灯盏花素对脓毒症急性肺损伤患者炎性因子、凝血功能的影响及疗效研究
2023-11-08 12:24周莹王雅宁吴爽柯慧娟孙鹏飞
天津医药 2023年4期
周莹 王雅宁 吴爽 柯慧娟 孙鹏飞
摘要:目的 探討灯盏花素对脓毒症急性肺损伤(ALI)患者炎性因子、凝血功能的影响及临床疗效。方法 84例脓毒症致ALI患者按随机数字表法分为对照组、灯盏花素低剂量组(灯低组)和灯盏花素高剂量组(灯高组),每组28例。对照组采用西医常规治疗,灯低组在对照组治疗基础上加用灯盏花素注射液(20 mg,1次/d),灯高组在对照组治疗基础上加用灯盏花素注射液(40 mg,1次/d),3组均治疗2周。评价3组患者临床疗效,比较3组治疗前及治疗2周后中医症候积分、氧合指数(PaO2/FiO2)、白细胞介素(IL)-6及肿瘤坏死因子-α(TNF-α)水平,测定凝血酶原时间(PT)、活化部分凝血活酶时间(APTT)及血小板计数,记录3组治疗期间药物相关不良事件。结果 灯低组和灯高组临床疗效和总有效率均优于对照组(P<0.05);3组治疗后中医症候积分及IL-6、TNF-α水平均较治疗前下降,且对照组、灯低组及灯高组依次降低(P<0.05);3组治疗后PT、APTT均较治疗前延长,且对照组、灯低组及灯高组依次延长(P<0.05);3组治疗后PaO2/FiO2、血小板计数均较治疗前增加,且对照组、灯低组及灯高组依次增加(P<0.05)。治疗中3组均未出现严重药物不良事件。结论 灯盏花素可明显改善脓毒症时凝血功能障碍,减少血小板不正常的消耗,抑制炎症反应,对脓毒症所致的ALI患者具有较为确切的临床疗效。
关键词:脓毒症;炎症;灯盏花素;急性肺损伤;凝血功能
中图分类号:R631文献标志码:ADOI:10.11958/20221250
Effects and clinical efficacy of breviscapine on inflammatory factors and coagulation function in patients with septic acute lung injury
ZHOU Ying, WANG Yaning, WU Shuang, KE Huijuan, SUN Pengfei
Department of Intensive Care Unit, the First Affiliated Hospital of Hebei North University, Zhangjiakou 075000, China
Abstract: Objective To explore effects and clinical efficacy of breviscapine on inflammatory factors and coagulation function in patients with septic acute lung injury (ALI). Methods A total 84 patients with ALI caused by sepsis were assigned to the control group, the low-dose breviscapine group (low-dose group) and the high-dose breviscapine group (high-dose group) according to random digital table, with 28 cases in each group. The control group was treated with conventional Western medicine. The low-dose group was additionally given breviscapine injection (20 mg, one time/d) on the basis of the control group, and the high-dose group was additionally given breviscapine injection (40 mg, one time/d) on the basis of the control group. The three groups were treated for 2 weeks. The clinical efficacy were evaluated in the three groups. Traditional Chinese medicine (TCM) syndrome scores, oxygenation index (PaO2/FiO2), interleukin (IL) -6 and tumor necrosis factor-α (TNF-α) levels, prothrombin time (PT), activated partial thromboplastin time (APTT) and platelet count were compared before and after two weeks of treatment between the three groups. Drug-related adverse events during treatment were recorded in each group. Results The clinical efficacy and total effective rate were better in the low-dose group and the high-dose group compared with those of the control group (P<0.05). After treatment, the TCM syndrome score and levels of IL-6 and TNF-α were decreased than those before treatment in the three groups (P<0.05), and the control group, the low-dose group and the high-dose group were decreased successively. After treatment, PT and APTT were prolonged compared with those before treatment in the three groups, and the control group, the low-dose group and the high-dose group were prolonged successively (P<0.05). After treatment, PaO2/FiO2 and platelet count were increased compared with those before treatment in the three groups, and the control group, the low-dose group and the high-dose group were increased successively (P<0.05). There were no severe adverse drug events during the treatment in the three groups. Conclusion Breviscapine can significantly improve the coagulation dysfunction in sepsis, reduce the abnormal consumption of platelets, inhibit inflammatory response, and has a relatively definite clinical effect on patients with sepsis-induced acute lung injury.
Key words: sepsis; inflammation; breviscapine; acute lung injury; coagulation function
急性肺损伤(ALI)是脓毒症患者的重要死因,而在脓毒症中炎症反应与凝血功能失控是导致死亡的重要因素[1-2]。当前尚无针对ALI的特效药物,但近年关于中药用于脓毒症ALI防治的研究报道日益增多。脓毒症属中医学“外感热病”,其中“暴喘”、“脱证”即脓毒症引起的ALI,关键病机在“痰饮、血瘀、热毒、气虚”4个方面[3]。有学者认为,瘀血是脓毒症关键[4]。因肺气不利,气不行血可致气滞血瘀,痰瘀互结,故凉血活血化瘀对脓毒症有着良好的疗效[5]。灯盏花素是从传统草药灯盏细辛中提取的黄酮类苷类化合物,具有活血化瘀、通经活络、抑制炎症反应、抗凝、抗血小板聚集、改善微循环等作用[6]。近期一项Meta分析研究显示,灯盏花素可改善慢性阻塞性肺疾病患者血液高凝状态,降低全血、血浆黏度,改善呼吸功能[7]。然而,关于灯盏花素可否改善脓毒症诱导的ALI患者的肺功能尚不清楚。本研究在传统西医综合治疗基础上加用灯盏花素制剂,观察不同剂量的灯盏花素对脓毒症ALI患者凝血功能、炎症反应的影响及临床治疗效果,旨在为脓毒症ALI患者的治疗提供参考。
1 资料与方法
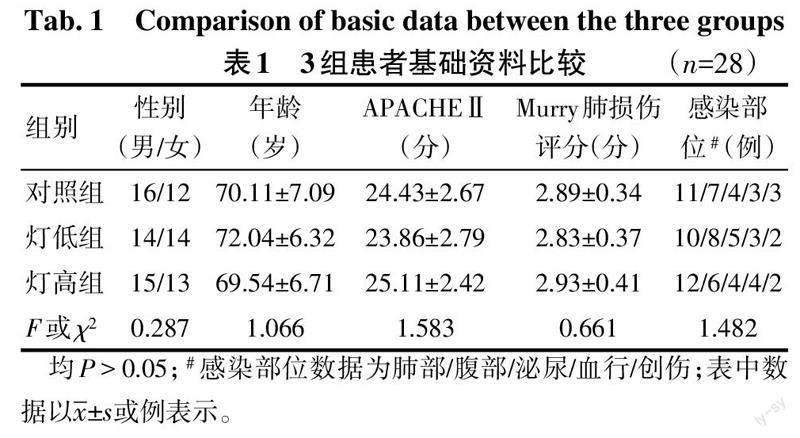
1.1 研究对象 选取2020年10月—2022年4月于河北北方学院附属第一医院重症监护病房收治的脓毒症合并ALI患者84例,采用随机数字表法将患者分为对照组、灯盏花素低剂量组(灯低组)和灯盏花素高剂量组(灯高组),每组28例。脓毒症诊断符合脓毒症3.0定义及诊断标准[8]。ALI参照柏林诊断标准[9]。中医诊断依据《中医病证诊断疗效标准》[10]:主要临床表现为气急、喘促、发昏、高热、便结、舌绛、脉滑数等。纳入标准:年龄55~81岁;拟行机械通气治疗。排除标准:合并肺纤维化、自身免疫性疾病、恶性肿瘤、胃肠道出血、严重肝肾功能异常者;有灯盏花素过敏史;有出血倾向、凝血功能紊乱或48 h内用过抗凝药物者;治疗期间自动出院或死亡的患者。3组性别、年龄、急性生理与慢性健康评分Ⅱ(APACHE Ⅱ)、Murry肺损伤评分及感染部位差异无统计学意义(P>0.05),具有可比性,见表1。本研究符合医学伦理学标准,并获得医院伦理委员审查批准(审批号:K2020099),患者或家属均签署知情同意书。
1.2 治疗方法 对照组在治疗原发病的同时,予以选择合适抗生素、液体复苏、肺保护性通气、应用血管活性药物等西医常规治疗,灯低组在对照组治疗基础上加用灯盏花素注射液(石药银湖制药有限公司,国药准字Z43020998)20 mg,灯高组在对照组治疗基础上加用灯盏花素注射液40 mg,均稀释到5%葡萄糖溶液里,1次/d静脉滴注,持续用药2周。
1.3 效果评价 (1)临床疗效:参照《临床疾病诊断依据治愈好转标准》[11]对3组患者的疗效进行评定,分为显效、有效和无效。总有效率(%)=(显效+有效)例数/总例数×100%。(2)中医症候积分:参照《中药新药临床研究指导原则》[12],于治疗前、治疗2周后对发热、喘息、胸闷、气促、黄痰、烦躁进行症状评分,根据症状无、轻、中、重,分别计0、1、2、3分,记录3组治疗前后中医证候积分。(3)氧合指数:分别于治疗前、治疗2周后采集动脉血3 mL,测定各组氧合指数(PaO2/FiO2)。(4)炎性因子:分别于治疗前、治疗2周后采集外周静脉血5 mL,分离血清,采用酶联免疫吸附试验(ELISA)测定血清白细胞介素(IL)-6、肿瘤坏死因子-α(TNF-α)水平,试剂盒购自北京贝尔生物工程股份有限公司。(5)凝血功能及血小板计数:分别于治疗前、治疗2周后采集外周静脉血5 mL,采用凝血分析仪测定凝血酶原时间(PT)、活化部分凝血活酶时间(APTT),采用血常规测定仪测定血小板计数。(6)不良反应:记录各组治疗过程中药物相关不良事件。
1.4 統计学方法 采用SPSS 19.0软件进行数据分析。符合正态分布的计量资料以x±s表示,组内治疗前后比较采用配对t检验,多组间比较采用单因素方差分析,组间多重比较用LSD-t法。计数资料以例或例(%)表示,组间比较采用χ2检验,等级资料采用Kruskal-Wallis H检验。P<0.05为差异有统计学意义。
2 结果
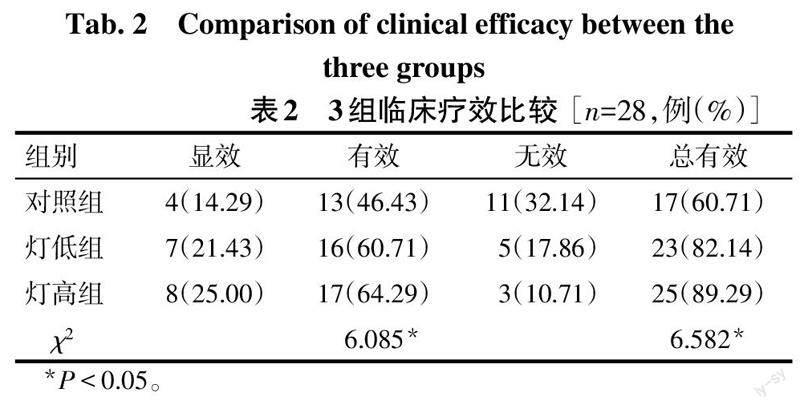
2.1 3组临床疗效比较 灯低组、灯高组临床疗效和总有效率均优于对照组(P<0.05),见表2。
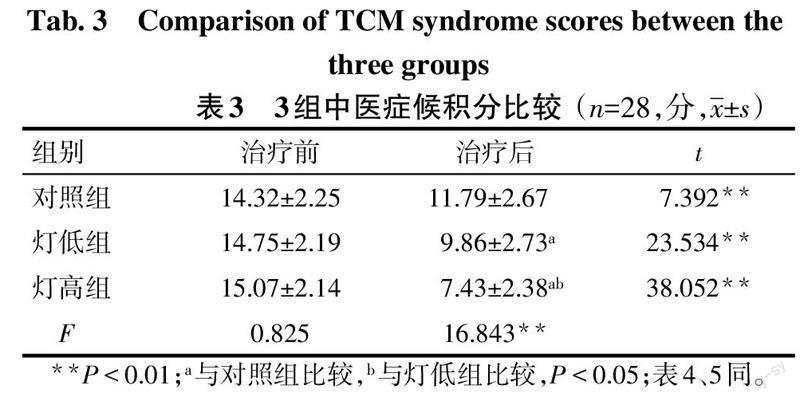
2.2 3组中医症候积分比较 治疗前3组中医症候积分差异无统计学意义,治疗后3组中医症候积分均较治疗前下降,且对照组、灯低组及灯高组中医症候积分依次降低(P<0.05),见表3。
2.3 3组治疗前后PaO2/FiO2比较 治疗前3组PaO2/FiO2差异无统计学意义,治疗后3组PaO2/FiO2均较治疗前升高,且对照组、灯低组及灯高组PaO2/FiO2依次升高(P<0.05),见表4。
2.4 3组治疗前后炎症水平比较 治疗前3组IL-6、TNF-α水平差异无统计学意义,治疗后3组IL-6、TNF-α水平均较治疗前下降,且对照组、灯低组及灯高组IL-6、TNF-α水平依次降低(P<0.05),见表5。
2.5 3组治疗前后凝血功能及血小板计数比较 治疗前3组PT、APTT及血小板计数水平差异无统计学意义,治疗后3组PT、APTT均较治疗前延长,且对照组、灯低组及灯高组依次延长(P<0.05);治疗后3组血小板计数均较治疗前增加,且对照组、灯低组及灯高组依次增加(P<0.05),见表6。
2.6 不良反应情况 灯高组治疗中出现1例皮疹和1例心悸,灯低组出现1例头晕,经对症处理后消失。对照组治疗过程中未见明显不良反应。
3 讨论
脓毒症ALI是一个多因素、多环节、多种机制共同参与的致病过程,炎症反应和凝血功能异常是其发病机制的关键环节[13]。脓毒症时炎性因子大量释放,凝血系统被激活,机体处于高凝状态,且凝血功能紊乱和炎性因子相互促进,互为因果,在体内形成恶性循环,最终可导致弥漫性血管内皮损伤及多脏器功能障碍,严重影响患者预后[14]。研究报道,抗凝药物可通过减少肺内凝血,改善脓毒症ALI时高凝状态,改善微循环,减轻炎症及肺水肿[15]。在脓毒症ALI治疗中注重调节炎症、凝血的平衡,对改善患者预后,增加患者生存率有着十分重要的意义[16]。近年来随着中医药的作用靶点不断深入研究,中药对脓毒症ALI防治的研究报道日益增多[17]。中医认为,活血化瘀应贯穿ALI的治疗始终[18];而灯盏花素不但具有活血化瘀、疏通脉络的功效,还具有抗凝、抗血小板聚集、抗炎性反应等多种药理学作用[6],有多途径、多靶点的作用机制,安全性高,不良反应少,故其符合中医对ALI的治疗理念。目前对中药的临床疗效评价与中医症候密不可分,中医症候积分是反应症候与辨证论治的评判方法[19]。本研究结果显示,灯低组和灯高组治疗后中医症候积分较对照组下降,PaO2/FiO2较对照组升高,临床疗效和总有效率优于对照组,且以灯高组改善更为著,表明灯盏花素对脓毒症ALI患者有较好的临床疗效,可以改善脓毒症患者肺部氧合状态,改善肺功能。
关于灯盏花素的使用剂量,文献报道较少,说明书推荐剂量为10~20 mg/d,但临床使用剂量往往比说明书推荐的剂量大。本试验选择灯盏花素说明书推荐剂量(20 mg)和临床常用剂量(40 mg)作为研究。PT和APTT分别是反映外源性和内源性凝血功能的指标,监测其改变可以尽早发现脓毒症时的凝血功能紊乱。本研究结果显示,治疗后3组患者PT、APTT均较治疗前延长,提示治疗后3组患者的凝血功能均改善。与对照组相比,灯低组、灯高组PT、APTT延长更明显,尤以灯高组为著,说明灯盏花素可以干预脓毒症时机体高凝状态,改善脓毒症ALI患者的凝血功能。
TNF-α和IL-6是机体重要的炎症介质,参与炎症级联反应及其他细胞因子的活化,可诱导细胞凋亡、损伤血管内皮,进而促进肺内微血栓形成,加重ALI[20]。脓毒症ALI时,血小板在促炎及血栓形成过程中会过度活化、消耗,引起血小板减少,进一步加重炎症损伤[21]。本研究结果显示,3组患者治疗后IL-6、TNF-α水平较治疗前均降低,血小板计数均升高,说明治疗后全身炎症反应有所降低,相比于对照组,灯低组、灯高组IL-6、TNF-α下降幅度大,血小板计数升高明显,且以灯高组改善更显著,说明灯盏花素尤其是高剂量能抑制炎性因子,减少血小板的活化、聚集、耗损,阻断炎症与凝血之间的级联反应。
综上所述,在脓毒症ALI早期给予灯盏花素辅助治疗,可有效提高患者氧合指数,抑制炎症反应,改善凝血功能,减少血小板非正常的消耗,對脓毒症ALI患者具有较为确切的临床疗效。
参考文献
[1] WANG X,XING Y,TANG Z,et al. Thioredoxin-2 impacts the inflammatory response via suppression of NF-κB and MAPK signaling in sepsis shock[J]. Biochem Biophys Res Commun,2020,524(4):876-882. doi:10.1016/j.bbrc.2020.01.169.
[2] 周醒,谢剑锋,杨毅. 脓毒症相关凝血功能障碍的机制及药物治疗进展[J]. 中华内科杂志,2022,61(2):224-228. ZHOU X,XIE J F,YANG Y. Mechanism and treatment progress for sepsis-induced coagulopathy[J]. Chinese Journal of Internal Medicine,2022,61(2):224-228. doi:10.3760/cma.j.cn112138-20210314-00212.
[3] 卢悦,张平平,王东强,等. 急性肺损伤中医病因病机的探讨[J]. 中国中医急症,2020,29(2):280-282. LU Y,ZHANG P P,WANG D Q,et al. Discussion on pathogenesis and pathogenesis of acute lung injury[J]. Journal of Emergency in Traditional Chinese Medicine,2020,29(2):280-282. doi:10.3969/j.issn.1004-745X.2020.02.025.
[4] 李若愚,肖超烈,沈其猷,等. 试论“瘀”在ARDS形成中的作用[J]. 光明中医,2016,31(15):2164-2165. LI R Y,XIAO C L,SHEN Q Y,et al. Discussion the function of “Blood Stasis” in the formation of ARDS[J]. Guangming Journal of Chinese Medicine,2016,31(15):2164-2165. doi:10.3969/j.issn.1003-8914.2016.15.010.
[5] 张海云,韩伟东,刘海梅,等. 丹参酮ⅡA对急性肺损伤小鼠炎症因子和氧化应激水平的影响[J]. 解剖学研究,2020,42(6):491-495. ZHANG H Y,HAN W D,LIU H M,et al. Effects of Tanshinone ⅡA on inflammatory factors and oxidative stress in mice with acute lung injury[J]. Study of anatomy,2020,42(6):491-495. doi:10.3969/j.issn.1671-0770.2020.06.002
[6] WU L H,LIU M,FANG Z Y. Combined therapy of hypertensive nephropathy with breviscapine injection and antihypertensive drugs:a systematic review and a meta-analysis[J]. Evid Based Complement Alternat Med,2018,2018:2958717. doi:10.1155/2018/2958717.
[7] 李慧,任小瑞,张育建,等. 活血化瘀中药注射剂治疗慢性阻塞性肺疾病急性加重期网状Meta分析[J]. 辽宁中医药大学学报,2022,24(2):120-127. LI H,REN X R,ZHANG Y J,et al. Network Meta-analysis of promoting blood circulation and removing blood stasis chinese medicine injections on acute exacerbation of chronic obstructive pulmonary disease[J]. Journal of Liaoning University of Traditional Chinese Medicine,2022,24(2):120-127. doi:10.13194/j.issn.1673-842x.2022.02.027.
[8] SINGER M,DEUTSCHMAN C S,SEYMOUR C W,et al. The third international consensus definitions for sepsis and septic shock sepsis-3[J]. JAMA,2016,315(8):801-810. doi:10.1001/jama.2016.0287.
[9] ARDS Definition Task Force,MARCO V R,GORDON D R,et al. Acute respiratory distress syndrome:the Berlin Definition[J]. JAMA,2012,307(23):2526-2533. doi:10.1001/jama.2012.5669.
[10] 國家中医药管理局医政局. 中医病证诊断疗效标准(2017版)[M]. 北京:中国中医药出版社,2017:3-4. National Administration of Traditional Chinese Medicine. Diagnostic efficacy criteria for Diseases and Syndromes of Traditional Chinese Medicine (2017 edition)[M]. Beijing:China Traditional Chinese Medicine Publishing House,2017:3-4.
[11] 孙传兴. 临床疾病诊断依据治愈好转标准[M]. 北京人民军医出版社,2002:126. SUN C X. Clinical disease diagnosis is based on cure and improvement criteria[M].Beijing:Beijing People's Military Medical Publishing House,2002:126.
[12] 黄蓓. 《证候类中药新药临床研究技术指导原则》发布[J]. 中医药管理杂志,2018,26(21):107. HUANG B. Technical guidelines for clinical research of new syndromic TCM drugs[J]. Journal of Traditional Chinese Medicine Management,2018,26(21):107. doi:10.16690/ j.cnki.1007-9203.2018.21.056.
[13] IBA T,LEVI M,LEVY J H. Sepsis-induced coagulopathy and disseminated intravascular coagulation[J]. Semin Thromb Hemost,2020,46(1):89-95. doi:10.1055/s-0039-1694995.
[14] 陈振华,江琴. 脓毒症患者凝血功能指标、降钙素原水平与临床预后的关系[J].检验医学,2020,35(10):1053-1055. CHEN Z H,JIANG Q. Relationship between coagulation function index,procalcitonin level and clinical prognosis in patients with sepsis[J]. Laboratory medicine,2020,35(10):1053-1055. doi:10.3969/j.issn.1673-8640.2020.10.021.
[15] 蒋湘粤,冯芮华,刘江萍,等. 低分子肝素对急性呼吸窘迫综合征患者临床疗效影响的Meta分析[J]. 中华危重病急救医学,2020,32(12):1472-1478. JIANH X Y,FENG R H,LIU J P,et al. Meta-analysis of the curative effect of low molecular weight heparin on acute respiratory distress syndrome[J]. Chinese Critical Care Medicine,2020,32(12):1472-1478. doi:10.3760/cma.j.cn121430-20201019-01426.
[16] 李桂云,冯永文,向兰,等. 不同预后脓毒症患者血清降钙素原、C反应蛋白与凝血功能指标和APACHEⅡ评分的关系分析[J]. 现代生物医学进展,2021,21(2):274-278. LI G Y,FENG Y W,XIANG L,et al. Analysis of the relationship between serum procalcitonin,c-reactive protein and coagulation function and APACHEⅡscore in sepsis patients with different prognosis[J]. Progress in Modern Biomedicine,2021,21(2):274-278. doi:10.13241/j.cnki.pmb.2021.02.016.
[17] 劉继法,胡渊龙,邱占军,等. 中药有效成分治疗脓毒症急性肺损伤作用机制研究进展[J]. 辽宁中医药大学学报,2021,23(1):171-176. LIU J F,HU Y L,QIU Z J,et al .Advances in the pathogenesis of active ingredients of traditional chinese medicine in the treatment of acute lung injury in sepsis[J]. Journal of Liaoning University of Traditional Chinese Medicine,2021,23(1):171-176. doi:10.13194/j.issn.1673-842x.2021.01.040.
[18] 余霞. 成人呼吸窘迫综合征病理分期的中医治疗思路[J]. 中医药学刊,2003,21(10):1760-1792. YU X. TCM treatment of adult respiratory distress syndrome by pathological stages[J]. Journal of Chinese Medicine,2003,21(10):1760-1792. doi:10.3969/j.issn.1673-7717.2003.10.094.
[19] 孙瑞华,李欢,徐凯,等. 中医证候临床评价的探讨[J]. 世界中医药,2017,12(6):1470-1474. SUN R H,LI H,XU K,et al. Clinical evaluation in Traditional Chinese Medicine (TCM)[J]. WORLD CHINESE MEDICINE,2017,12(6):1470-1474. doi:10.3969/j.issn. 1673-7202.2017.06.063.
[20] 韩宇,高传玉,秦秉,等. 抗凝治疗对脓毒症凝血和炎症指标的影响及其意义[J].中华危重病急救医学,2015,27(2):102-105. HAN Y,GAO C Y,QIN B,et al. The effect of anticoagulant therapy on coagulation and inflammation markers in sepsis patients and its significance[J]. Chinese Critical Care Medicine,2015,27(2):102-105. doi:10.3760/cma.j.issn.2095-4352.2015.02.005.
[21] WALBORN A,RONDINA M,MOSIER M,et al. Endothelial dysfunction is associated with mortality and severity of coagulopathy in patients with sepsis and disseminated intravascular coagulation[J]. Clin Appl Thromb Hemost,2019,25:1-9. doi:10.1177/1076029619852163.
(2022-08-15收稿 2022-10-22修回)
(本文编辑 陆荣展)
猜你喜欢
中华养生保健(2020年4期)2020-11-16
中国中医急症(2019年10期)2019-05-21
中外医疗(2016年33期)2017-03-02
中国实用医药(2016年30期)2016-12-28
上海医药(2016年23期)2016-12-22
中国现代医生(2016年23期)2016-11-15
现代仪器与医疗(2016年4期)2016-10-09
中国实用医药(2016年22期)2016-08-19
中华老年多器官疾病杂志(2016年9期)2016-04-28
中国实用医药(2016年5期)2016-02-20