
Tricuspid valve avulsion
2023-05-23 04:26:44AbhinavKaranAnamarysBlancoEmilMissovSrinivasanSattiraju
Journal of Geriatric Cardiology 2023年4期
Abhinav Karan, Anamarys Blanco, Emil Missov, Srinivasan Sattiraju
1.Internal Medicine, University of Florida College of Medicine-Jacksonville, Florida, USA; 2.Department of Cardiology,University of Florida College of Medicine-Jacksonville, Florida, USA
✉ Correspondence to: abhinavkaran@hotmail.com https://doi.org/10.26599/1671-5411.2023.04.009
A 71-year-old male with a medical history of sick sinus syndrome with dual-chamber pacemaker system implantation six years prior,and hypertension presented to the emergency department with complaints of generalized malaise, fever, and severe lower back pain.His evaluation was significant for a 2.3 cm × 1.2 cm epidural abscess, alongside methicillin-resistant staphylococcal bacteremia.He was started on intravenous vancomycin.A transthoracic echocardiogram was performed with the discovery of a 1.2 cm long vegetation in the upper right atrium attached to the pacemaker lead, an ejection fraction of 50%-55%, and no gross valvular abnormalities.
Given his diagnosis of infective endocarditis, a pacemaker device and lead extraction were planned with transesophageal surveillance.He underwent successful right atrial lead extraction.Immediately following right ventricular lead extraction, a disruption in the anterior leaflet of the tricuspid valve was noted on echocardiographic monitoring, with attached, mobile, echogenic structures moving along the tricuspid annular plane (Figure 1A) with torrential tricuspid regurgitation (Figure 1B).These findings were most consistent with an acute traumatic tricuspid valve avulsion.The patient was subsequently immediately referred for urgent surgical tricuspid valve repair.
Right ventricular lead extraction results in tricuspid valve injury in less than 10% of all cases.[1]Tricuspid valve avulsion, however, is very rare, documented primarily in isolated case reports in medical literature.[2]The mechanism of the majority of these cases relates to mechanical disruption of the tricuspid valvular apparatus,such as malcoaptation, leaflet impingement, and damage to the chordae tendinae.We propose that echocardiographic surveillance during implantation and extraction of right ventricular leads is beneficial to idenity and reduce the likelihood of tricuspid valve disease.
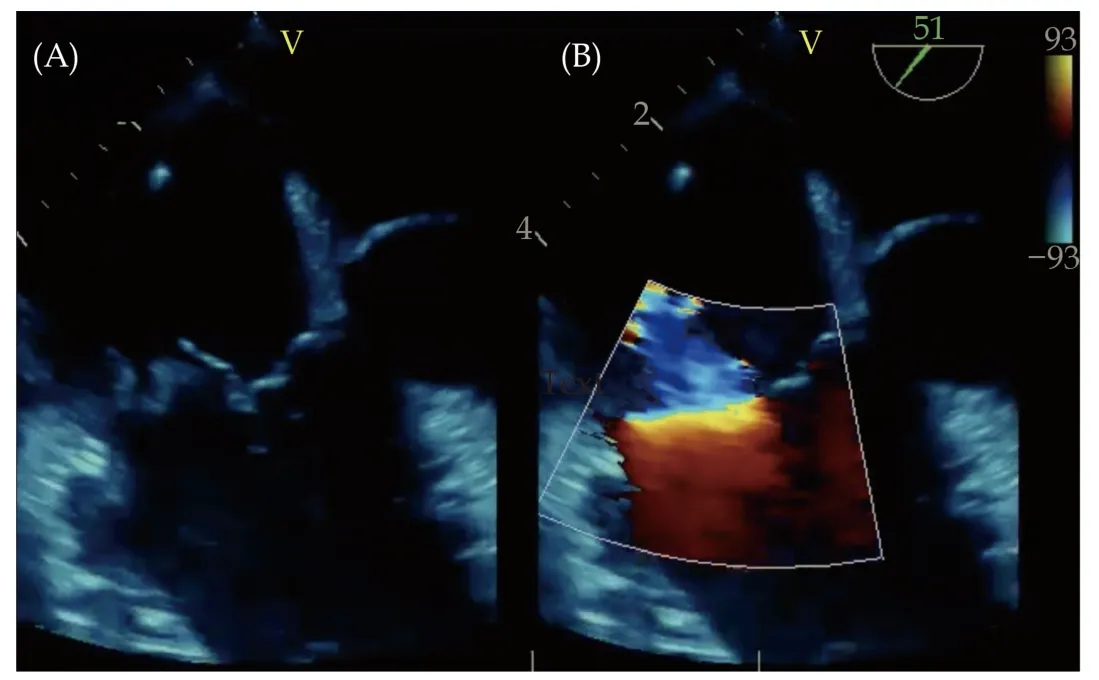
Figure 1 Transesophageal echocardiogram showing mid-esophageal view of tricuspid valvular apparatus.(A): Disruption in continuity of anterior leaflet of tricuspid valve; and (B): color flow imaging of tricuspid valve with torrential tricuspid regurgitation.
ACKNOWLEDGMENTS
All authors had no conflicts of interest to disclose.
 Journal of Geriatric Cardiology2023年4期
Journal of Geriatric Cardiology2023年4期
- Journal of Geriatric Cardiology的其它文章
- A rare cause of pulmonary hypertension in an elderly woman
- How to effectively manage the refractory coronary thrombus? A systemic mini-review
- Safety of butylphthalide and edaravone in patients with ischemic stroke: a multicenter real-world study
- Prevalence and incidence of heart failure among community in China during a three-year follow-up
- Minimally invasive valve surgery: pushing boundaries over the eighty
- Feasibility and clinical benefits of the double-ProGlide technique for hemostasis after cryoballoon atrial fibrillation ablation with uninterrupted oral anticoagulants