic nerve by simultaneously pulling the optic chiasm and its perfusion vessels downwards.This relationship should be borne in mind in cases involving the triad of empty sella,NTG, and visual loss.Some authors suggest that neuroimaging should be performed in all NTG patients to prevent delayed diagnosis and visual impairment[19].Another study has suggested that the association between primary empty sella and glaucomatous optic neuropathy is likely coincidental[20].
A study identified pathological changes in the anterior visual pathways in 18 patients (14.2%) through neuroimaging, with intracranial meningioma being the most common cause.Kalenaket al[21]reported a case of a patient developing optic disc excavation and VF loss due to intracranial meningioma.In our study, among the suspected NTG patients referred for neuroimaging, 4 patients were found to have meningioma,3 with pituitary adenoma, 2 with pineal cyst, and 1 with arachnoid cyst.Another study reported that 4 NTG patients with a positive family history of glaucoma were found to have advanced intracranial meningioma after years of being treated with antiglaucomatous medications.Rapid progression that was incompatible with glaucoma was noted, leading to neuroimaging and the detection of mass lesions[6].These findings suggest that neuroimaging should be considered in NTG patients with unusual clinical features to prevent delayed diagnosis and vision loss.
In a study, it was found that 40% of patients undergoing neuroimaging due to NTG had rapid progression as the cause, indicating an underlying compressive neuropathy.The mentioned study defined progression rate in terms of VF-MD with a threshold of 1.5 dB or higher per year.Therefore, a detailed analysis of pattern defects and progression rate appears to be crucial in determining who should undergo MRI scanning to identify those at risk[22-23].According to our findings, the absence of significant pathology in neuroimaging results conducted with indications of rapid progression may be associated with the coincidental benign nature of the patients’conditions.Intracranial lesions with a malignant nature can exhibit faster progression, thus warranting the indication for neuroimaging during follow-up.
Some authors argue that neuroimaging screening should be the primary approach in managing NTG patients due to the prevalence of intracranial lesions.Assessing the costeffectiveness of this strategy requires considering health outcomes, benefit values, adjusted life years gained, and costs.Ahmedet al[4]conducted a study analyzing the economic and quality of life consequences of delayed or missed diagnosis of intracranial lesions affecting the anterior visual pathway.The findings supported routine neuroimaging as a cost-effective approach for NTG patients.Thus, neuroimaging screening for suspected NTG patients could enhance early detection and timely management of intracranial lesions, leading to improved outcomes and quality of life.
According to the American Academy of Ophthalmology,neuroimaging is not mandatory for the evaluation of all NTG patients, but consultation with a neuro-ophthalmologist and neuroimaging may be necessary if there is more pallor than cupping in the optic nerve, if the patients are younger than 65 years of age, if there is a rapid progression of optic nerve damage, if there is significant asymmetry between the optic nerves, or if the VF defects suggest damage in a more posterior visual pathway[24].
In our study, it is crucial to emphasize that neuroimaging was specifically requested for cases identified as having atypical findings, rather than for all NTG cases.We made a deliberate and thoughtful decision to perform neuroimaging scans on patients who met at least one additional inclusion criterion.These inclusion criteria were meticulously established through a comprehensive review of the existing literature.By adopting this approach, we aimed to target and investigate the specific subset of NTG cases that exhibit unique characteristics warranting further examination.
Our study reveals a high incidence of intracranial pathology,particularly in NTG patients with atypical VF defects that are not consistent with glaucoma.In light of these results, we strongly recommend requesting neuroimaging, particularly for NTG patients who exhibit VF abnormalities that are not typical of glaucoma.It is important to note that ischemic gliotic changes and vascular sequelae are more prevalent in older individuals, while compressive lesions may be more common in younger people, often mimicking the symptoms of NTG.Although ischemic gliotic foci were observed at a high rate,we could not conclude whether this condition is associated with NTG or should be evaluated as a different intracranial pathology.The influence of NTG on cognitive functions and its effects on the brain have not been conclusively demonstrated[25].For this, further studies with age-matched comparisons are needed.
Our study has some limitations.First, it is retrospective in nature.Another limitation is that it is a single-center study,so neuroimaging was only performed on atypical NTG cases deemed appropriate by our clinic.However, our sample size may be too small to reach a conclusion, and it needs to be confirmed in further studies.Finally, due to the absence of a control group, we cannot comment on the frequency of pathologies or findings in individuals with NTG compared to healthy individuals, limiting the scope of our study.
In daily clinical practice, ophthalmologists face the challenge of identifying patients who require neuroimaging to rule out potentially life-threatening conditions that can mimic glaucomatous optic neuropathy.With this study, we hope to raise awareness of the importance of comprehensive evaluation and appropriate management of patients with NTG and atypical VF defects.Further studies are needed to better understand the relationship between ischemic gliotic changes and NTG.
ACKNOWLEDGEMENTS
Conflicts of Interest:Güvenç U,None;Demirok G,None;Üney G,None;Uzman S,None.
 International Journal of Ophthalmology2024年3期
International Journal of Ophthalmology2024年3期
- International Journal of Ophthalmology的其它文章
- Meibomian glands segmentation in infrared images with limited annotation
- Artificial intelligence for the detection of glaucoma with SD-OCT images: a systematic review and Meta-analysis
- Overexpression of TRPV1 activates autophagy in human lens epithelial cells under hyperosmotic stress through Ca2+-dependent AMPK/mTOR pathway
- Dry environment on the expression of lacrimal gland S100A9, Anxa1, and Clu in rats via proteomics
- Semaphorin 7A impairs barrier function in cultured human corneal epithelial cells in a manner dependent on nuclear factor-kappa B
- Novel MIP gene mutation causes autosomal-dominant congenital cataract