
Effectiveness and the nomogram of small incision lenticule extraction in the correction of myopic anisometropia in adults
2023-11-10 04:05TongZhangLuZhuHangJiaZuoZhiJunChenYanJiXinYangXiaoRongLuQiongWuQingWangJiuYiXiaMengLiChunJiangZhouYaoWangKeHuWenJuanWan
Tong Zhang, Lu Zhu,2, Hang-Jia Zuo,2, Zhi-Jun Chen,2, Yan Ji,2, Xin Yang,2, Xiao-Rong Lu,2,Qiong Wu,2, Qing Wang,2, Jiu-Yi Xia,2, Meng Li,2, Chun-Jiang Zhou,2, Yao Wang,2,Ke Hu,2, Wen-Juan Wan,2
1Chongqing Medical University, Chongqing 400000, China
2The First Affiliated Hospital of Chongqing Medical University, Chongqing Key Laboratory of Ophthalmology,Chongqing Eye Institute, Chongqing Branch (Municipality Division) of National Clinical Research Center for Ocular Diseases, Chongqing 400000, China
Abstract
● KEYWORDS: refractive surgery; small incision lenticule extraction; anisometropia; nomogram
INTRODUCTION
Anisometropia refers to the unequal refraction of two eyes, which manifests as a difference in refractive errors or properties.Mild differences in refraction are common and usually do not cause clinical symptoms.Obvious anisometropia may cause stereoscopic dysfunction, asthenopia,strabismus, or amblyopia[1].Absolutely equal refraction in both eyes is rather rare in general population, according to studies conducted in different regions, the incidence of this common refractive abnormality ranges from 3.79% to 21.8%[2-3].Furthermore, many cases of anisometropia are ignored owing to the lack of vision abnormalities, such as amblyopia.
In addition to optical correction, refractive surgery is also one of the current ways to treat anisometropia.Refractive procedures, such as photorefractive keratectomy, laserin situkeratomileuses, laser-assisted subepithelial keratectomy, and phakic intraocular lens implantation treatments have been reported to be safe and effective in treating anisometropia and even anisometropic amblyopia, which have been shown to improve visual acuity, binocular vision in patients with anisometropia[2,4].
Previous studies have well documented that small incision lenticule extraction (SMILE) has become one of the preferred surgical modalities for people suffering from anisometropia due to its safety, efficacy, predictability, and fewer postoperative flap-related complications[1,5-8].The implantation of implantable collamer lenses (ICL) has emerged as a promising approach for the correction of high myopic anisometropic amblyopia in adults[9].ICL implantation and SMILE have similar and comparable outcomes in term of the efficacy and predictability for correcting high myopia[10].Some children and adolescents with stereoscopic dysfunction caused by anisometropia can also benefit from various cornea refractive surgeries including SMILE and laser-assistedin situkeratomileusis[11-12].However, myopic anisometropia in adult patients whose visual development has been completed, the effect of SMILE on stereoscopic function has been rarely reported in the literature,so this article will evaluate the efficacy of SMILE correction of myopia refractive error aged 18 years old or older (including stereoscopic function).In addition, in order to reduce the tendency for undercorrection after cornea refractive surgery in patients with high myopia, a part of refractive surgery centers at home and abroad have included nomogram in the parameters of adjusting target spherical equivalent (SE)[1,5,13-15].Therefore, this study also explores the personalized design scheme of SMILE in correcting adult myopia anisometropia based on the nomogram, to inform future clinical applications of SMILE in refractive error correction.
SUBJECTS AND METHODS
Ethical ApprovalThe study protocol was approved by the Ethics Committee of the First Αffiliated Hospital of Chongqing Medical University (ethical approval number: 2020-376),which adhered the principles of the Declaration of Helsinki.After explaining the nature of the study and the possible consequences, written informed consent for the procedure was obtained from patients and their immediate family members.Research ObjectThis was a prospective cohort study.This study included 45 patients with myopic anisometropia.Among them, 8 eyes with emmetropia were not operated on, and 37 patients underwent SMILE treatment for both eyes.All patients underwent SMILE at the Ophthalmology Department of the First Affiliated Hospital of Chongqing Medical University(Chongqing, China) between September 2020 and March 2021 were included.
Inclusion and Exclusion CriteriaThe inclusion criteria included a minimum age of 18y, no previous ocular surgery history, normal corneal topography, stable refraction for at least 2y.Patients with binocular myopic anisometropia having an SE greater than or equal to 2.0 D.The logMAR corrected distance visual acuity (CDVA) in both eyes was equal to or better than 0.1, and the corrected spherical power of each eye was within the range of -9.0 D to -0.25 D.The patients with other ocular or systemic organic diseases and pregnant or lactating women were excluded.
NomogramTo develop an individualized surgical plan, the nomogram was derived from the formula as follow:
SEerror=0.25+0.11×SEpreoperative.
And we slightly adjusted according to age, sex, accommodation status, surgeon’s experience and hospital environment,etc.[16-17].A respectively lower nomogram was designed in eyes with higher myopia compared with that of the contralateral eyes.
Surgical MethodsThree days before surgery, all surgical patients were administered sodium hyaluronate eye drops(10 mL: 0.1%, Hylo-comod®, RSAPHARM Arzneimittel GmbH, Industriestraße, Saarbrücken, Germany) and levofloxacin eye drops (5 mL: 24.4 mg, Cravit®, Santen, Osaka,Japan) four times a day.Intraoperatively, oxybuprocaine hydrochloride eye drops (20 mL: 80 mg, Benoxil®, Santen,Osaka, Japan) were administered twice for topical anesthesia.VisuMax femtosecond laser system (Carl Zeiss Meditec AG,Jena, Germany) was used for surgical refractive corrections for all patients with pulse frequency of 500 kHz and pulse energy of 135 nJ.The spot size was 4.3 μm and optical zone diameter ranges from 6.0 to 6.7 mm.The corneal cap diameter ranged from 6.8 to 7.5 mm, and cap thickness was 120 μm.The incision length was 2.8 mm, position of incision was 90°,and the edge cutting angle was 90°.Αfter the canning, microseparator was used to separate and lift the edge of the corneal cap, and separate the front and back surfaces of the lens in turn.Then, the stromal lens was removed by micro tweezers from the small incision and the wholeness of stromal lens was carefully checked.Before the surgery was completed, extra water was absorbed by sterile sponge.
Postoperative TreatmentTobramycin and dexamethasone eye drops (TobraDex®, Novartis, Rijksweg, Puurs, Belgium)were given immediately after surgery for four times, every ten minutes.Other postoperative regimens were follows: 0.5%levofloxacin eye drops, four times a day for 21d; tobramycin dexamethasone eye drops, four times a day for one week,and then replaced with loteprednol eye drops (5 mL: 0.5%,Lotemax®, Bausch & Lomb Incorporated, Tampa, Florida,USA), 3 times a day for one week, then twice a day for one week, and then once a day for one week; sodium hyaluronate eye drops, 4 times a day for one month.
Follow-up IndicatorsBefore the operation, patients underwent the anterior segment under slit lamp examination and the fundus examination under the indirect ophthalmoscope,and compound tropicamide eye drops (1 mL, Zhuobi’an®,Sinqi Pharmaceutical, Shenyang, China) used to dilate the pupil.The distance vision both before and after the operation were detected with the logMAR chart; corneal topography was obtained by performing Pentacam®AXL panoramic biometer(Oculus GmbH, Wetzlar, Germany); and Titmus Stereoacuity Test was applied to examine stereoscopic function.The dilated and small pupil tests were run by the same experienced optometrist.SE was obtained by adding the sum of the sphere power with half of the cylinder power.
Tests were conducted before the surgery and follow-ups were arranged at 1wk, 1, 3, and 6mo after surgery.Followup indicators include: uncorrected distance visual acuity(UDVΑ), CDVΑ, refractive error, effectiveness index (defined as preoperative CDVA/postoperative UDVA), safety index(defined as postoperative CDVA/ preoperative CDVA)[18],stereoscopic function, nomogram and complications.All missing data came from lost follow-up, and the small number of lost samples did not affect statistical analysis method.
Statistical AnalysisSPSS 17.0 (IBM Corp., Armonk, NY,USA) software was used to perform data processing and analysis.Data are presented as mean±standard deviation(SD).The Shapiro-Wilk test was used for normal distribution analysis.Pairedt-test and repeated-measures analyses of variance were applied to continuous normally distributed variables, and Wilcoxon signed-rank test was used for groups with non-normally distributed continuous variable.Pearson Chi-squared test were used for categorical variables.Pvalues<0.05 were considered indicative of statistical significance.PASS 15.0 (NCSS, Utah, USA) software was used to estimate the sample size.The sample size was calculated to detect a tolerance of 0.05; set alpha=0.05 (twosided), with a confidence level (1-α) of 95%; assuming SD of efficacy index and safety index after SMILE to 0.2 according to previous study[19], and 80 eyes were required.
RESULTS

Figure 1 Cumulative percentage of preoperative logMAR CDVA and postoperative UDVA Preop.: Preoperative; Postop.: Postoperative;CDVA: Corrected distance visual acuity; UDVA: Uncorrected distance visual acuity.
Baseline InformationThe study included 45 consecutive patients (average age: 25.0±6.9y).Among them, 24 (53.3%)were males and 21 (46.7%) were females.We finally evaluated 82 out of 90 eyes (45 patients) undergoing SMILE, while 8 emmetropia eyes was not operated, and 37 patients underwent SMILE treatment for both eyes.The average preoperative SE was -4.74±0.22 D (range -1.13 to -9.63 D).The average of refractive error of eyes with higher myopia (-6.37±1.43 D)was significantly higher than that of eyes with lower myopia(-3.48±1.41 D,P<0.001).Among 37 patients who underwent surgery in both eyes, 22 cases (59.5%) had higher myopia in the right eye, which was significantly higher than that in the left eye (15 cases, 19.5%;P=0.104).During the operation,mild diffuse opaque bubble layer (OBL) occurred in 2 eyes(2.4%).There were no other intraoperative or postoperative complications.
Effectiveness of SurgeryPreoperative logMAR CDVA of all eyes was better than 0.1, with 37 (45.1%) of them having a better value than -0.1.Six months after the operation, all eyes had postoperative UDVA of 0.1 or better; 79 eyes (96.3%) had UDVA of 0.0 or better, 58 (70.7%) eyes had UDVA of -0.1 or better, and 3 eyes (3.7%) had UDVA of -0.2 or better (Figure 1).The effectiveness index 6mo after surgery was 1.05±0.12.Surgery SafetyOne week after the surgery, 75 (91.5%)eyes had logMAR CDVA equal or better than that under the preoperative situation; the number of eyes with CDVA equal or better than that under the preoperative situation at postoperative 1, 3, and 6mo were 78 (95.1%), 80 (97.6%), and 81(98.8%), respectively.The number of eyes with CDVA that gained 1 line and 2 lines six months postoperatively were 33(40.2%) and 1 (1.2%) respectively.The number of eyes whose CDVA decrease 1 line six months after surgery was 1 (1.2%).None of the cases showed CDVA decreasing 2 lines or more(Figure 2).The safety index was 1.09±0.11 six months after the surgery.
Predictability of SurgerySix months after the surgery, 70(85.4%) eyes showed SE correction error within ±0.5 D; 11(13.4%) eyes showed SE correction error ranging from ±0.5 D to 1.0 D (Figure 3).The linear regression equation of actual SE and pre-corrected SE at 6mo after surgery is y=0.9340x-0.3635(R2=0.9582,P<0.0001; Figure 4).
The numbers and percentages of eyes with different levels of postoperative astigmatism six months after surgery were as follows: 0.00-0.50 D, 66 eyes (80.5%); 0.51-1.00 D, 16 eyes(19.5%); 1.01-1.50 D and >1.51 D, none (Figure 5).

Figure 2 The changes in lines of logMAR CDVA after SMILE surgery Preop.: Preoperative; Postop.: Postoperative; CDVA: Corrected distance visual acuity.

Figure 3 Accuracy of spherical equivalent refraction after SMILE surgery Preop.: Preoperative; Postop.: Postoperative.

Figure 4 Achieved versus attempted change in SE 6mo after SMILE surgery SE: Spherical equivalent; D: Diopter.
Stability of SurgeryFigure 6 shows the SE refraction changes over time after SMILE surgery.Compared with the preoperative data, there was a significant reduction in the mean SE at 1wk, 1, 3, and 6mo postoperatively (P<0.05).However,no statistical difference of mean SE was detected between different points of time after operation.

Figure 5 Percentage of preoperative and postoperative refractive astigmatism Preop.: Preoperative; Postop.: Postoperative; D: Diopter.
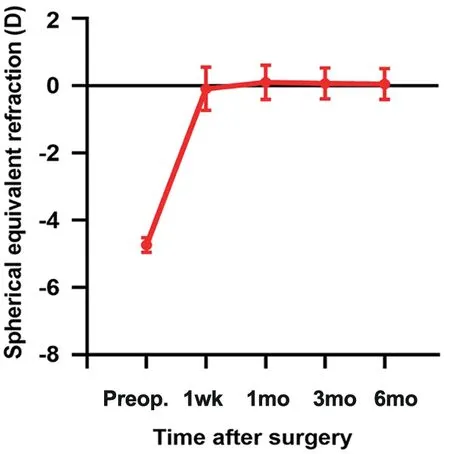
Figure 6 Stability of spherical equivalent refraction.
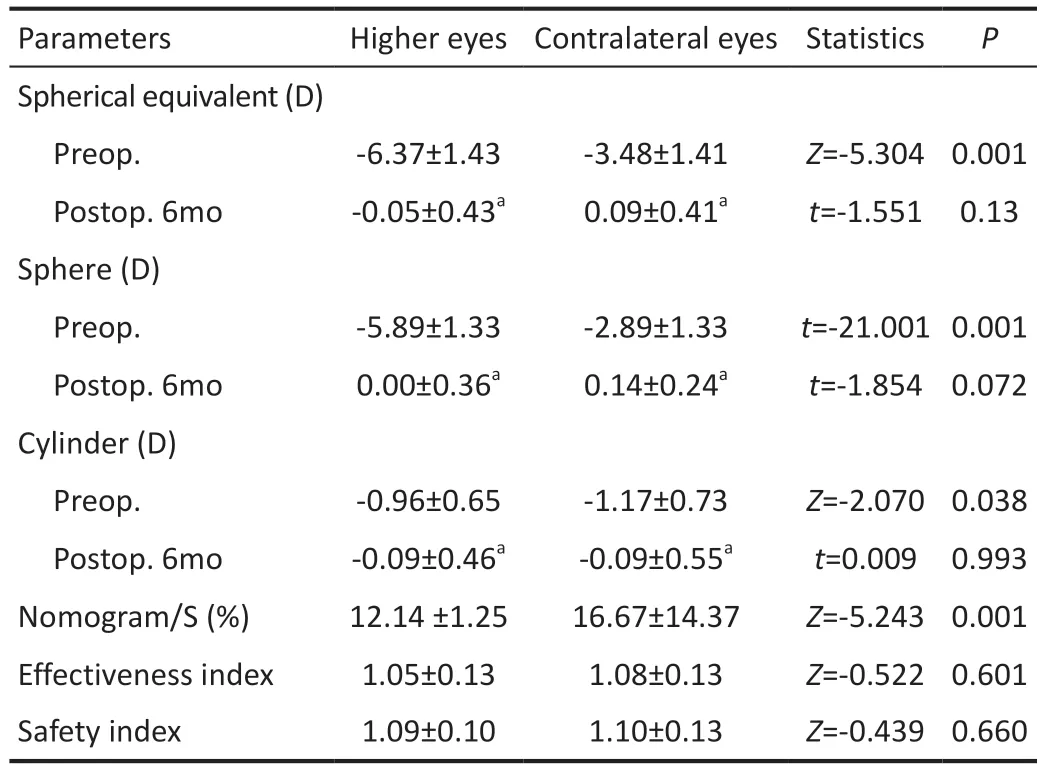
Table 1 The refractive outcomes of higher eyes versus contralateral eyes before and after SMILE
Comparison Between Eyes with Higher Myopia andContralateral EyesTable 1 shows the outcomes of higher eyes versus contralateral eyes before and after SMILE among 37 patients who underwent SMILE in both eyes.The average nomogram value/spherical refraction ratio of the eyes in higher myopia was 12.14%±1.25%; this data in contralateral eyes was 16.67%±14.37%; there was significant difference between higher myopia eyes and contralateral eyes (P<0.001).Six months after surgery, the average SE of eyes with higher myopia was -0.05±0.43 D, while that of the contralateral eyes was 0.09±0.41 D, suggesting no significant difference between the two eyes in this respect (P=0.13).Αlso, the difference of effectiveness index as well as safety index between higher eyes versus contralateral eyes postoperatively was not statistically meaningful.
Stereoscopic FunctionWe recorded the Titmus stereoscopic examination of 45 patients.On preoperative Titmus stereoscopic examination, 12 patients (26.7%) had a stereoscopic function ≥ 600”, and 25 cases (55.6%) had a stereoscopic function ≤ 200”.Six months after surgery, the proportion of eyes with stereoscopic vision ≥600” (2 cases,4.4%) was significantly reduced (P=0.006), and the proportion of eyes with stereoscopic vision equal or less than 200” (40 cases, 88.9%) was significantly increased (P<0.001).
DISCUSSION
Refractive surgery poses unique advantages over other treatment of anisometropia.Compared with spectacles, it could offer better visual quality and cause less optically-induced aniseikonia.Also, it may protect patients against infection when compared with contact lenses.Characterized as no corneal flap-related complications[20], SMILE is reported to induce less damage to the corneal subepithelial stromal nerve plexus, have a mild surgical response, and it is less likely to cause dry eyes[21-22].Therefore, it is gradually becoming one of the mainstream refractive surgeries.We found that SMILE is not only a safe, effective and predictable method for correcting adult myopic anisometropia, but it also alleviates refractive differences and in turn helps improve the stereoscopic function of these patients.Nomogram design may provide better refractive outcomes for SMILE surgery with anisometropic eyes.
Studies have demonstrated the long-term safety and effectiveness of SMILE[23-26], and it is a promising modality for improving adult myopic anisometropia[27].Anget al[19]pointed out that, one year after SMILE, in 98.0% of cases,the CDVA was equal to or better than that before surgery, and the efficacy index was 0.99±0.20.In Taneriet al’s[28]study, at 3mo after SMILE surgery 96.0% cases had CDVA equal or better than before the surgery, and the mean efficacy index was 1.03.Our results reported that the data was 98.8% 6mo after SMILE surgery, and the efficacy index was 1.05, both similar to previous results, thereby confirming the safety and efficacy of SMILE in correcting myopia refractive error in adults.In addition, the excellent performance of SMILE surgery in terms of predictability has also been confirmed by previous studies.Zhonget al[25]and Sánchez-Gonzálezet al[29]reported that SE correction error within ±0.5 D was 81.4%-83.9% and 83.0%,respectively, which is also very close to our 85.4%, confirming the predictability of SMILE in the correction of myopic anisometropia.
Of note, obvious anisometropia may cause amblyopia,whereas some patients with anisometropia only present with stereoscopic dysfunction[1].Indeed, there is considerable inter-individual variability with respect to tolerance to anisometropia, and lower levels of anisometropia do not cause obvious abnormalities in visual development[30-31].Nonetheless,a significant proportion of patients with anisometropia are affected by stereoscopic dysfunction.It was reported that children and adolescents with myopic anisometropic amblyopia exhibited different degrees of improvements of their already lost stereoscopic function after refractive surgical correction[12,32-33].There is also a possibility that anisometropia correction surgery improves vision and visual function in adults with anisometropic amblyopia, even though they have missed the critical period of visual development[2,12].These potential visual abnormalities, visual fatigue and other discomforts are often overlooked in daily lives.It underlines the importance of paying more attention to individuals who have normal vision but exhibit abnormal visual function.Our study shows that SMILE surgery can improve stereoscopic function in adults with myopic anisometropia, which is consistent with previous views.
In previous studies on corneal refractive procedures, including SMILE for the correction of myopic anisometropia, it was found that eyes with high myopia were more likely to be under corrected, and the effectiveness was worse than that of the contralateral eyes[13,34-35].This may be related to the asymmetric eye adjustment ability of the eyes with anisometropia, the greater movement adjustment ability of the eyes with higher myopia, and the thicker ciliary muscle of the eyes with higher myopia in case of anisometropia[13].Nowadays, more attention has been paid to nomogram to adjust the corrected refractive error of SMILE.Different nomogram designs for anisometropia can help improve the predictability of surgery.It has been previously reported that the tendency of undercorrection after corneal refractive surgery in high myopia patients disappeared after adjusting results according to nomogram[13-15,36].In our study, we determined the individualized nomogram before surgery according to the factors such as preoperative sphere refraction, age, sex,surgeon’s experience, hospital environment,etc.Furthermore,no difference was observed between the SE of eyes with higher myopia and that of the contralateral eyes.Furthermore,other factors that affect the predictability of SMILE (including astigmatism and axial, corneal curvature, tear filmetc.)deserve our attention[17,37].Αpplication of artificial intelligence technology in the nomogram design of SMILE surgery will provide a more accurate solution for the individualized design of the surgery for patients with anisometropia[38].
Nevertheless, the study still has some limitations.Nomogram for the correction of myopic anisometropia based on deep learning algorithms, large sample size and long-term follow up should be conducted in the future.A larger prospective cohort study investigating the factors related to the recovery of visual function after SMILE will provide more definitive evidence.
Our findings suggest that SMILE is a predictable, effective,and safe modality for correcting myopic anisometropia.For anisometropia in adults, the correction of refractive differences can bring about an improvement in stereoscopic function.The precise and individualized design of the nomogram is a vital element to ensure the balance of both eyes after SMILE.
ACKNOWLEDGEMENTS
Foundations:Supported by the National Natural Science Foundation of China (No.81970832; No.81870650);the Key Project of the Chongqing Health Commission(No.2018MSXM003; No.2018GDRC008); Natural Science Foundation of Chongqing Science and Technology Bureau(No.cstc2021jcyj-msxmX0967).
Conflicts of Interest: Zhang T,None;Zhu L,None;Zuo HJ,None;Chen ZJ,None;Ji Y,None;Yang X,None;Lu XR,None;Wu Q,None;Wang Q,None;Xia JY,None;Li M,None;Zhou CJ,None;Wang Y,None;Hu K,None;Wan WJ,None.
 International Journal of Ophthalmology2023年11期
International Journal of Ophthalmology2023年11期
- International Journal of Ophthalmology的其它文章
- Quantitative analysis of optic disc changes in school-age children with ametropia based on artificial intelligence
- Association analysis of Bcll with benign lymphoepithelial lesions of the lacrimal gland and glucocorticoids resistance
- In vitro protective effect of recombinant prominin-1 combined with microRNA-29b on N-methyl-D-aspartateinduced excitotoxicity in retinal ganglion cells
- Bioinformatics and in vitro study reveal the roles of microRNA-346 in high glucose-induced human retinal pigment epithelial cell damage
- Therapeutic effect of folic acid combined with decitabine on diabetic mice
- Comparison of visual performance with iTrace analyzer following femtosecond laser-assisted cataract surgery with bilateral implantation of two different trifocal intraocular lenses