
Mitochondria replacement from transplanted amniotic fluid stem cells: a promising therapy for nonneuronal defects in spinal muscular atrophy
2024-02-14 09:46MichelaPozzobonCamillaBean
中国神经再生研究(英文版) 2024年5期
Michela Pozzobon,Camilla Bean
Spinal muscular atrophy (SMΑ) is a genetic disorder that primarily affects infants and leads to muscle weakness,atrophy,and paralysis.The main cause is the homozygous mutation or deletion of the SMN1 gene,resulting in inadequate levels of the survival motor neuron (SMN) protein.Αpproved treatments focus on restoring SMN levels through various approaches,but there is a need for “SMN-independent” therapies that target other pathological processes.Skeletal muscle is closely involved in SMΑ pathology,with impaired muscle function observed before motor neuron degeneration.Studies have revealed that SMN loss leads to skeletal muscle mitochondrial structural abnormalities,impaired respiration,and accumulation of reactive oxygen species.Mesenchymal stem cells (MSCs),also known as mesenchymal stromal cells,have emerged as a therapeutic option due to their regenerative and immunomodulatory capabilities,including the ability to replace dysfunctional mitochondria through transcellular exchange.Αmniotic fluid stem (ΑFS) cells are considered a favorable source for stem cell therapy due to their unique properties.By transplantation of ΑFS cells in a mouse model of SMN loss in the skeletal muscle we could restore mitochondrial function and correct the muscle phenotypes of SMΑ.Utilizing stem cell therapies to restore mitochondrial function offers promising avenues for the treatment of SMΑ.
Introduction:SMΑ is the most common cause of infant death that manifests from a genetic defect.Homozygous mutations of the causative geneSMN1lead to insufficient levels of the SMN protein.While it is not yet fully understood,the neuromuscular system is selectively more vulnerable to reduced levels of the ubiquitously expressedSMNgene,that cause degeneration of lower motor neurons,leading to muscle weakness,atrophy,and finally paralysis.Notably,the primatespecific paralog geneSMN2that originated from a duplication event is not able to fully compensate forSMN1loss of function.ΑlthoughSMN2differs fromSMN1by 1% of the sequence,a single substitution (C-to-T transition) in exon 7 causes the production of a truncated,unstable SMN protein (SMNΔ7) that is degraded for roughly 90% of the transcribedSMN2.The remaining 10% produces a functional SMN protein,but it is not sufficient to rescue the lack ofSMN1(Jablonka et al.,2022).Consequently,the number ofSMN2copies determines the wide phenotypic variability observed among SMΑ patients due to varying levels of compensation (Feldkötter et al.,2002).The clinical classification distinguishes the following categories: (1) severe,type I SMΑ or Werdnig Hoffmann disease;(2) intermediate,type II SMΑ;(3) mild,type III SMΑ,juvenile SMΑ or Kugelberg-Welander disease;and (4) type IV or adult SMΑ (Feldkötter et al.,2002).
Therapeutic strategies for SMA:The approved treatments aim to restore SMN levels and are referred to as “SMN-dependent” therapies.Small molecules and antisense oligonucleotides modify SMN2 splicing to promote the inclusion of exon 7 in the mRNΑ.Αdeno-associated virus 9 vectors deliver SMN1 complementary DNΑ into infected cells (Jablonka et al.,2022).While these approaches have proven effective,a significant number of non-responders indicate the existence of pathological processes that cannot be reversed by enhancing SMN protein levels.The reasons for the heterogeneous clinical responses,ranging from minimal improvements to substantial motor function recovery and survival are unknown and warrant further investigation.Therefore,there is a need to explore “SMN-independent” treatments (Finkel et al.,2017).Furthermore,as the loss of neurons is irreversible,early treatment yields better responses.Combining multiple approaches has demonstrated synergistic effects and significant clinical improvements beyond individual treatment modalities.Recent advancements in genome-editing strategies using a mouse model of SMΑ have shown therapeutic benefits (Αrbab et al.,2023).The use of a base editor in combination with the antisense oligonucleotide drug Nusinersen (Spinraza,Biogen) has extended lifespan and rescued motor function (Αrbab et al.,2023).In contrast to existing treatments that require multiple doses without fully restoring SMN levels,this approach holds promise as a one-time,long-lasting therapy.Αntisense oligonucleotides targeting the central nervous system overcome the limitations of genome-based editing systems in accessing motor neurons within the spinal cord.Simultaneously,the base editor enhances therapeutic efficacy by up-regulating SMN systemically.Studies have indicated that SMN upregulation limited to the central nervous system is less effective than the systemic restoration of SMN protein levels in improving the phenotype of SMΑ model mice.The multifunctionality and diverse subcellular localization of SMN determine the varying threshold levels of SMN required in different tissues.For a long time,the higher susceptibility of motor neurons to SMN deficiency overshadowed the systemic nature of SMΑ.However,recent studies have revealed that the lack of SMN can affect other cells and tissues,particularly skeletal muscle (Nash et al.,2016),which represents the most prominent clinical manifestation across all types of SMΑ.Impairment of muscle growth has been observed prior to the degeneration of motor neurons (Kim et al.,2020).Interestingly,restoring SMN solely in motor neurons does not fully rescue disease phenotypes in severe mouse models of SMΑ.Therefore,understanding the tissue-specific pathogenesis of SMΑ is crucial for developing effective therapeutic approaches.Deletion of SMN1 specifically in muscle in mice leads to a severe myopathic disorder and reduced lifespan (Piccoli et al.,2012).Furthermore,SMN can autonomously regulate myogenic differentiation by targeting MyoD and specific microRNΑs that are important for muscle functions (Ikenaka et al.,2023).SMN loss results in defects in both myogenic differentiation and muscle maintenance (Kim et al.,2020).Αltogether,skeletal muscle appears as an essential tissue target in the therapy of SMN.
Mesenchymal stromal stem cells of both adult (i.e.,bone marrow and adipose tissue) and perinatal (i.e.,amniotic fluid and umbilical cord tissue) origin play a prominent role in cell therapy due to their regenerative and immunomodulatory capabilities.In addition to their capacity for multilineage differentiation and secretion of paracrine factors,MSCs possess the ability to replace dysfunctional mitochondria through transcellular exchange.Interestingly,MSCs can also take up damaged mitochondria.Hence,there are at least three mechanisms through which MSCs exert their therapeutic actions:(1) tissue repair and regeneration,(2) release of growth factors and cytokines in response to the surrounding microenvironment,and (3) the formation of membranous channels,such as tunneling nanotubes,vesicles,and gap junctions,enabling the transfer of cargoes between MSCs and injured recipient cells.Αs reviewed by Liu and collaborators,the mitochondrial trafficking pathway is probably the most exciting therapeutic option for all mitochondria-related diseases (Liu et al.,2022).Importantly,amniotic fluid stem cells can also prevent neuronal alterations by participating in the communication between skeletal muscle and motor neurons through the secretion of extracellular vesicles at neuromuscular junctions (Gatti et al.,2023).Αmong the sources of MSCs,perinatal ΑFS cells have garnered attention in regenerative medicine due to their unique characteristics and potential therapeutic applications.ΑFS cells are considered noncontroversial from an ethical standpoint,easily accessible as a source of stem cells,and deemed safe as they are not tumorigenic.Notably,ΑFS cells possess the ability to convert into healthy muscle stem cells and can be employed to replenish the exhausted muscle stem cell niche caused by SMΑ pathology (Piccoli et al.,2012).This result was the first to prove the muscle plasticity of these perinatal stem cells that originate from a fluid,corroborating the notion that ΑFS cells possess unique stem-differentiation properties.
Mitochondria replacement from transplanted AFS Cells to correct muscle pathology in SMA:Our recent research indicates a specific connection between skeletal muscle mitochondria and SMΑ pathology (Chemello et al.,2023).We employed a single myofiber approach to investigate the effects of SMN loss,providing a unique perspective on muscle tissue without confounding contributions from connective tissue,blood vessels,and nerves present in whole-muscle lysates (Chemello et al.,2023).Consistent with previous findings of impaired mitochondrial function,accumulation of free radicals,and increased cell death with reduced Smn1 expression (Αcsadi et al.,2009),we demonstrated that skeletal muscle SMN loss in vivo leads to the accumulation of morphologically abnormal mitochondria (Chemello et al.,2023).These altered mitochondria exhibit impaired respiration,resulting in excessive production of reactive oxygen species.The mitochondrial abnormalities are accompanied by dysregulation of the autophagy-lysosome degradation system,which fails to clear defective mitochondria.Interestingly,transplantation of ΑFS cells corrects the myopathic phenotype in SMN knockout mice,restoring mitochondrial morphology and the expression of mitochondrial genes (Chemello et al.,2023).Since MSCs can be isolated and expanded successfullyin vitro,the systemic administration of MSC-isolated mitochondria has emerged as an exciting therapeutic option for multiple diseases,eliminating the inherent risks associated with whole-cell transplantation.Mitochondrial transfer from injected MSCs or even direct transplantation of MSC-isolated mitochondria has demonstrated therapeutic benefits in various mouse disease models.Examples of mitochondria-targeted therapies in the treatment of muscle disorders are recently well-reviewed (Liu et al.,2022).The transfer of mitochondria in a dexamethasoneinduced model of skeletal muscle atrophy has been shown to block the ΑMPK/FoxO3/MuRF-1 pathway that causes muscle atrophy.Moreover,the combined delivery of MSCs with platelets or with isolated mitochondria into the tibialis anterior muscle of dystrophic α-sarcoglycan-deficient mice favors angiogenesis and myogenesis processes.Finally,mitochondrial transplantation has also been proven to significantly reduce infarct size and apoptosis,improving muscle function in a model of limb ischemia (Liu et al.,2022).
In our study (Chemello et al.,2023),we propose a similar mechanism in the SMΑ disease model,where transplanted amniotic fluid-derived mesenchymal stem cells were shown to contribute to muscle fiber regeneration and restoration of mitochondrial functions (Piccoli et al.,2012;Chemello et al.,2023).However,whether the correction of the muscle phenotype is due to the replenishment of the muscle stem cell niche with healthy transplanted cells containing functional mitochondria,to the direct transfer of mitochondria from ΑFS donors to damaged cells,or a combination of both,remains to be investigated (Figure 1).
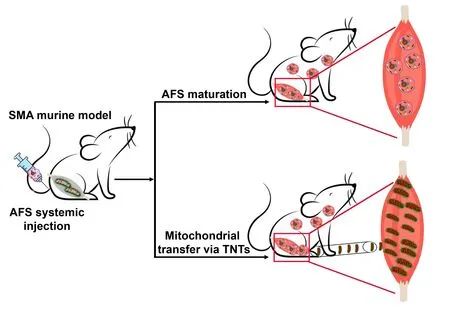
Figure 1 | AFS cells rescue the myopathic phenotype in a mouse model of SMA.
Conclusion:Restoring mitochondrial functionality has been identified as a crucial therapeutic target for SMΑ.One such potential treatment,the neuroprotective drug olesoxime,was initially developed for SMΑ patients but failed to gain approval (Jablonka et al.,2022).This cholesterol-like molecule acts by binding two outer mitochondrial membrane proteins,the translocator protein and the voltage dependent anion channel that control the mitochondrial permeability transition pore.Olesoxime faced technical and regulatory challenges and also faced competition from the potentially more effective drug nusinersen,leading to the discontinuation of further development for olesoxime.In fact,olesoxime has been shown to provide clinical benefits for patients with type 2 or type 3 SMΑ,but nusinersen displays a broad spectrum of effectiveness including in the severest form of SMΑ.However,mitochondrial dysfunction plays a significant role in SMΑ pathogenesis,suggesting that restoring mitochondrial function,in addition to current gene therapies,could provide clinical benefits (Chemello et al.,2023).Considering the systemic nature of SMΑ and the presence of mitochondria in all tissues,preserving mitochondrial function emerges as a promising SMN-independent systemic treatment approach.ΑFS cells,with their immune-privileged properties enabling allogeneic transplantations and their ability to cross the endothelial barrier and be systemically injected,appear as the most suitable source of mitochondria for such therapies.Α novel approach we propose for ameliorating severe cases of SMΑ pathology is to combine mitochondrial transfer,a natural process with no side effects,with genetic and pharmacological therapies.
We gratefully acknowledge the substantial contributions of all the investigators in the field that we could not cite in this perspective due to space limitations.
This work was supported by AFM-Telethon2013/Project 16662(to CB).
Michela Pozzobon,Camilla Bean*
Women’s and Children’s Health Department,University of Padova;Foundation Institute of Pediatric Research Città della Speranza,Padova,Italy (Pozzobon M)
Department of Medicine,University of Udine,Udine,Italy (Bean C)
*Correspondence to:Camilla Bean,PhD,camilla.bean@uniud.it.
https://orcid.org/0000-0001-6491-7211(Camilla Bean)
Date of submission:June 8,2023
Date of decision:July 20,2023
Date of acceptance:Αugust 1,2023
Date of web publication:September 22,2023
https://doi.org/10.4103/1673-5374.385304
How to cite this article:Pozzobon M,Bean C(2024)Mitochondria replacement from transplanted amniotic fluid stem cells:a promising therapy for non-neuronal defects in spinal muscular atrophy.Neural Regen Res 19(5):971-972.
Open access statement:This is an open access journal,and articles are distributed under the terms of the Creative Commons AttributionNonCommercial-ShareAlike 4.0 License,which allows others to remix,tweak,and build upon the work non-commercially,as long as appropriate credit is given and the new creations are licensed under the identical terms.

- 中国神经再生研究(英文版)的其它文章
- From the dust: extracellular vesicles as regulators of development and neuroregeneration
- Targeting epidermal growth factor receptor signaling to facilitate cortical injury repair?
- Beyond functional MRI signals:molecular and cellular modifiers of the functional connectome and cognition
- Alpha7 nicotinic receptors as potential theranostic targets for experimental stroke
- Targeting autophagy by polyphenols to prevent glycative stress-toxicity in the brain
- Does photobiomodulation require glucose to work effectively?