
Management of urethral strictures and stenosis caused by the endo-urological treatment of benign prostatic hyperplasia—a single-center experience
2023-06-28 07:16:52RajivKore
Asian Journal of Urology 2023年2期
Rajiv N.Kore
Warana Institute of Urosurgery, Kolhapur, India
KEYWORDS Urethral stricture;Benign prostatic hyperplasia;Transurethral resection of prostate;Urethroplasty;Holmium laser enucleation of prostate;Trans-urethral bipolar electro-enucleation;Bladder neck stenosis
Abstract Objective: Urethral stricture disease after endo-urological treatment of benign prostatic hyperplasia (BPH) is a sparsely described complication.We describe management of five categories of these strictures in this retrospective observational case series.Methods: One hundred and twenty-one patients presenting with symptoms of bladder outflow obstruction after endo-urological intervention for BPH from February 2016 to March 2019 were evaluated.Among them,76 were eligible for this study and underwent reconstructive surgery.Preoperative and postoperative assessments were done with symptom scores, uroflowmetry,ultrasound for post-void residue, and urethrogram.Any intervention during follow-up was classed as a failure.The recurrence and 95% confidence interval for recurrence percentage were calculated.Results: The following five categories of patients were identified: Bulbo-membranous (33[43.4%]), navicular fossa (21 [27.6%]), penile/peno-bulbar (8 [10.5%]), bladder neck stenosis(6 [7.9%]), and multiple locations (8 [10.5%]).The average age was 69 years (range: 60—84 years).Overall average symptom score, flow rate, and post-void residue changed from 21 to 7,6 mL/s to 19 mL/s,and 210 mL to 20 mL,respectively.The average follow-up was 34 months(range: 12—58 months).Overall recurrence and complication rates were 10.5% and 9.2%,respectively.The recurrence in each category was seen in 3, 1, 2, 1, and 1 patient, respectively.Overall 95% confidence interval for recurrence percentage was 4.66—19.69.Conclusion: Urethral stricture disease is a major long-term complication of endo-urological treatment of BPH.The bulbo-membranous strictures need continence preserving approach.Navicular fossa strictures require minimally invasive and cosmetic consideration.Peno-bulbar strictures require judicious use of grafts and flaps.Bladder neck stenosis in this cohort could be treated with endoscopic measures.Multiple locations need treatment based on their sites in single-stage as far as possible.
1.Introduction
Benign prostatic hyperplasia (BPH) is a highly prevalent condition managed by urologists across the world.Medically refractory BPH is treated endo-surgically.Despite a host of competitive modalities, the trans-urethral resection of prostate (TURP) remains the so-called gold standard for more than nine decades.The other endo-urological interventions are bipolar TURP,holmium laser enucleation of prostate(HoLEP),photo-selective vaporization of prostate,trans-urethral microwave therapy, and trans-urethral bipolar electro-enucleation.These interventions can cause urethral stricture disease (USD), having a stricture rate of 1.7%—11.7% and bladder neck stenosis (BNS) rate of 0.4%—9.7% [1].The early post-surgical complications after prostate therapy such as hemorrhage, infection, and TUR syndrome are declining due to improved techniques.However, long-term complications such as USD are on the rise[1].The occurrence of a stricture defeats the purpose of surgical therapy of BPH.The extent and complexity may vary but the long-term consequences are overwhelming.Locations of these strictures are predominantly bulbomembranous segment and navicular fossa.Penile urethra and bladder neck get affected less frequently, albeit with severe effects.The treatment of USD could range from simple dilatation/urethrotomy to complex urethroplasty using graft or flap.This complication is sparsely discussed in the literature.Some reports have referred to the bulbomembranous stricture following TURP [2]; however,comprehensive approaches for this entity have not been adequately reported.We describe the management of five different categories of these strictures in this retrospective observational case series.
2.Patients and methods
The patients presenting with symptoms of bladder outflow obstruction after endo-urological intervention for BPH were evaluated.Apple Saraswati Multispecialty Hospital Institutional Ethical Committee approval was obtained for the conduct of this study (Project approval No.55).All the prostate cancer related complication cases or any patients with concomitant stricture at the time of BPH treatment were excluded.The study period was from February 2016 to March 2019.The common presenting features were bladder outflow obstruction, urinary tract infection, dysuria, and hematuria.
Overall, 121 patients were screened for this study.Out of these 19 patients had only urinary tract infection.Fifteen patients had detrusor hypo-function due to diabetes.Eleven patients were lost to follow up after the initial consultation.Seventy-six patients were eligible for this study.The intervention for BPH in these included TURP in 21 (28%), TURP with trans-urethral incision of prostate(TUIP) in 6 (8%), HoLEP in 8 (11%), and bipolar TURP in 41(54%).The clinical evaluations were done with symptom score, uroflowmetry, ultrasound for post-void residue,retrograde urethrogram, and micturating cysto-urethrogram.Urine culture was done to confirm urine sterility.
Reconstructive procedures and endoscopic treatment were done in these 76 patients.All the patients had urethrocystoscopy to confirm the diagnosis, either prior to reconstruction as a separate procedure or at the time of urethroplasty.
A silicon catheter was left in place in 70 patients of urethroplasty for 3—4 weeks and an irrigating catheter in six patients of bladder neck resection for 2—3 days.A check urethrogram was done in urethroplasty group to assess the repair.If a major leak was noted, the catheter was left in place for additional time for an overall maximum duration of 6 weeks.The patients were followed every 3 months initially and yearly after, with clinical evaluation, uroflowmetry and if required urethrogram.Any intervention needed was classed as a failure.The recurrence after urethroplasty and 95% confidence interval for recurrence percentage were calculated.
3.Results
The outcome analysis of the management of 76 patients of USD developed following endo-urological intervention for BPH was done.The average age was 69 years(range:60—84 years).The comorbidities were diabetes mellitus in 23 (30%), hypertension in 21 (28%), coronary artery disease in 8 (11%), cerebrovascular accidents in 3 (4%), and bronchial asthma in 4 (5%) patients.
Five different categories of patients could be identified(Table 1):

Table 1 Distribution of location, prior intervention, recurrence and 95% CI for recurrence percentage.
· Bulbo-membranous stricture;
· Navicular fossa stricture;
· Penile/peno-bulbar long segment stricture;
· BNS with or without prostatic urethral stenosis;
· Multiple locations.
3.1.Bulbo-membranous stricture
A ventral onlay buccal mucosal graft (BMG) urethroplasty described by Barbagli et al.[3] was done.A ventral urethrotomy was done, distal to the site of bulbomembranous stricture.The mucosa deep incision was extended towards and beyond the stricture without deepening into spongiosa till the verumontanum could be visualized.A hydrophilic guidewire helped maintain the line and length of this mucosal incision.A DeBakey forceps helped keep the stricture open.This step was for continence preservation.With the internal sphincter mechanism destroyed during resection, the patient was dependent solely on the external sphincter for continence.A tailored BMG was then parachuted to the proximal apex of this mucosal incision(Fig.1).Ventral onlay grafting was completed with spongioplasty.
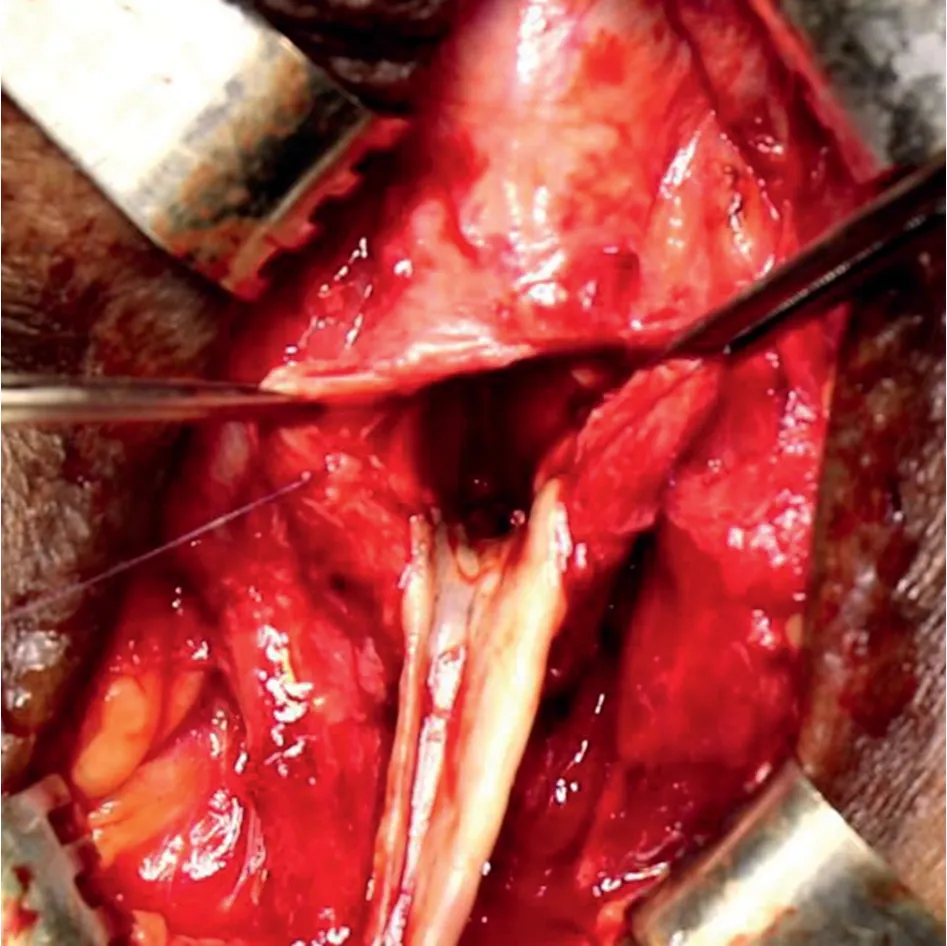
Figure 1 Ventral onlay for bulbo-membranous stricture showing graft parachuted to the apex.
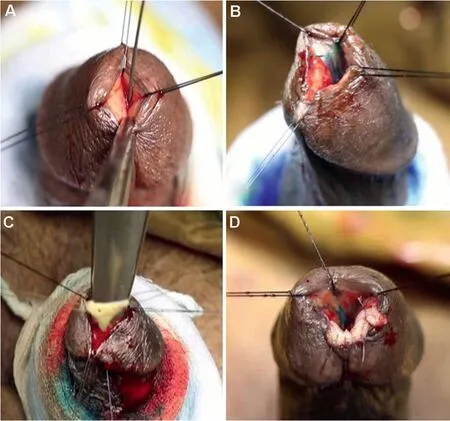
Figure 2 Trans-urethral ventral inlay for navicular stricture.(A)Initial appearance accommodating only a small guide wire;(B) Ventral excision of the stricture; (C) Triangular graft being parachuted; (D) Final appearance.
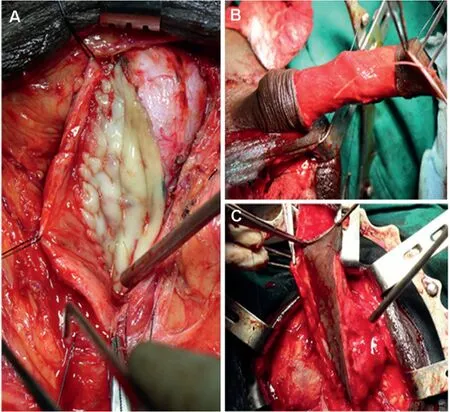
Figure 3 Graft and flapinlongsegmentpenile andpeno-bulbar stricture.(A) Dorsal onlay buccal mucosal graft; (B) McAninch flap:circular penile fasciocutaneous flap on dartos;(C)McAninch flap:flap rotated and sutured to the urethral plate.

Figure 4 Double face substitution in near-obliterated stricture.(A)Dorsal approach showing grafting on dorsal and ventral side,approached from dorsal route;(B—H)All ventral approach:(B)Ventral urethrotomy;(C)Narrow urethral plate of near obliterated stricture; (D) Dorsal incision; (E) Dorsal inlay substitution; (F) Widened urethral plate after the substitution; (G) Ventral onlay substitution; (H) Spongioplasty.

Figure 5 Bladder neck stenosis.

Figure 6 Multiple locations: Transurethral resection of bladder neck stenosis through dorsal urethrotomy in a case of peno-bulbar stricture.
Out of33patients treated withventral onlay,three showed obstructive symptoms during 6—15 months postoperatively.They were confirmed to have stricture recurrence at the proximal anastomotic site.They needed endoscopic dilatation.None of these patients were incontinent.
3.2.Navicular fossa stricture
In the majority of patients in this group,minimally invasive trans-meatal ventral inlay BMG urethroplasty was done.With three stay sutures, the penis was stabilized.After placing a guidewire, a ventral mucosal incision was done across the stricture with an ophthalmic knife, extending into the proximal healthy urethra.A DeBakey forceps was used to keep the lumen open.A triangular-shaped tailored BMG was then parachuted into the lumen with an apical stitch that was tied outside.Double passes were required through the spongiosa and apex of the graft.The rest of the graft was then spread fixed with quilting stitches (Fig.2).Fifteen patients out of 21 were treated with transurethral ventral inlay BMG urethroplasty.The remaining six patients had an advanced, nearly obliterative stricture.Two of these six patients underwent extended meatotomy described by Malone[4].Two had a trans-glanular approach where the entire scarred mucosa was excised and buccal mucosal substitution was done.One patient underwent Jordan flap [5].One patient with diabetes mellitus and significant spongiofibrosis of glans had a trans-glanular substitution of the entire diseased urethra and resurfacing of glans.He developed early recurrence at 3 months and was treated with dilatation.
3.3.Penile/peno-bulbar long segment stricture
In this unique subset of patients, the extent of urethral damage was much more.Based on the location, length,width of stricture, and availability of substitution, various procedures were done, using grafts or flaps (Fig.3).Dorsal onlay for segmental stricture or pan-urethroplasty for an entire extent of the urethra was done.Flaps such as McAninch and Orandi were constructed for a long segment stricture in patients with insufficient oral mucosa but healthy penile skin.In near-obliterated strictures, double face substitution using BMG was done either through a dorsal or ventral route (Fig.4).
McAninch flap was constructed in two patients while Orandi flap was done in one.Pan-urethroplasty was done in two patients while dorsal onlay BMG urethroplasty was done in one.Double-face BMG urethroplasty was done in two patients, one each with a dorsal and a ventral approach.Two of these eight patients had early recurrence at 6 months.One of these responded well to urethrotomy and the other to dilatation.
3.4.BNS
In this group of patients,the endoscopic correction was done in all patients.A transurethral incision was done through the fibrotic ring at the bladder neck(Fig.5).If the fibrous tissue was seen in abundance at the bladder neck or prostatic urethra, it was resected to achieve adequate lumen.
Out of six patients of BNS,four patients had only bladder neck occlusion.Two of these patients had entire prostatic occlusion.They were also treated by resection of fibrous tissue.One of these two pan-prostatic strictures recurred.This was treated with endoscopic resection.None of these patients hadde novoincontinence.None required either open, laparoscopic/robotic reconstructive procedures.
3.5.Multiple locations
Some patients had more than one location of stricture.They were reconstructed on their merit depending on the site and length of the stricture.In patients of the penobulbar stricture with BNS, the resection was done through the urethrotomy performed for dorsal onlay urethroplasty,and planned for the peno-bulbar stricture (Fig.6).
There were five patients with bulbo-membranous and navicular strictures, one with penile and navicular strictures,and two with peno-bulbar strictures with BNS.In this group, higher rate of postoperative complications such as wound infection and pyrexia was observed.
In summary,70 of 76 patients had 2 to 4 prior dilation or urethrotomy.Overall average symptom score, flow rate,and post-void residue changed from 21 (range: 15—27) to 7(range: 5—12 mL), 6 mL/s (range: 3—9 mL/s) to 19 mL/s(range: 14—33 mL/s), and 210 mL (range: 90—270 mL) to 20 mL(range 0—40 mL), respectively.Clavien-Dindo grades I, II, and IIIb complications such as pyrexia, wound infection,glans dehiscence,and fistulae were seen in 2(2.6%),3(3.9%), and 2 (2.6%) cases, respectively.The overall complication rate was 9.2%.The average follow-up was 34 months (range: 12—58 months).Table 1 shows the distribution of the number of patients at each location, the average number of interventions before treatment, recurrence after urethroplasty, and 95% confidence interval for recurrence percentage in each category.The overall recurrence rate after the treatment was 10.5%.The overall 95% confidence interval for this result was 4.66—19.69.
4.Discussion
USD following surgical management of BPH is a long-term complication.This complication defeats the purpose for which surgical therapy was instituted for BPH in the first place—bladder outflow obstruction.There are scanty references for this complication in the literature[2,3].
BPH is one of the most prevalent conditions in men above 60 years of age.It is primarily treated with pharmacotherapy.However, a significant number of pharmacotherapy resistant patients and/or those landing with BPH complications warrant surgical intervention.
Rassweiler et al.[6] have evaluated perioperative and long-term complications after TURP, and compared the percentage of occurrence of these complications in the recent periods versus past periods.They were transfusion rate (0.4%vs.7.1%), TUR syndrome (0.0%vs.1.1%), clot retention (2%vs.5%), and urinary tract infection (1.7%vs.8.2%) [6].However, the long-term complications like USD and BNS have not decreased, with the rates remaining at 2.2%—9.8% and 0.3%—9.2%, respectively [6].
Other modalities of BPH treatment are also not without complications of USD.Bipolar TURP—an increasingly popular modality to treat BPH—is blamed for a high rate(almost twice)of USD(8.3%)compared to monopolar(4.2%)[7,8].The possible reason could be the high cutting power of 270 W; however, a recent study by Falahatkar et al.[9]reported a converse finding.USD and BNS are common after HoLEP with an incidence of 1.4%—3.0% and 0.6%—5.4%,respectively [10].Photo-selective vaporization of prostate achieves better hemostasis in high-risk bleeding disorder cases but it has a stricture rate of 1.7%—5.2%and a BNS rate of 1.4%—3.6% [11].Trans-urethral microwave therapy can cause BNS and prostatic urethral stenosis in 10% of cases,due to thermal injury[12].Long-term data regarding transurethral bipolar electro-enucleation are still awaited.
Several factors either individually or collectively may lead to USD and/or BNS.They are, compression by either the large resectoscope sheath or large catheter leading to ischemia,perioperative infection,excessive resection,long resection duration, inadvertent stray current leak, urinary extravasations, and comorbid condition such as diabetes.These factors can be controlled.
Bulbo-membranous stricture is the commonest location[13], also seen in our study.It occurs because of the fixed position of the urethra and compression of the largecaliber size of the sheath.The great concern of this location is continence.The external urinary sphincter is omega-shaped.Barbagli et al.[3] demonstrated the technique to address these important issues while repairing these strictures [3].A judicious mucosa-deep ventral incision protects this only remaining mechanism of continence after TURP.The apical stitches and parachuting of the graft are the important key steps in this procedure as done in this group of our series.
Navicular stricture is the second most common location[13].The reason is the relatively narrow lumen compared to other parts.Compression due to oversize sheath leads to ischemic stricture.The initial treatment is dilatation urethrotomy.A simple meatotomy or extended meatotomy described by Malone [4] is sometimes sufficient.Tonkin and Jordan [14] have recommended that this so-called “reconstructive ladder”should not be followed.They described the popular Jordan flap repair (a transverse preputial flap on a dartos pedicle, rotated inside as ventral onlay followed by glansplasty) [5].Skin flaps were described as early as 1963[15].When the urethra is extensively fibrosed with an unsalvageable urethral bed, a staged procedure is a viable option.DePasquale et al.[16] described a trans-glanular approach of complete excision of the fibrosed urethra and primary grafting followed by tubularization in the second stage.This procedure can be done as a single-stage in selected cases with a healthy spongiosal bed.In recent years, a minimally invasive transurethral BMG urethroplasty has been described by Nikolavsky et al.[17].In our series,we performed this minimally invasive technique in less severe cases and other techniques in more advanced, obliterated, and longer strictures with optimal results.
Penile/peno-bulbar long segment stricture occurs,especially in inexperienced hands or in technical failure leading to current leak causing damage to a long segment of the penile urethra.Several techniques are described to repair these strictures [18—21].A dorsal onlay substitution urethroplasty either through a perineal or penile route is the most common approach [18].McAninch flap [19],Querty flap [20], and Orandi flap [21] have a specific place in the reconstruction of these strictures.They have a robust blood supply and can reach the required length of the stricture.Double face grafting, either through a dorsal or ventral approach is required in obliterated strictures[22,23].Others have used lingual mucosa as a new urethral plate and completion of reconstruction by a ventral onlay,with penile skin flap[24].In our study group a judicious use of these grafts and flaps resulted in successful outcomes.
BNS is termed as stenosis (not as stricture) due to absence of spongiosal tissue surrounding this part of the urethra.An extensive resection around the bladder neck may result in scarring due to excessive current causing damage to the prostatic urethra, especially in small prostate glands [25].The histopathological evidence of the prostate showing chronic prostatitis and a multifocal prostatic abscess has shown to be associated with BNS [26].Iatrogenic stenosis of the prostatic urethra has been classified according to location, into three categories: Type I,located exclusively at the bladder neck; Type II, located in the mid-portion of the prostatic fossa;and Type III,located in the entire prostatic fossa (replaced by fibrosis) [28].TUIP, first described by Orandi [27] is a deep incision at 5 o’clock and 7 o’clock position while resection involves a complete removal of fibrous element within the prostatic fossa.Though TUIP is commonly done, Pansadoro and Emiliozzi [28] showed that the effective measure for these strictures leading to BNS is endoscopic resection.The management of recurrent BNS is also resection.It achieves a success rate of 91%—98% [28].Kranz et al.[29] have shown that TUR for BNS is significantly more successful(p=0.031).Our success rate of 87% compares well these studies.Sometimes open, laparoscopic/robotic bladder neck reconstruction is required in intractable fibrosis [30].
Multiple locations, noted in some cases, are due to a combination of reasons.A systematic plan is required to repair these in one stage if possible as seen in our series.
Limitations of our study were, a retrospective study in a single center with its inherent limitation of number and a relatively short follow-up.A multi-institutional study with a larger cohort size is required to establish the long-term outcome.
5.Conclusion
USD is a major long-term complication of the endourological management of BPH.All the currently available modalities of trans-urethral treatment for BPH can cause USD.The bulbo-membranous and navicular fossa are the most common locations.Five categories are noted with specific treatment strategies.Though the initial management is conservative, several different reconstructive techniques are required, specific for the location of stricture.The bulbo-membranous strictures need a diligent continence preserving approach.Navicular fossa strictures should be dealt preferably with minimally invasive intent and cosmetic consideration.Peno-bulbar strictures require judicious use of grafts and flaps.BNS in this cohort could be treated with endoscopic measures.Multiple locations need treatment, based on their site, in one stage if possible.
Conflicts of interest
The author declares no conflict of interest.
 Asian Journal of Urology2023年2期
Asian Journal of Urology2023年2期
- Asian Journal of Urology的其它文章
- Radiofrequency ablation for renal tumours:A retrospective study from a tertiary centre
- The role of quick Sepsis-related Organ Failure Assessment score as simple scoring system to predict Fournier gangrene mortality and the correlation with Fournier’s Gangrene Severity Index: Analysis of 69 patients
- Role of circulating tumor cell clusters in patients with metastatic hormone-sensitive prostate cancer receiving a gonadotropin-releasing hormone antagonist: A pilot study
- Percutaneous embolization by direct puncture for the treatment of high-flow priapism
- Subadventitial resection of the ureter—new method for surgical corrections of the ureteropelvic junction and ureterovesical junction obstructions
- Tunica albuginea versus buccal mucosa graft urethroplasty for anterior urethral stricture:A prospective randomised pilot study