
Association analysis of Bcll with benign lymphoepithelial lesions of the lacrimal gland and glucocorticoids resistance
2023-11-10 04:05XuJuanZhangPengXiangZhaoMingShenMaHaoWuRuiLiuHuiWangMengYuLiuFeiXieXueMeiMa
Xu-Juan Zhang, Peng-Xiang Zhao, Ming-Shen Ma, Hao Wu, Rui Liu, Hui Wang,4,Meng-Yu Liu, Fei Xie, Xue-Mei Ma
1Faculty of Environment and Life, Beijing University of Technology, Beijing 100124, China
2Beijing International Science and Technology Cooperation Base of Antivirus Drug, Beijing 100124, China
3Beijing Tongren Hospital, Capital Medical University, Beijing 100730, China
4State Key Laboratory of Military Stomatology & National Clinical Research Center for Oral Diseases & Shaanxi International Joint Research Center for Oral Diseases,Department of General Dentistry and Emergency, School of Stomatology, Air Force Medical University; Xi’an 710032,Shaanxi Province, China
Abstract
● KEYWORDS: lacrimal gland benign lymphoepithelial lesion; BclI; single nucleotide polymorphisms; glucocorticoids resistance; fibrosis
INTRODUCTION
Benign lymphoepithelial lesions (BLEL) are lymphoepithelial proliferative diseases characterized by symmetrical bilateral swelling of the lacrimal, parotid, and submandibular glands.Once considered a subtype of primary Sjögren’s syndrome (pSS), BLEL is now classified as an IgG4-related disease[1], with elevated serum IgG4 levels and CD21+ B lymphocytes in the lacrimal, submandibular, and salivary glands, and CD4+, CD8+ T lymphocyte infiltration and fibrosis of the involved tissues.In contrast to pSS, BLEL is characterized by nonperiductal lymphocytic infiltration with hyperplastic multiple germinal center formation and mild destruction of the acini[2].Different organs are involved,which can also lead to different organ dysfunctions and clinical manifestations.When lacrimal glands are involved, the condition is known as BLEL of the lacrimal gland (LGBLEL).LGBLEL is an inflammatory lesion that occurs primarily in middle-aged women, and its main clinical manifestations include swelling of the eyelid and painless diffuse enlargement of the lacrimal gland.Although LGBLEL is regarded as a benign lesion, it is prone to recurrence, and malignant transformation to lymphoma occurs in 10.4%–14.3% of patients, which may endanger the life of the patients[3].While the specific pathogenesis of LGBLEL is still unclear,some studies have shown that it may be related to estrogen deficiency[4-5], elevated IgG4 level[6-7], autoimmunity and other factors[8], B cell receptor signaling pathway[9], T cell receptor signaling pathway[10], complement signaling pathway[11],and FcεRI signaling pathways[12].To date, glucocorticoids(GCs) are the key component of most treatment regimens for LGBLEL.GCs have a good curative effect in the short term[13];however, there is a risk of recurrence or aggravation after drug withdrawal, and many patients exhibit GCs resistance or GCs insensitivity.While total excision combined with postoperative steroid administration is selected for patients with severe clinical manifestations or poor response to GCs[14],this may lead to dry eye after lacrimal gland removal, which may require additional interventions such as scleral contact lenses to relieve dry eyes[15].Therefore, a more personalized diagnosis and treatment plan should be formulated in line with the individual’s responsiveness to GCs.
GCs are a class of steroid hormones secreted by the zona fasciculata of the adrenal cortex.The main GC hormone is cortisol, which binds to the glucocorticoid receptor (GR)encoded by the geneNR3C1.The GR complex undergoes nuclear translocation and binds to a specific DNA sequence on the target gene, thereby regulating gene transcription and participating in the regulation of the body’s development,metabolism, inflammation, and stress response[16].GCs are widely used clinically and play an important role in the treatment of nephrotic syndrome[17], bronchial asthma[18],rheumatic diseases[19], and other diseases.Dexamethasone,prednisone, and hydrocortisone are often used as anti-allergy,anti-inflammatory, anti-shock medications, and stimulants of bone marrow hematopoiesis; however, they are often accompanied by withdrawal reactions, such as disease recurrence and even degeneration of the adrenal cortex function[20].Moreover, any changes in GR, such asGRgene mutation or GR deficiency caused by disease, may lead to insensitivity to GCs, that is, poor or no reaction to GCs, which is also known as glucocorticoid resistance syndrome[21].
Various abnormalities in NR3C1 may be related to the occurrence and development of diseases.For example, it has been found that the gene polymorphism, methylation, and expression levels of NR3C1 are closely related to depression and other psychiatric diseases[22].Many studies[23-25]have shown that the single nucleotide polymorphisms (SNPs)of NR3C1 can affect the body’s responsiveness to GCs.Specifically, BclI (rs41423247), ER22/23EK (rs6189/rs6190),and N363S (rs6195) are the most extensively studied SNPs that are associated with alterations in GCs sensitivity or cortisol levels[26-28].
In LGBLEL, the association of BclI, ER22/23EK, and N363S polymorphisms with disease occurrence and resistance to GCs has not been studied.Therefore, in this study, we analyzed genotypes of these three SNPs loci in 56 LGBLEL patients.Data from healthy subjects and Han Chinese in Beijing(CHB)/Southern Han in Chinese (CHS) populations from the 1000 Genomes Project database were used for comparison to evaluate the three SNPs correlation with the development of LGBLEL.Moreover, we examined the clinical efficacy of GCs by meta-analysis to determine the evidence for the association between SNPs and GCs resistance to provide a reference for the clinical diagnosis and treatment of LGBLEL patients.
MATERIALS AND METHODS
Ethical ApprovalThis study has been approved by the Local Ethics Committee of Beijing Tongren Hospital, Capital Medical University (China, protocol code TRECKY203-KS-05).A signed consent was obtained from each patient prior to blood and tissues collection.
Participants and SampleTotally56 patients who were diagnosed with LGBLEL at the Capital Medical University Beijing Tongren Hospital, 11 males and 41 females, 25-73 years old.Ten healthy individuals contained 5 males and 5 females were recruited as a control group (normal), 30-58 years old, were included.The disease course of the patients(from the first discovery of eyelid enlargement to surgery) was counted and selected the patients who had been confirmed to have used GCs and received surgery because of poor or ineffective GCs were divided into GCs dependent group(n=22) and GCs resistant group (n=14)[29-32].The remaining patients who were confirmed not to have used GCs were in the no GCs group (n=16).
Peripheral blood serum from healthy individuals and LGBLEL patients were collected and peripheral blood DNA was extracted for subsequent testing.Pathological tissue samples and blood serum from patients with LGBLEL were collected immediately after surgery.A portion of the collected tissues was stored in liquid nitrogen until subsequent assays; the rest of the collected tissues were fixed in formalin, embedded in paraffin, cut into 5 μm sections for downstream histological analysis.
DNA Extraction and GenotypingPolymerase chain reaction(PCR) was used to amplify three SNP loci (BclI, ER22/23EKand N363S) in NR3C1 from peripheral blood DNA samples isolated with RelaxGene Blood DNA System (Tiangen, China).The primers and product sizes are shown in Table 1, PCR Premix Taq used TaKaRa TaqPCRTM Version 2.0 plus dye (RR901Q),the conditions are 94℃ denaturation for 5min, followed by 42 cycles of 94℃ 30s, 60℃ 30s, 72°C 30s, and finally 4℃incubation after 72℃ 5min; PCR products were analyzed by 2% agarose gel electrophoresis and then sequenced by Sangon Biotech (Shanghai, China), the genotypes of SNP was analyzed according to the sequential peak.

Table 1 Sequences of primers for single-nucleotide polymorphism in the NR3C1 gene
The CHB and CHS population data in the 1000 Genomes Project were used to analyze the gene variation coefficient of the study group compared with the normal population.
Meta-AnalysisIn accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA)guidelines, we conducted a systematic review of human studies investigating the relationship between the NR3C1 BclI polymorphism and GCs sensitivity and the review was registered in the international prospective register of systematic reviews (PROSPERO, ID: CRD42022349262).
Articles published before October 10, 2021 were searched in PubMed, Web of Science, Wanfang and CNKI databases.The search language of PubMed, Web of science and Wanfang is((glucocorticoid responsive) OR (glucocorticoid sensitive))OR (glucocorticoid resistant)) AND ((BclI) OR (rs41423247)),CNKI search language is: ((glucocorticoid responsive) +(glucocorticoid sensitive) + (glucocorticoid resistant)) * ((BclI)+ (rs41423247)).
The eligibility criteria for articles were as follows: should include a study of the relationship between the NR3C1 BclI polymorphism and GCs sensitivity, and should provide the genotype or allele frequency of BclI in the GCs-sensitive and resistant groups.If the article is reviews or uses animals as experimental subjects, they will not be included.Of note, consistent with PRISMA guidelines, records screened includes screening of both titles and abstracts.Two authors(Zhang XJ and Ma XM) will assess the quality of the studies independently without blinding to authorship or journal.Discrepancies will be resolved by discussion in conjunction with a third author (Zhao PX).The reference lists of the retrieved studies were manually scanned to identify additional relevant studies.Data extraction from each manuscript was performed in consistence with the eligibility criteria,and the extracted data was recorded in a spreadsheet.The following were recorded from each article: first author, year of publication, population of the research, outcomes, sample size (good response to glucocorticoid/poor response to glucocorticoid), and the genotype and allele counts for good/poor.We will use the Newcastle–Ottawa scale (NOS; http://www.ohri.ca/) of the case–control study to assess the quality of our included studies.The scoring items included the selection,comparability and exposure.Studies that received a score of 6 or higher were considered as high quality.
The Hardy-Weinberg equilibrium of genotypes in each group was evaluated by the Chi-square (χ2) test.P<0.05 was considered to be statistically significant.The heterogeneity was tested byχ2-basedQstatistic, andP<0.05 indicated that heterogeneity existed among the eligible studies.Dominant genetic model and allelic model were used to analysis the relationship between the NR3C1 BclI polymorphism and GCs sensitivity.Odds ratio (OR) with corresponded 95%confidence intervals (CI) in a fixed effect model using Mantel-Haenszel (M-H) method will be used.If there’s heterogeneity,random effect model will be conducted.Sensitivity analysis was performed by excluding individual studies from the pooled ORs and recalculating the statistical significance to explicate the stability of findings and to ascertain whether final pooled effect sizes were affected by a single publication.Review Manager Version 5.2 software (Denmark) was used to perform the Meta-analysis.
Funnel plots were planned to assess effects.If asymmetry in the funnel plot was detected, we planned to review the characteristics of the studies to assess whether the asymmetry was likely due to publication bias or other factors such as methodological or clinical heterogeneity of the studies.
Masson StainingMasson staining was used to evaluate fibrosis in LGBLEL tissues.The hearts were fixed with neutral formalin, sectioned, dehydrated, prepared in paraffin sections,and stained using a Masson staining kit (Solarbio, Beijing,China).The Masson staining was performed according to the manufacturer’s protocol.Collagen fibers are green or blue, cytoplasm, muscle fibers, red blood cells are red,and the nucleus is blue.The quantitative statistical method of collagen area from Masson staining: Collagen area fraction (%)=(Masson staining collagen positive area/total area)×100%.
Statistical AnalysisAnalysis of data was performed using the software IBM SPSS Statistics ver.20, GraphPad Prism9 and Review Manager Version 5.2.t-test for parametric variables(data presented as mean±SD), Mann-WhitneyUtest for nonparametric variables (data presented as median and 5thto 95thpercentiles).The genotype and allele distributions of the study groups were determined by direct counts and expressed as frequencies with standard errors (SE), and their association with the disease was investigated using OR and 95%confidence intervals (95%CI).Genotype and allele frequencies were calculated using the Chi-square test.
RESULTS
Demographic CharacteristicsWe analyzed the age and gender distribution of LGBLEL patients.Consistent with most of the existing reports, the disease is more common in women aged 41–60y (Figure 1; Table 2).The sequential peaks of the three SNPs with different genotypes are shown in Figure 2,and the NR22/23EK and N363S mutants were not detected.
Association Between Genotype and DiseaseThe frequencies of each genotype in the LGBLEL, Normal, and CHB/CHS groups are shown in Tables 3 and 4.The genotype distribution of each NR3C1 SNP did not deviate from the Hardy-Weinberg equilibrium (data not shown).There were no statistically significant differences in allele frequencies of any of the analyzed SNPs (P>0.05) between the LGBLEL group and the Normal group or the 1000 Genomes Project database CHB/CHS group.No mutation was found in ER22/23EK or N363S in any of the three groups (Table 3).The results showed that ER22/23EK and N363S were not associated with the development of LGBLEL and GCs responsiveness.
The allele frequencies of BclI were not significantly differed among the groups (P>0.05; Table 4).The occurrence of BclI polymorphism in the LGBLEL group was not significantly different from that in the normal group or CHB/CHS group.As the minor allele C in the LGBLEL group had the lowest frequency (OR<1), it might be a protective factor that may reduce the incidence of LGBLEL to a certain extent, but this was not statistically significant.
The analysis of the relationship between BclI genotype and disease course revealed that the LGBLEL patients with GC genotype had a longer disease course, indicating slower disease progression, but this was not statistically significant (Figure 3Α).This result needs to be confirmed with a larger sample size.
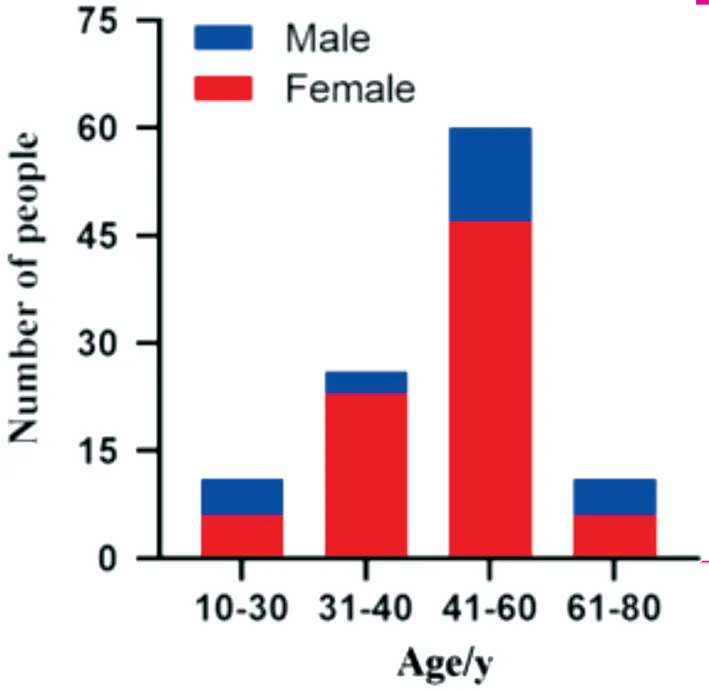
Figure 1 Age distribution of patients with LGBLEL LGBLEL: Lacrimal gland benign lymphoepithelial lesion.

Figure 2 Results of DNA sequencing with different SNPs A: DNA sequencing of the three genotypes of BclI; B: DNA sequencing of the wild-type genotype of ER22/23EK and N363S.
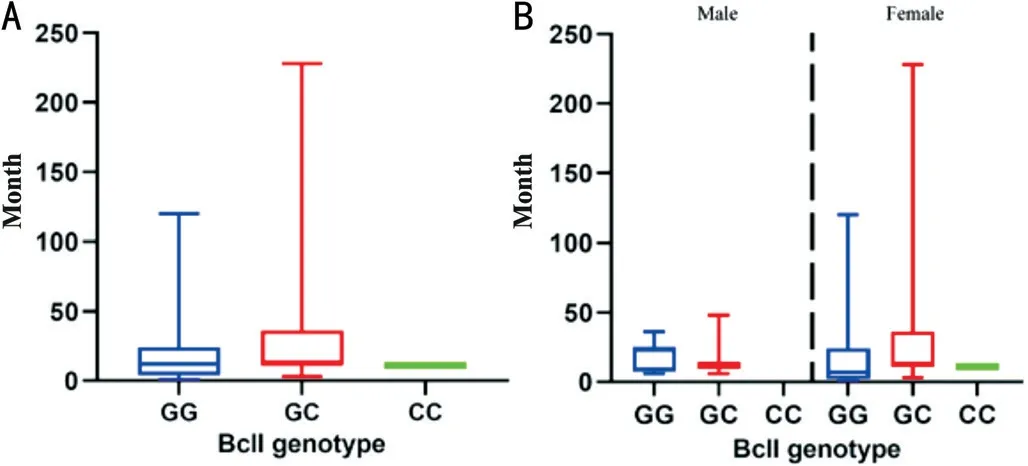
Figure 3 Disease course of LGBLEL patients A: Disease course in different genotypes of BclI; B: Disease course of BclI genotypes in different genders.LGBLEL: Lacrimal gland benign lymphoepithelial lesion.

Table 2 Demographic characteristics of the study population mean±SE
To verify whether gender contributed to the observed differences in the genotype frequencies, we divided the samples according to gender and compared them with the corresponding data of BclI from the 1000 Genomes Project (CHB/CHS; Table 5).There were 11 male patients in the LGBLEL sequencing sample,compared with 98 males in the CHB/CHS group.Althoughgender distribution was not significantly different between the groups (P>0.05), the frequency of the minor allele C was lower in the patients’ male group (P>0.05; OR=0.466; 95%CI,0.133–1.632), showing a stronger protective effect of C,which may be the reason for the lower incidence of LGBLEL in men.In contrast, the minor allele C frequency in females did not differ between the 41 patients and the 110 CHB/CHS individuals (P>0.05; OR=1.013; 95%CI, 0.567–1.807).These results suggest that the occurrence of LGBLEL in women is independent of BclI.However, the BclI genotype in female LGBLEL patients was associated with a longer disease course compared with that in male patients, especially in the GC genotype, although there was no significant difference(Figure 3B).The above results indicate that the high incidence of LGBLEL in women is not only related to the single factor of gender, but also the result of the joint influence of many factors including the SNP site BclI on the NR3C1 intron.Since the number of male samples was only 11, we still need to increase the number of male samples to reconfirm the correlation between the frequency of BclI minor allele C in males and the occurrence of the disease.

Table 3 Genotype frequencies of ER22/23EK and N363S in LGBLEL patients compared to healthy subjects (normal group) and subjects from the 1000 Genomes Project (CHB/CHS group)

Table 4 BclI genotype and minor allele C frequencies in LGBLEL patients and control population (normal group and CHB/CHS group)
Meta-Analysis of the Association between BclI and GCs SensitivityTo assess the relationship between BclI and hormone responsiveness, we performed a Meta-analysis of BclI and GCs sensitivity.Α total of 259 studies were identified through a literature search.We excluded 244 studies for specific reasons, which are described in Figure 4; finally, a total of 15 studies were included.All studies included in this systematic review had an overall good methodological quality with NOS scores ranging from 6 to 8.The characteristics of the studies included were summarizes in Table 6[31-45].Dominant genetic model (GC+CC in GCs-resistancevsGC+CC in GCs-sensitivity):

Figure 4 Literature screening process.

Table 5 BclI genotype and minor allele C frequencies in LGBLEL and control population males and females

Table 6 Characteristics of eligible studies on the association between the NR3C1 rs41423247 polymorphism and GCs sensitivity
For the 15 studies included, the heterogeneity test showed good homogeneity (I2=0;P=0.55), and the fixed-effects model was selected.The overall-effects test showed no significant differences in the CC genotype frequencies between the GCsresistance and the GCs-sensitivity groups (OR=1.05; 95%CI,0.86–1.27;P=0.63).To reduce racial differences, nine studies with non-Chinese subjects were excluded, and six studies were finally analyzed to evaluate the association between the NR3C1 BclI polymorphism and GCs response in Chinese subjects.The heterogeneity test showed good homogeneity(I2=37%;P=0.16), and the fixed-effects model was selected.The overall-effects test showed no significant differences in the CC genotype frequencies between the GCs-resistance and GCs-sensitivity groups in Chinese subjects (OR=0.96; 95%CI,0.71–1.41;P=1.30; Figure 5).The corresponding pooled ORs were not materially altered on removal of any individual study and there was no potential for publication bias.
Allelic model (C in GCs-sensitivityvsC in GCs-resistance):After one study was excluded for a lack of allelic frequencies,a total of 14 studies were included.For all the selected studies,the heterogeneity test showed significant heterogeneity(I2=52%;P=0.02), and the random-effects model was selected.The overall-effects test showed no significant differences in allele frequencies between the GCs-resistance and GCssensitivity groups (OR=1.02; 95%CI, 0.80–1.31;P=0.86).For further subgroup analyses on the studies with Chinese subjects only, the heterogeneity test showed significant heterogeneity(I2=59%;P=0.04), and the random-effects model was selected.The overall-effects test showed no significant differences in allele frequencies between the GCs-resistance and GCssensitivity groups in Chinese individuals (OR=0.96; 95%CI,0.58–1.60;P=0.88; Figure 6).Sensitivity analysis was used to eliminate heterogeneity.The removal of an individual study (Xueet al[42], 2015), the heterogeneity test showed good homogeneity (I2=37%;P=0.19), and the fixed-effects model was selected.The overall-effects test showed no significant differences in allele frequencies between the GCs-resistance and GCs-sensitivity groups in Chinese individuals (OR=1.07;95%CI, 0.74–1.55;P=0.73).
The Meta-analysis showed no significant differences between BclI and GCs sensitivity.
Association Between the BclI Genotype and GCs ResistanceIn our study, to investigate the relationship between BclI and GCs responsiveness in LGBLEL, according to the use and response to glucocorticoids, we divided patients into No GCs(n=16), GCs dependence (n=22), and GCs resistance (n=14)groups.The demographic characteristics are shown in Table 7.To further evaluate the relationship between BclI genotypes and GCs response, we counted the frequencies of each genotype and the minor allele C in the no GCs, GCs dependence,and GCs resistance groups (Table 8).The frequency of the minor allele C was significantly different between the GCsresistance patients and the no GCs patients.The allele C was more frequently observed in the GCs resistance group[OR (95%CI)=4.529 (1.243–16.510);P=0.017], and the GC genotype was more frequently observed in the GCs resistance group [OR (95%CI)=14.625 (2.191–97.612);P=0.003].These results indicate that BclI minor allele C is indeed a predictor of GCs response in LGBLEL patients and that GC genotype is more common in the GCs resistance group.No statistically significant differences were found between the GCs dependence and the no GCs groups.
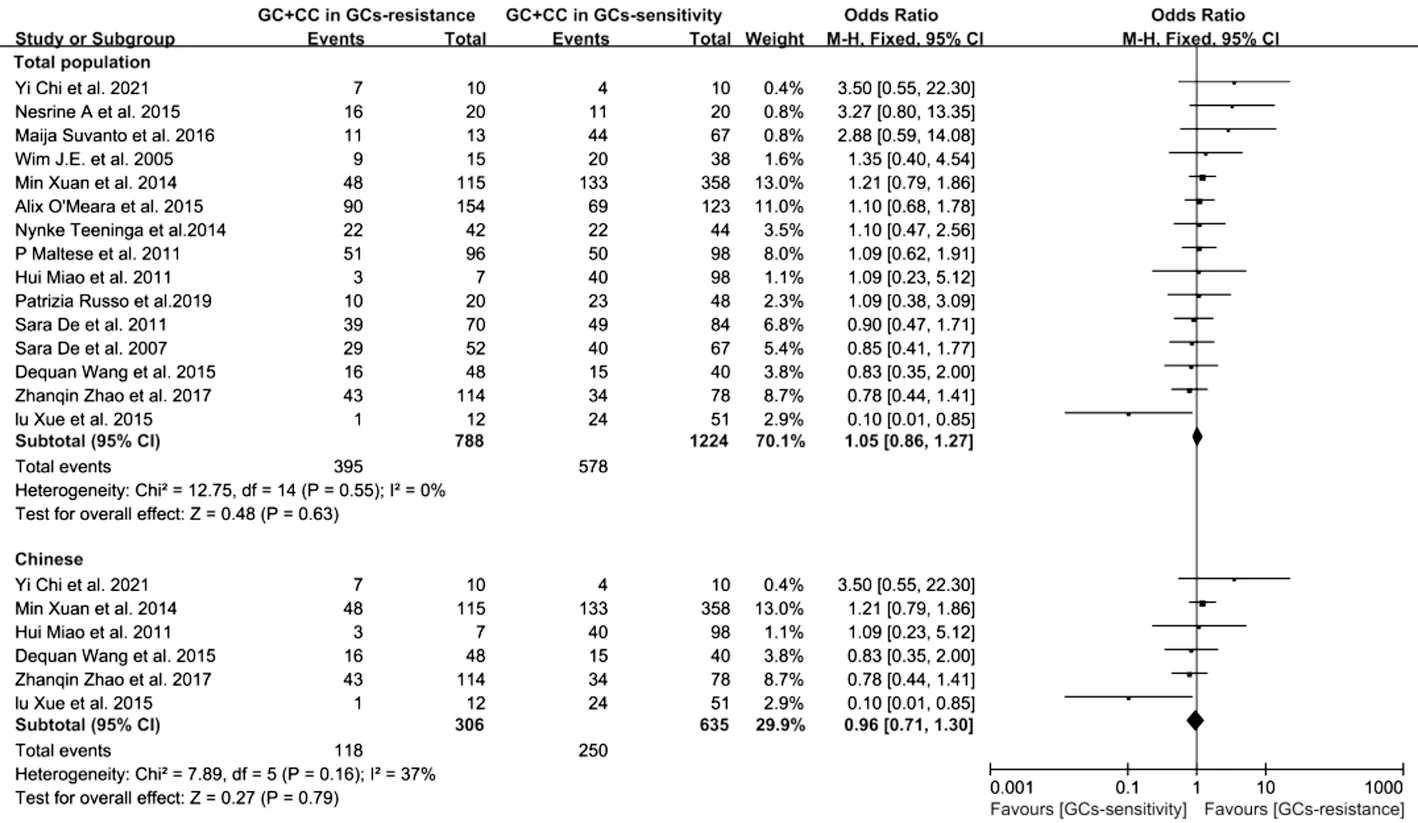
Figure 5 Forest plot of Meta-analysis for NR3C1 BclI genotype (GG+GC) and the GCs sensitivity GCs: Glucocorticoids; CI: Confidence interval;M-H: Mantel–Haenszel.

Figure 6 Forest plot of Meta-analysis for NR3C1 BclI minor allele C and GCs sensitivity GCs: Glucocorticoids; CI: Confidence interval; M-H:Mantel–Haenszel.

Table 8 BclI genotype and minor allele C frequencies in no GCs, GCs dependence, and GCs resistance groups of LGBLEL patients
Association analysis of the relationship between BclI genotypes and LGBLEL disease course in the no GCs, GCs dependence, and GCs resistance groups (Figure 7F) showed that patients with GC genotype in the GCs dependence group had a longer course of disease than GG patients in the GCs dependence group (the GCs dependence group without CC genotype patients).There were no statistically significant differences in the course of disease among patients with different genotypes in the three groups.
To explore the possible effect of BclI genotype on LGBLEL,we observed the pathological characteristics of samples with different genotypes in two of the groups by H&E and Masson staining (Figure 7; GCs dependence group did not have the CC genotype samples).The atrophy of lacrimal glandular parenchyma was observed in all the samples (green arrows in Figure 7B); among them, we observed massive hyperplastic lacrimal glands in GC samples from all groups, especially in the resistance group.There was more infiltration of lymphocytes(black arrows in Figure 7B) and fibrotic areas (red arrows in Figure 7B) in each sample, especially in the GG and CC genotype samples.The results of Masson staining analysis(Figures 7D–7E) further verified that the collagen fiber content of the GC genotype was lower than that of other genotypes in the same group; namely, the collagen fiber content of the GC genotype in the GCs dependence group was significantly lower than that of the GG genotype (P<0.001).The same trend also existed in the GCs resistance group, and the difference was significant (P<0.05).Indeed, the collagen fiber content of the GG genotype in the resistance group was the highest among the three groups, and was significantly higher than that in the no GCs group; for the GC genotype, the collagen content in the GCs dependence group was the lowest, significantly lower than that in the no GCs group (P<0.05), and extremely significantly lower than that in the GCs resistancegroup(P<0.001); and for GG genotype, the collagen content in the GCs resistance group was significantly higher than that in the no GCs group (P<0.001).
DISCUSSION
LGBLEL is an IgG4-related autoimmune disorder with unknown pathogenesis, for which therapeutic management is centered around the use of immunosuppressive agents(e.g., GCs) to inhibit inflammatory cytokines[46].The firstline treatment regimens consist of high-dose systemic GCs.However, patients’ insensitivity to GCs limits this treatment.TheNR3C1gene polymorphism of GR has been reported in many studies as one of the important reasons for GCs resistance, and it is even related to the occurrence of many diseases.However, there have been no reports of a correlation between NR3C1 SNPs and pathogenesis or GCs effectiveness in LGBLEL.
In the present study, we detected the association between three extensively researched SNPs of theNR3C1gene and pathogenesis or GCs effectiveness in LGBLEL.No differences regarding the allele frequencies and genotypes of these SNP sites were found between the LGBLEL patients and healthy subjects.Two SNP sites (NR22/23EK and N363S) did not show any mutations in our subjects.Therefore, these two SNPs are not associated with the pathogenesis and GCs effectiveness in LGBLEL, while the BclI GC may be associated with the development of LGBLEL and a decreased response to GCs.In particular, the heterozygous genotype GC of BclI slowed disease progression and fibrosis, especially in the GCs dependence group, and the minimal allele C may be related to a decreased GCs sensitivity.
Previous studies have shown that N363S polymorphism can increase and ER22/23EK can reduce the sensitivity to GCs[47], but there is no clear agreement on the effects of BclI in different diseases.In autoimmune disorders, BclI may be a protective factor for the development of systemic autoimmune disease in the Caucasian population, and it has also been shown to increase the sensitivity to GCs[48-50]; however, in studies of juvenile idiopathic arthritis, BclI is associated with longer arthritis duration, lower age at onset of arthritis, and higher levels of inflammation[51].In contrast, BclI is associated with reduced sensitivity to GCs in asthma.Namely, Corvolet al[52]found that patients with pulmonary fibrosis carrying the BclI gene, especially homozygous mutations, had a more significant decrease in forced expiratory volume in 1s (FEV 1) and forced vital capacity (FVC), indicating that BclI may be associated with the regulation of the inflammatory response in fibrotic lung tissue, thereby further interfering with the anti-inflammatory effect of GCs.Furthermore, BclI is not only related to the GCs resistance[53]but also the pathogenesis of bronchial asthma[54].A Meta-analysis of depression and BclI polymorphisms showed that the frequency of homozygous mutant CC genotypes in the depression group of the Caucasian population was significantly higher than that in the control group[55].A large number of studies have shown the dysregulated HPA axis negative feedback and elevated cortisol concentration due to the changed GR sensitivity[56-59], resulting in a partial or complete inability of GCs, indicating the relationship between altered GCs sensitivity mediated by BclI of GR gene and changes in metabolic parameters.In conclusion, BclI has different effects on different diseases and populations.
Similar to the results of the Meta-analysis in this study, the results of De Iudicibuset al[31], O’Mearaet al[37], and Xueet al[42]showed that the minor allele C could increase the body’s glucocorticoid sensitivity; however, Mohamedet al[41]and Kumstaet al[60]found the opposite correlation, and the results of other studies showed no significant correlation.The genotype frequencies of the population from different regions were different.The articles selected for our Metaanalysis included various diseases such as rheumatoid arthritis,depression, and colitis, and the regions from which the subjects were recruited in each study were different.Given that the number of selected papers was too small to be classified and analyzed according to the region and diseases, the differences in the final results may be masked.In the future, with the increase in the number of studies, it may be possible to analyze the correlation between NR3C1 polymorphisms of GR and the occurrence and development of diseases and GCs sensitivity according to factors such as diseases and populations, to more accurately evaluate the function of these polymorphisms.
Several recent studies have found that chronic exposure to high levels of GCs may exacerbate inflammation and lead to increased adipose tissue fibrosis[61], which may be due to high levels of GCs affecting the complex interactions of intercellular communication such as macrophages and adipocytes[62].
In the present study, H&E and Masson staining showed that the BclI GG genotype was associated with more lymphocyte infiltration, which may be closely related to the occurrence of chronic inflammation in LGBLEL, and the degree of fibrosis was higher than that of the other two genotypes.Massive lacrimal gland dysplasia was found, especially in the hormoneresistant group, whereas in the two CC genotype samples,denser lymphocytic infiltration was seen, also representing higher levels of inflammation.Because LGBLEL often presents with persistent inflammation and fibrosis of some glandular tissues, continuous treatment with high concentrations of GCs may exacerbate the degree of inflammation and fibrosis and accelerate the progression of the disease in patients with poor hormone response.
In summary, the present study offers evidence of an association between NR3C1 SNPs (BclI, ER22/23EK, N363S) and GCs effectiveness in LGBLEL patients.Moreover, BclI appears to be involved in regulating the development of LGBLEL,especially in tissue fibrosis.Due to the limitations such as the small sample size and SNP selection, these results only provide preliminary conclusions.Therefore, larger studies with a pharmacogenomics approach are necessary to establish definitive conclusions regarding the relevance of these SNPs.
ACKNOWLEDGEMENTS
We thank LetPub (www.letpub.com) for its linguistic assistance during the preparation of this manuscript.
Foundations:Supported by Natural Science Foundation of Beijing (No.7222025); Beijing Hospitals Authority’ Ascent Plan (No.DFL20190201); Natural Science Foundation of Beijing Projects (No.81602408).
Conflicts of Interest: Zhang XJ,None;Zhao PX,None;Ma MS,None;Wu H,None;Liu R,None;Wang H,None;Liu MY,None;Xie F,None;Ma XM,None.
 International Journal of Ophthalmology2023年11期
International Journal of Ophthalmology2023年11期
- International Journal of Ophthalmology的其它文章
- Quantitative analysis of optic disc changes in school-age children with ametropia based on artificial intelligence
- In vitro protective effect of recombinant prominin-1 combined with microRNA-29b on N-methyl-D-aspartateinduced excitotoxicity in retinal ganglion cells
- Bioinformatics and in vitro study reveal the roles of microRNA-346 in high glucose-induced human retinal pigment epithelial cell damage
- Therapeutic effect of folic acid combined with decitabine on diabetic mice
- Comparison of visual performance with iTrace analyzer following femtosecond laser-assisted cataract surgery with bilateral implantation of two different trifocal intraocular lenses
- Comparison of three fundus inspection methods during phacoemulsification in diabetic white cataract