
Comparison of visual performance with iTrace analyzer following femtosecond laser-assisted cataract surgery with bilateral implantation of two different trifocal intraocular lenses
2023-11-10 04:05RuiHongJuHaoKunQuZheMingWuYunChenLiNanWuYuanLongZhengWang
Rui-Hong Ju, Hao-Kun Qu, Zhe-Ming Wu, Yun Chen, Li-Nan Wu, Yuan Long, Zheng Wang
Aier Eye Hospital, Jinan University, Guangzhou 510071,Guangdong Province, China
Abstract
● KEYWORDS: femtosecond laser-assisted cataract surgery; visual performance; binocular; AT LISA tri839MP;AcrySof PanOptix TFNT00; iTrace
INTRODUCTION
Cataract remains the most common cause of blindness in the world[1-2].Surgery is the only effective treatment at present, which has a profound impact on patients’ quality of life.Conventional phacoemulsification is the most prevalent way of cataract surgery in many countries.With the development of technology, femtosecond laser has been recently applied to cataract surgery, particularly for corneal incision, anterior capsulotomy and phacofragmentation.However, there are still some controversial viewpoints in the two main surgery methods, especially in the potential benefits and cost-effectiveness[3-5].Intraocular lens (IOLs)implantation following cataract surgery can provide spectacle independence at all distances after surgery, which is also a refractive procedure[6].The majority of patients undergoing cataract surgery also suffer from presbyopia, a refractive disorder that affects the ability to see close clearly due to the crystalline lens’s physiological degenerative changes as they age (common in adults older than 40)[7-8].Through advances in IOL technology, patients with presbyopia could be corrected or mitigated during cataract surgery and achieve a stable and functional uncorrected vision without spectacles at all distances[9-11].Trifocal IOLs are designed to improve the whole-course vision.In China, there are two commonly used trifocal IOLs: AT LISA tri839MP (Carl Zeiss, German)and AcrySof IQ PanOptix TFNT00 (Alcon, USA).These two IOLs have demonstrated excellent visual performances after cataract surgery in multiple clinical trials around the world,with low rates of serious and non-serious complications[12-16].The postoperative visual performances includes not only subjective ones such as visual acuity at different distances,contrast sensitivity and visual functioning questionnaires, but also objective ones such as aberrations, modulated transfer function (MTF), point spread function (PSF), Strehl ratio (SR)and so on.
At present, there are few reports about the comparison of both subjective and objective binocular visual performance after bilateral implantation of these two different types of diffractive trifocal IOLs especially following femtosecond laser-assisted cataract surgery (FLACS).In this study, we aim to compare the postoperative subjective visual outcomes, objective visual performances using by iTrace analyzer and safety aspects,which were obtained after bilateral implantations of the AT LISA tri839MP and AcrySof IQ PanOptix TFNT00 during FLACS.
SUBJECTS AND METHODS
Ethical ApprovalEthics approval was granted by the ethics committee of Aier Eye Hospital, Jinan University (Guangzhou,China; No.GZAIERIRB2020003), which followed the Helsinki Declaration.Written informed consent forms were obtained from all participants.
Ophthalmic ExaminationsAll ophthalmic examinations were performed by qualified technicians or doctors.Surgical, preoperative and postoperative data were collected retrospectively.Patients all underwent the second eye surgery within 2wk after the first one and received the routine ophthalmic examinations before surgery and were followed-up at 1d, 1wk, 1, and 3mo after the second eye surgery.Regular perioperative examinations included uncorrected distance visual acuity (UDVA, at 5 m), uncorrected near visual acuity(UNVA, at 30 cm and 40 cm), uncorrected intermediate visual acuity (UIVA, at 60 cm and 80 cm), spherical equivalent (SE),intraocular pressure (IOP), slit-lamp microscopy, and objective performances (total MTF10, MTF30 and the average height with or without correction, SRs with or without correction and HOAs) at every visit.Visual acuity was measured in decimal visual acuity under photopic conditions using international standard logarithmic eye chart (GB11533-2011) and then converted into the logarithm of minimum angle of resolution(logMAR) notation.The SEs were recorded by automatic optometry at very visit.The axial length (AL) was measured by IOL Master 700 (Carl Zeiss, Germany) before operation.The IOL power was calculated by Barrett Universal II formula, and target diopter was set between 0 and -1.0 D to account for the farsighted drift in the long axis eyes.Objective visual qualities were recorded by the iTrace analyzer (Tracey Technologies,USA), which is a powerful device using ray tracing to analyze visual function and sources of aberrations[17-18].
The total MTF10, MTF30 and the average height with or without correction, SRs with or without correction and HOAs(coma, spherical, secondary astigmatism, trefoil) were recorded at a 3-mm pupil size before surgery and 1wk, 1, and 3mo after surgery.The average data were taken after 3 measurements.
Study LensesThe AT LISA tri839MP is a trifocal (+3.33 D for near; +1.66 D for intermediate), clear, aspheric (-0.18 μm),aberration-correcting IOL, which was made of 12%hydrophilic acrylate with hydrophobic surface.The IOL size is 11 mm, with a diffractive front surface and an optical diameter of 6 mm, in which a central 4.3 mm area with trifocal design,and the surrounding area with bifocal design, and its inner ring optical diameter is 1.04 mm.The range is from 0 to +32.0 D.
The AcrySof IQ PanOptix TFNT00 is another trifocal(+3.25 D for near; +2.17 D for intermediate), yellow, aspheric(-0.10 μm), aberration-correcting IOL, which was made of hydrophobic acrylate/methacrylate copolymer.The IOL size is 13 mm, with an optical diameter of 6 mm and a diffractive region of 4.5 mm, and its inner ring optical diameter is 1.164 mm.The range is from +6.0 to +34.0 D.
Surgical ProceduresAll FLACSs were performed as following: patients under topical anesthesia (Benoxil; Santen Pharmaceutical Co.Ltd., China) lay on the operating bed, the femtosecond laser was used to perform capsulorhexis (5.0 mm)and nucleus fragmentation (energy parameter, 10 μJ) (LenSx;Alcon Laboratories, USA).A 2.2 mm main corneal incision and a 1.0 mm side incision were made manually.The anterior chamber was then filled with viscoelastic agent, and the isolated anterior capsule was removed and separated.
A phaco procedure was performed using the Centurion Vision System with Active Fluidics (Alcon Laboratories,USA).During I/A mode, residual cortices were sucked,anterior and posterior capsule were polished.Then an IOL(AT LISA tri839MP or AcrySof IQ PanOptix TFNT00) was implanted and adjusted to a normal position in the capsular bag.Following removal of the viscoelastic agent, the puncture site was hydrated to form anterior chamber.At the end of surgery, the Purkinje reflex was checked to ensure the optimal centralization of the IOLs in all patients.The operative eyes were bandaged after usage of dexamethasone and tobramycin eye ointment (Tobradex, Yangtze River Pharmaceutical Group Co.Ltd., China).
The same experienced surgeon (Wu ZM) performed all surgical procedures with the same equipment and instruments.All patients received topical levofloxacin (Shentian Pharmaceutical Co., Ltd., China) and diclofenac sodium eye drops (Shenyang Xingqi Pharmaceutical Co., Ltd., China) 4 times daily for 3d before surgery.The standard postoperative treatment was same to each eye and consisted of topical tobradex (0.3%tobramycin and 1% dexamethasone, Alcon, USA) 4 times per day for 2wk, and pranoprofen (Yangtze River Pharmaceutical Group Co., Ltd., China) 4 times per day for 2wk.
金融机构尤其是商业性金融机构以利润最大化为目标,以追求盈利和市场业绩为目的,商业性金融机构资金的流动方向始终与利润的高低保持紧密的联系,受资本约束影响较大。银监发〔2011〕34号文规定“针对全覆盖、基本覆盖、半覆盖和无覆盖平台贷款,自2011年一季度起做到分别按照100%、140%、250%、300%计算贷款风险权重,发挥资本约束作用”。而水利项目具有建设资金需求量大、偿还周期长、项目收益率低的特点,与商业性金融机构经营目标及监管要求相悖,因此在财政补偿机制不完善的情况下,水利项目尤其是公益性项目,很难吸引商业性金融机构较大规模的信贷投放。
Sample SizeBefore the research starts, we calculated the sample size according to our previous clinical observational results.UDVA outcome was observed 0.01±0.03 logMAR in the TFNT group and 0.04±0.03 logMAR in the tri839 group during 1mo follow-up.So, the mean and average values were set 0.01±0.03 and 0.04±0.03 respectively in experimental group and control group.The K value (experimental group sample size/control group sample size), alpha and power were set 1:1, 0.05 and 0.9 respectively.Based on these assumptions,16 eyes were required in each group.Assuming the loss rate of the subjects is 20%, finally the sample size is at least 20.
Statistical AnalysisAll statistical analyses were conducted using SPSS software (version 26, USA).To determine the normality of data distribution, Kolmogorov-Smirnov test was carried out.For normally distributed data, continuousand categorical variables were described as mean±standard deviation (SD) and number and percentage (%), respectively,while for non-normally distributed data, the median and interquartile range (IQR, P25-P75) were used.Pairedt-test orχ2test was chosen to assess between-group differences in normal distribution variables, and Mann-WhitneyUtest for non-normal distribution ones.Kruskal-Wallis and one-way ΑNOVΑ were used to evaluate the differences between the two IOL groups.APvalue <0.05 was considered significant.

Table 1 Preoperative patient characteristics mean±SD
RESULTS
Preoperative Demographic CharacteristicsAt the beginning,54 patients 108 eyes with cataract who underwent uneventful FLACS combined with bilateral implantation of the tri839 or TFNT were recorded.After 3mo’ follow-up, only 28 patients’clinical records were available.Hence, data from 56 eyes of 28 patients were collected for analysis: 26 eyes of 13 patients in the tri839 group and 30 eyes of 15 patients in the TFNT group.The patients’ preoperative demographic characteristics are described in Table 1.The mean age was 59.3±11.8y and 61.5%(n=8) of patients were males in tri839 group, while the mean age was 56.2±8.3y and 73.3% (n=11) were males in TFNT00 group.The dysfunctional lens index (DLI), preoperative UDVΑ and expected SE did not differ statistically significantly between groups preoperatively.However, most patients were myopic with longer mean AL 27.32±3.05 mm in tri839 group than 25.85±2.54 mm in TFNT group (P=0.055).Accordingly,the IOL power implanted in both groups had a significant difference which was 10.40±7.40 D in tri839 group and 14.65±6.60 D in TFNT group respectively (P=0.027).

Figure 1 The preoperative and postoperative visual acuity of two groups in 3mo A: Visual acuity at 5 m (logMAR); B: Postoperative visual acuity at 30 cm (logMAR); C: Postoperative visual acuity at 40 cm (logMAR); D: Postoperative visual acuity at 60 cm (logMAR); E: Postoperative visual acuity at 80 cm (logMAR).
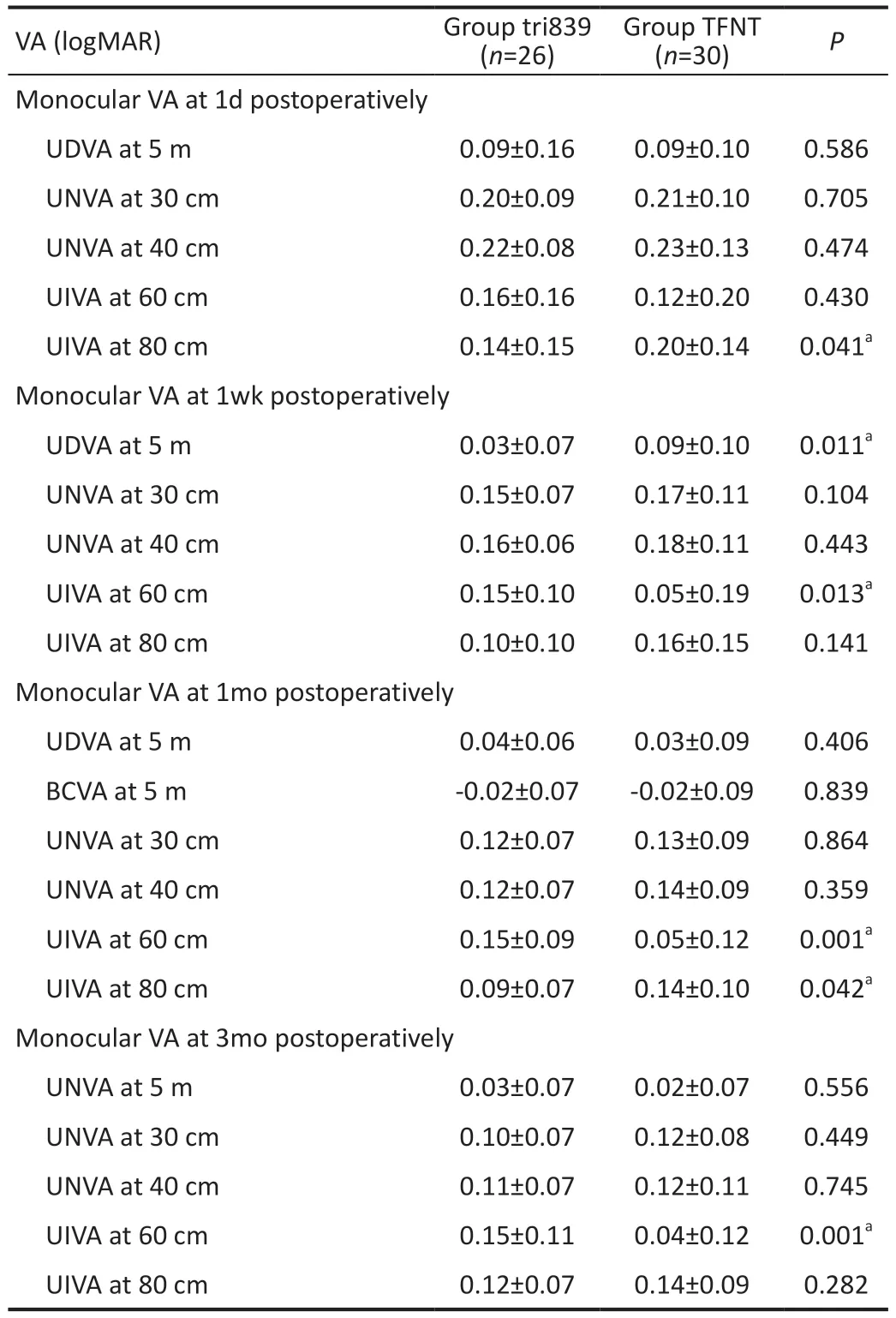
Table 2 The postoperative visual acuities of two groups

Table 3 The postoperative refractive stability of two groups
Visual AcuityPostoperative visual acuities are described in Table 2, both groups had achieved satisfactory natural whole-course visual acuities.UDVA was not significantly different between groups except at 1wk postoperative visit,which was due to the cornea edema in 2 eyes in TFNT group(Figure 1A).Best-corrected distance visual acuity (BCVA) in both group was similarly good at 1mo follow-up (-0.02±0.09vs-0.02±0.07 logMAR,P=0.839).TFNT group showed statistically significant better UNIΑ at 60 cm than tri839 group at the 1wk (0.05±0.19vs0.15±0.10 logMAR,P=0.013),1mo (0.05±0.12vs0.15±0.09 logMAR,P=0.001) and 3mo (0.04±0.12vs0.15±0.11 logMAR,P=0.001) followup, while tri839 group showed statistically significant better UNIA at 80 cm than TFNT group at the 1d (0.14±0.15vs0.20±0.14 logMAR,P=0.041) and 1mo (0.09±0.07vs0.14±0.10 logMAR,P=0.042) follow-up (Figure 1D, 1E).Furthermore, UNVA outcomes both at 30 cm and 40 cm were seemly better in the TFNT group than in the tir839 group at very visit, but with non-significantly difference (allP>0.05;Figure 1B, 1C).
Postoperative Refractive StabilityThe SEs had a great significantly difference between the two groups at very followup (Table 3).However, postoperative refractive status in both groups were described and showed a stable status at every visit(Figures 2 and 3).
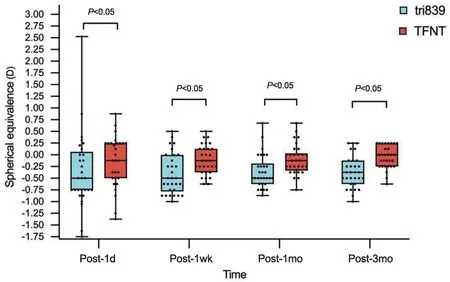
Figure 2 Distribution of postoperative spherical equivalence.
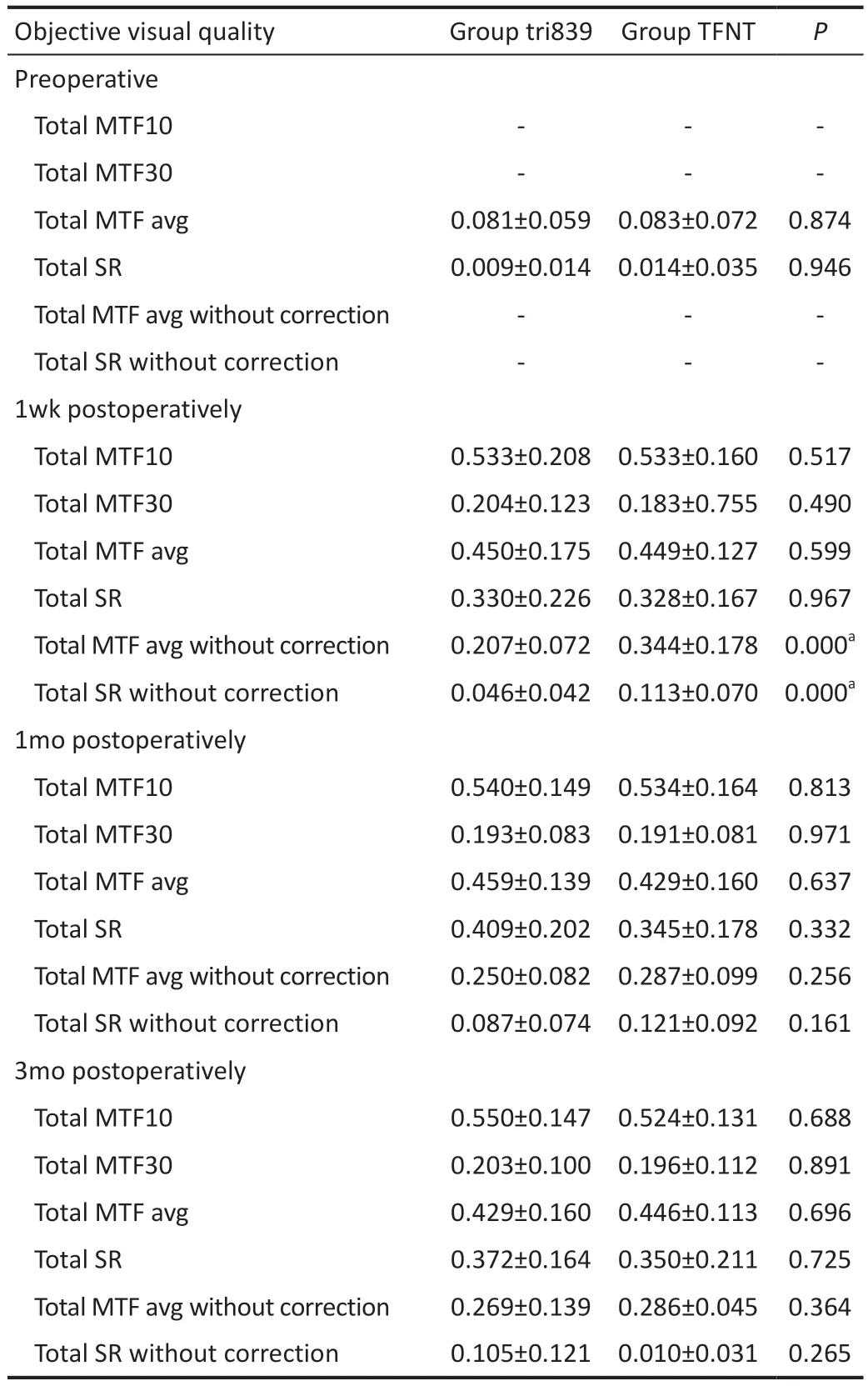
Table 4 The objective visual quality with iTrace analyzer of two groups mean±SD
Objective Visual QualityCompared with the preoperative total MTF and SR of the two groups, both postoperative values were significantly increased (P<0.05; Table 4, Figure 4A).However, during the 3mo follow-up, similar results and tendency were observed between groups, no matter with correction in sphere and cylinder or not (Figure 4B).Notably,when the sphere and cylinder were corrected, the total corrective average height of MTF and SR in tri839 group were better than those in TFNT group.
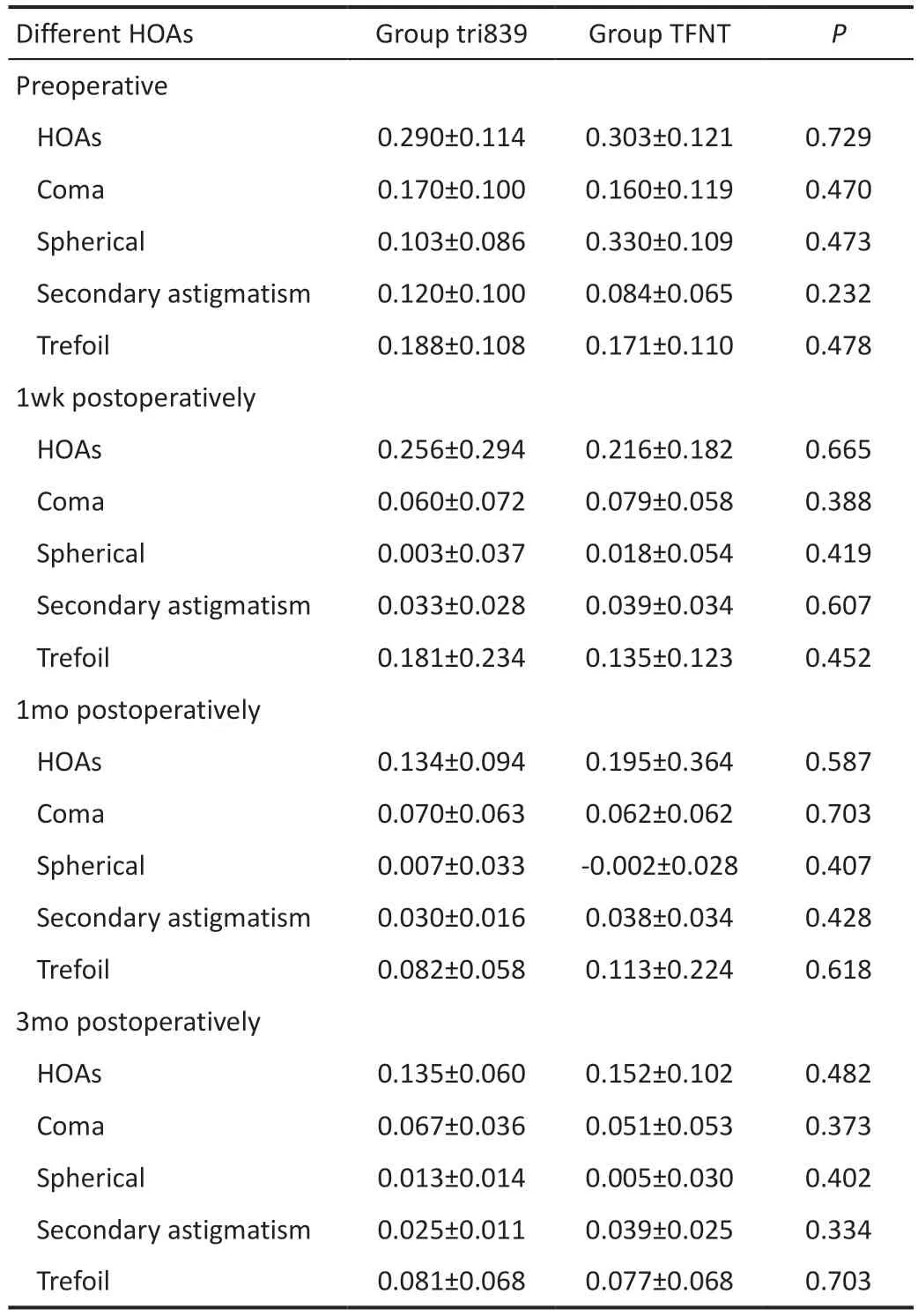
Table 5 The HOAs with iTrace analyzer of two groups mean±SD
High-Order AberrationsCompared with the preoperative total HOAs, coma, spherical, secondary astigmatism and trefoil of the two groups, both postoperative values were decreased,but without significant difference (P>0.05).And postoperative total HOAs, coma, spherical, secondary astigmatism and trefoil between two groups also showed no statistically significant difference at every visit time (P>0.05; Table 5, Figure 5).
Postoperative ComplicationsThe IOLs were successfully centered at every visit, and there were no serious postoperative complications during the 3mo period.However, there were 2 eyes in TFNT group with central cornea edema at 1d and 1wk visit due to the hard nucleus cataract and 1 eye in tri839 group with some signs of capsular opacification at 3mo visit which caused a little diminution of vision but did not yet need YAG laser posterior capsulotomy.
DISCUSSION
With the advances of IOL and development of surgical approaches, FLACS combined with trifocal IOLs implantation have been reported to make patients achieve clear, comfortable and lasting visual quality and optimal satisfaction[19-21].Hence, the refractive cataract surgery has become a new trend, and the aim of this type of surgery is to restore and reconstruct binocular tertiary visual function with the guidance of binocular vision theory.However, there are few reports about the comparison of binocular visual performance(subjective and objective) after FLACS combined with bilateral implantation of trifocal IOLs.Therefore, our study was designed to compare the subjective and objective clinical visual outcomes of bilateral implantations with the tri839 or TFNT during FLACS.

Figure 3 Postoperative refractive stability distribution of two groups A: Accumulated postoperative refractive error at 1mo; B: Accumulated postoperative refractive error at 3mo.

Figure 4 Preoperative and postoperative visual quality of two groups A: Corrective visual quality; B: Uncorrected visual quality.MTF:Modulated transfer function; SR: Strehl ratio.
Our study showed that postoperative visual acuities at all three distances were improved significantly compared with that preoperatively in both groups, which was similar to the previous studies with both identical trifocal IOLs[13,16,22-24], and confirmed that two trifocal IOLs could provide satisfactory results in whole-course visual acuities.Similarly, our data described both lenses (tri839 and TFNT00) provided excellent distance visual acuity (≤0.1 logMΑR; 100% and 93.33%) and better intermediate visual performance at 60 cm in group TFNT(86.67%) and 80 cm in group tri839 (76.92%), respectively.Between-group comparison also found that TFNT group showed statistically significant better UNIA at 60 cm than tri839 group at the 1wk, 1, and 3mo follow-up while tri839 group showed statistically significant better UNIA at 80 cm than TFNT group at 1d and 1wk follow-up.This is due to the design of the TNFT00 IOLs with middle focus at 60 cm originally and the comfortable intermediate distance work for Chinese were at 60-70 cm[25].Moreover, these results also indicate the importance of determining which intermediate distances are best for patients with different IOLs.UNVA outcomes both at 30 and 40 cm were seemly better in the tir839 group than TFNT group at very follow-up, but with non-significantly difference.Additionally, we noticed that the UNVA both at 30 and 40 cm in the two groups seemed not so good as the UIVA and UDVA.Several factors may contribute to these phenomena, such as the optical design of IOLs, limited patient sample, age, AL, examination protocol, environment and so on.In our study, since most patients were myopic with longer mean AL 27.32±3.05 mm in tri839 group than 25.85±2.54 mm in TFNT group (P=0.055), the target diopter was set between 0 and -1.0 D to account for the farsighted drift in the long axis eyes, and the SEs were -0.46±0.26 D in the tri839 group and-0.05±0.24 D in the TFNT group at 3mo follow-up, which also had a great significantly difference between the two groups at very follow-up.Liuet al[26]have found the similar results, in which they concluded that near vision would decrease in the extremely myopic eyes especially at lower luminance due to the IOLs distance-dominant design.
Refractive stability is an important indicative index for the visual performance and quality of life after cataract surgery[27-29].Since the patients in our study were mostly high myopic especially in tri839 group, the target refraction was set between 0 and -1.0 D due to the tendency of hyperopic drift in long axis eyes, so our results showed the postoperative SE in group 839 were a little myopic, but SEs were in a very stable status at very visit in both groups (Figures 2 and 3).These results corroborate the findings of a great deal of the previous work.According to McNamaraet al[27], visual and ocular parameters remained stable for two weeks after surgery.Khanet al[28]reported that refractive errors for most patients could be successfully measured and corrected one week after surgery, but need up to 4wk to stabilize due to the changes of central corneal thickness, effective lens position and so on;Charlesworthet al[29]found that the postoperative spherical and cylindrical degrees at 1 and 4wk had no statistical difference.In our study at 3mo visit, 30.8% and 90.0% of the eyes had SE within ±0.25 D, 69.3% and 96.7% had SE within ±0.50 D,92.4% and 100% had SE within ±0.75 D in tri839 group and TFNT group respectively, and both 100.00% had SE within±1.00 D, and the results were similarly at 1mo visit (Figure 3), which implies the stability of the refractive status.Good refractive stability indicates that the cornea and other tissues were not damaged during the surgery, hence the corneal thickness, effective lens position were in a stable status.This result may be explained by the usage of femotosecond laser during the surgery procedure, which has an accuracy and advantages in small tissue damage[30].
Objective visual quality can be evaluated by the MTF curves and SRs[31-32].The MTF curves reflect the different spatial frequencies in clear imaging degrees.In general, low spatial frequencies indicate the ability to see contours of objects,whereas high spatial frequencies indicate the ability to discern fine details.Shenet al[32]used the MTF values under a spatial frequency of 10 (MTF10) and 30 (MTF30) to evaluate far and near visual acuities in their study respectively.In this study,we not only used total MTF10 and MTF30 but also added the average height of total MTF (MTFavg) values to evaluate visual quality, and the average height less than 0.3 was implied not good visual acuity.An SR is obtained by taking the ratio of the peak intensity of an aberrated PSF to the diffraction-limited ideal PSF, and a value of 1.0 indicates the perfect optical quality[33].SR reflects the level of image quality and has the highest correlations with the visual performance[34-35].Besides,in our study, we also added the total MTF average height and SR without any correction in sphere and cylinder, which reflected the real and natural visual quality status.
Table 4 and Figure 4A showed that both postoperative total MTF and SR values at very visit time in two groups were significantly increased compared with the preoperative values, which indicated visual qualities in both group were greatly improved after surgery.These findings were similar to previously described data on MTF and SR[23,32,36].However,similar results and tendency were observed between groups at very visit time, no matter with correction in sphere and cylinder or not, which implied that the stability of the visual quality.What is noteworthy is that when the sphere and cylinder were corrected, the total corrective MTFavg and SR in tri839 group were better than those in TFNT group, while when the sphere and cylinder were not corrected, the total uncorrected MTFavg and SR in tri839 group were worse than those in TFNT group.These changes were due to the longer AL and myopic shift in tri839 group, when the postoperative SEs were corrected, the visual quality could be improved.We also found the consistent existing research which showed that MTFcutoff and SR decreased with increasing AL, especially when ΑL≥28 mm because there was more intraocular light scattering when the AL increasing[26].
HOAs can cause blurred vision, glare, decreased night vision and so on even in patients with excellent postoperative vision[37-38].Therefore, measuring the total HOAs postoperatively is useful to indicate the objective visual quality changes.Our findings showed the postoperative total HOAs were not high, which implied the patients were able to achieve satisfactory visual results.And the total HOAs, coma, spherical, secondary astigmatism and trefoil at very visit time were statistically lower than those before surgery, in accordance with the results of Zein El-Deinet al[36].It is well known that total HOAs were comprised with cornea HOA and internal HOA.Therefore,one possible explanation for these results was the application of FLACS.Xuet al[39]reported that FLACS presented a significantly lower total HOAs and spherical aberration,because femtosecond laser was able to accurately control the size and shape of the capsulotomy and deliver a more centered IOL, resulting in lower internal HOAs and higher visual quality in comparison with conventional phacoemulsification.Similarly, Miháltzet al[40]also concluded that laser-assisted capsulotomy produced significantly fewer internal aberrations than conventional capsulotomy, which may be able to achieve a better optical quality.
The novelty of our study lies in two places: the first one is the comparison of both subjective and objective visual performance for bilateral implantation of two trifocal IOLs,which is focus on the binocular vision theory and aims to restore binocular tertiary visual function; the second one is the analysis of visual performance with visual acuity, refractive stability and MTF, SR, HOAs with iTrace analyzerafter trifocal IOLs implantation using by femtosecond laser-assisted cataract procedures.
However, a number of limitations need to be noted in this study.First, it is a small sample size and short follow-up period study, which is inadequate to allow the generalizability of the results, hence a large-scale multicenter study and a longer follow-up period needs to be explored in future.Second, due to the lack of standardized reading charts, reading parameters were not tested.Finally, since the patient-related visual functioning questionnaires were mostly self-made and not standardized, visual disturbances and photic phenomena were difficult to determine.
In conclusion, FLACS with bilateral implantations of both tri839 and TFNT00 can achieve satisfactory natural wholecourse vision, high postoperative refractive stability and good visual quality but without significantly difference.iTrace aberration instrument can accurately evaluate the visual quality under different status.
ACKNOWLEDGEMENTS
Foundations:Supported by Medical Science and Technology Research Foundation Project of Guangdong Province (No.C2021087); The Scientific Research Foundation Project of Guangzhou Aier Eye Hospital, Jinan University (No.GA2023004).
Conflicts of Interest:Ju RH,None;Qu HK,None;Wu ZM,None;Chen Y,None;Wu LN,None;Long Y,None;Wang Z,None.
猜你喜欢
祖国(2019年1期)2019-02-22
经济技术协作信息(2018年30期)2018-11-22
消费导刊(2018年10期)2018-08-20
辽宁经济(2017年3期)2017-05-04
吉林农业·下半月(2016年6期)2016-10-21
戏剧之家(2016年17期)2016-10-17
河北金融年鉴(2016年0期)2016-03-15
名人传记·财富人物(2015年6期)2015-10-29
名人传记·财富人物(2015年6期)2015-10-29
体育世界(学术版)(2015年9期)2015-07-01
 International Journal of Ophthalmology2023年11期
International Journal of Ophthalmology2023年11期
- International Journal of Ophthalmology的其它文章
- Quantitative analysis of optic disc changes in school-age children with ametropia based on artificial intelligence
- Association analysis of Bcll with benign lymphoepithelial lesions of the lacrimal gland and glucocorticoids resistance
- In vitro protective effect of recombinant prominin-1 combined with microRNA-29b on N-methyl-D-aspartateinduced excitotoxicity in retinal ganglion cells
- Bioinformatics and in vitro study reveal the roles of microRNA-346 in high glucose-induced human retinal pigment epithelial cell damage
- Therapeutic effect of folic acid combined with decitabine on diabetic mice
- Comparison of three fundus inspection methods during phacoemulsification in diabetic white cataract