
Prevalence and incidence of heart failure among community in China during a three-year follow-up
2023-05-23 04:26LuFUJunRongJIANGWeiDongLINHuiYiLIUShuYuJINXingDongYEYanLinCHENSiJiaPUYangLIUShangFeiHEShuLinWUHaiDENGYuMeiXUE
Journal of Geriatric Cardiology 2023年4期
Lu FU, Jun-Rong JIANG, Wei-Dong LIN, Hui-Yi LIU, Shu-Yu JIN,2, Xing-Dong YE,Yan-Lin CHEN, Si-Jia PU,3, Yang LIU, Shang-Fei HE, Shu-Lin WU,5, Hai DENG,6,✉, Yu-Mei XUE,5,✉
1.Department of Cardiology, Guangdong Cardiovascular Institute, Guangdong Provincial People’s Hospital, Guangdong Academy of Medical Sciences, Guangzhou, China; 2.The Second School of Clinical Medicine, Southern Medical University,Guangzhou, China; 3.School of Medicine, South China University of Technology, Guangzhou, China; 4.Department of Cardiology, the First Affiliated Hospital of Guangzhou Medical University, Guangzhou, China; 5.Guangdong Provincial Key Laboratory of Clinical Pharmacology, Research Center of Medical Sciences, Guangdong Provincial People’s Hospital, Guangdong Academy of Medical Sciences, Guangzhou, China; 6.Qinghai Province Cardio Cerebrovascular Disease Specialist Hospital, Xining, China
✉ Correspondence to: doctordh@hotmail.com (DENG H); xymgdci@163.com (XUE YM)https://doi.org/10.26599/1671-5411.2023.04.008
ABSTRACT BACKGROUND Epidemiological surveys on heart failure (HF) in Chinese community are relatively lacking.This study aimed to estimate the prevalence and incidence of HF among community residents in southern China.
Heart failure (HF) has a worldwide diffusion with an incidence approaching 21 per 1000 population after the age of 65 years in America,[1]and affecting nearly 38 million patients throughout the world.[2]As a major cause of mortality, morbidity, namely hospitalizations, and poor quality of life, it has become a major burden in developed countries.[3]
Prevalence of HF can be estimated at 1%-2% in the western world and the incidence approaches 5-10 per 1000 persons per year.[4]Estimates of the occurrence of HF in the developing countries are largely absent.[3,4]In 2000, it had been reported the prevalence of chronic HF in the Chinese aged 35-74 years was 0.9% in a cross-sectional survey involving ten provinces.[5]The China Hypertension Survey reported that 1.3% of the Chinese adult population aged ≥ 35 years had HF in 2019,while no significant differences in gender subgroups had been found.[6]Even fewer reports on the incidence of HF in Chinese.Recently, a retrospective cross-sectional study designed to determine the prevalence and incidence of HF in the Chinese aged ≥ 25 years from outpatient and inpatient from 2013 to 2017 reported that agestandardized prevalence and incidence of HF were 1.10% and 275 per 100,000 person-years.[3]
Epidemiological surveys on HF in Chinese community populations are relatively insufficient.This prospective community-based study aimed to understand the epidemiological characteristics of HF and its associated risk factors in the Chinese community populations.
METHODS
Study Population
The baseline data collection of Guangzhou Heart Study began in July 2015 and completed in August 2017.[7]Permanent residents aged ≥ 35 years from the randomly chosen communities in Guangzhou, China were recruited into this study during three mobilization rounds of door-to-door visits or telephone contacts and using a randomized multistage cluster sampling.[7]The population inclusion and exclusion criteria for the baseline survey have been reported in detail before.[7-9]
A total of 12,013 community populations aged ≥ 35 years were included at baseline, of which 3557 community populations were aged ≥ 65 years.After a three-year interval, the latter 3557 individuals received re-investigated with the same surveys as baseline.A total of 2597 subjects responded to the second phase of the study.
Public Involvement
The public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Definitions
Patients with HF were defined as those who had been diagnosed with one of following diagnoses as listed in the International Classification of Diseases 10threvision codes: (1) HF; (2) hypertensive heart and renal disease with congestive HF; (3) hypertensive heart disease with congestive HF; (4) hypertensive heart and renal disease with both congestive HF and renal failure; (5) rheumatic HF; (6) other functional disturbances following cardiac surgery; (7) aneurysm of heart; (8) cardiomyopathy; (9) cardiomyopathy in diseases classified elsewhere; (10) ischemic cardiomyopathy; and (11) cardiomyopathy in the puerperium.Those who had been diagnosed with cardiac insufficiency, cardiac dysfunction, cardiogenic shock, cardiac asthma, cardiogenic pulmonary edema, cardiac amyloidosis, cardiac aneurysm, New York Heart Association class II to IV, Killip class II to IV,cardiomyopathy, rheumatic HF, and noncompaction of ventricular myocardium, were also identified as HF based on the facts of clinical practice in China.[3]
Statistical Analysis
The prevalence of HF according to the categories grouped by demographic characteristics including age, gender, body mass index, personal history, and with or without related cardiovascular combinations was compared by the independent samplest-test or theKindependent samples test of the nonparametric statistical tests.Multivariate logistic regression models were developed to investigate the associations between the prevalence or incidence of HF and baseline personal history of illness or new-onset complications.The odds ratio (OR) with 95% confidence interval (CI) was calculated to assess the associations.All statistical analyses were conducted with SPSS 22.0 (SPSS Inc., IBM, Chicago, IL, USA).All statistical tests were two-sided, and aP-value < 0.05 was considered to be statistically significant.
RESULTS
Prevalence of HF and Its Risk Factors
A total of 12,013 residents were enrolled, and 11,634 residents completed the entire data collection in the baseline.Among these participants, 123 participants has been diagnose as HF; thus, the total prevalence of HF in individuals aged ≥ 35 years was 1.06%.
The prevalence of HF increases with aging (OR = 1.49,P< 0.001 per 10 years increasing in age), as showed in Table 1 and Figures 1 & 2.Male had higher risk of HF with an OR of 1.50 (P= 0.027).In the age ≥ 55 years, HF prevalence in male was significantly higher than that in female of the same age, especially for those aged 55-65 years and ≥ 75 years (bothP< 0.05, Figure 1).When adjusted for age, the OR of male seemed to come weak (OR =1.43,P= 0.052), while gender-adjusted aging remained a strong risk factor for HF prevalence (OR = 1.48,P< 0.001).
Hypertension, valvular heart disease (VHD), atrial fi-brillation (AF), myocardial infarction (MI), chronic obstructive pulmonary disease (COPD) and smoking history were closely related to the prevalence of HF in community residents, with ORs of 3.52, 6.60, 12.84, 1.49,2.89 and 1.71, respectively (allP< 0.05).When adjusting for age and gender, residents with VHD, AF, COPD,or smoking history had statistically significant higher risk for HF (allP< 0.05, Figure 2).

Table 1 Prevalence of HF and related risk factors in people over 35 years at baseline.

Continued
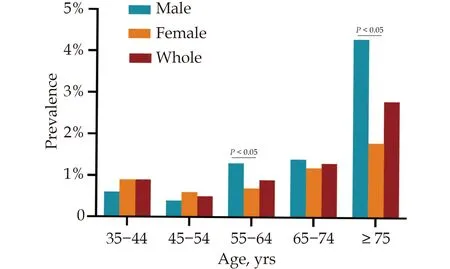
Figure 1 Age-specific prevalence of heart failure in the baseline population.
Incidence of HF and Its Risk Factors
In the first phase of the study, there were 3557 people aged ≥ 65 years, of which 2597 people completed the follow-up visit three years later.During the three-year follow-up, 14 people died, of which three people died of cardiovascular disease (CVD), including one case of acute MI and two cases of cerebral hemorrhage caused by essential hypertension.The other 11 cases died of non-cardiogenic diseases.Among the 14 dead patients,one patient had a baseline left ventricular ejection fraction(LVEF) of 49%, and the rest had a baseline LVEF of more than 65% with no significant reduction in LVEF during follow-up.
A total of 36 HF patients existed in baseline, accounting for 1.39% in the elderly residents.HF increased by 66 during three years, accounting for an HF incidence in individuals above 65 of 847 per 100,000 personyears (826 and 860 per 100,000 person-years in male and female, respectively;P= 0.898).There were 22 new cases of AF, 66 new cases of VHD, 192 new cases of hypertension, 102 new cases of diabetes mellitus (DM), 50 cases increase in hyperthyroidism, 168 cases of COPD, 137 cases of MI, and 319 new cases of chronic kidney disease(CKD).Reassuringly, smoking and alcohol consumption decreased by 265 cases and 30 cases, respectively (Table 2).
As shown in Table 3, baseline AF, VHD, and DM were closely associated with HF incidence, through multivariate regression analysis with stepwise model with ORs of 6.26, 4.59 and 2.64, respectively (allP< 0.05).Age- and gender-adjusted ORs for individuals with baseline AF,VHD or DM getting HF in their future were 5.05, 3.99 and 2.11, respectively (allP< 0.05), compared to those without.
As shown in Table 4, the correlation between new cardiovascular comorbidities and the incidence of HF during follow-up was performed via stepwise multivariate regression analysis.New-onset AF, VHD, and MI were statistically associated with new-onset HF (OR = 16.36,3.26, 7.54, respectively; allP< 0.05).After adjusted for age and gender, new-onset AF and MI remained to be strong predictive factors of HF incidence (OR = 14.41,8.54, respectively; bothP< 0.05).
DISCUSSION
Prevalence of HF
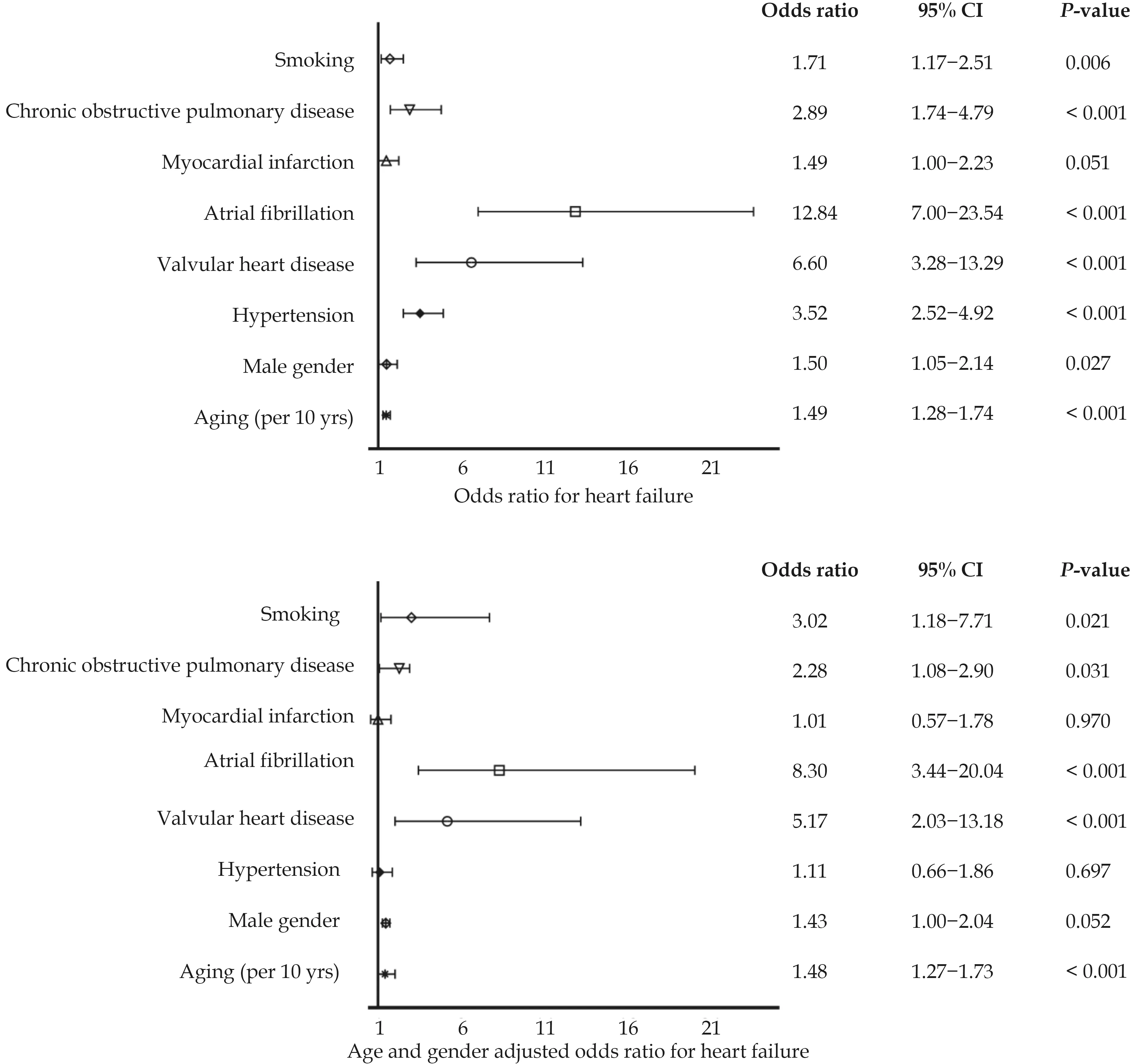
Figure 2 Association of age, gender, and cardiovascular comorbidities with the prevalence of heart failure.
Prevalence of HF could be estimated at 1%-2% in the western world.[4]In a United States population-based study, the prevalence of HF was 2.2% (95% CI: 1.6%-2.8%),increasing from 0.7% in persons aged 45-54 years to 8.4% for those aged 75 years or older in 2003.[10]A few epidemiological studies focused on HF in the Chinese population, and most of them involved inpatients or outpatients.Including from the first nationwide cross-sectional HF-related survey in 2000, prevalence of chronic HF in the Chinese population aged 35-74 years was 0.9%(0.7% in male and 1.0% in female).[5]And the China Hypertension Survey from 2015 to 2017, reported 1.3% of the Chinese adult population aged ≥ 35 years had HF,while no significant differences were found between male and female.[6]Then in 2017, a population-based study,using records of individuals aged ≥ 25 years from the national urban employee basic medical insurance, came into a conclusion that age-standardized HF prevalence was 1.10% (1.10% among male and female), which increased with increasing age (0.57%, 3.86%, and 7.55% among persons who were 25-64 years, 65-79 years, and ≥ 80 years, respectively).[3]In this survey, it could be concluded that the prevalence of HF in Guangdong community residents was approximately 1.06% among those aged ≥ 35 years, and was 1.39% among individuals aged ≥ 65 years.And HF prevalence increased with aging,which was consistent with the results of previous studies.Age is a major determinant of the risk for CVD and associated with aortic stiffening, myocardial hypertrophy, myocardial fibrosis, and frequently cardiac amyloidosis.[11,12]
Inconsistent reports on the association between the prevalence of HF and gender could been seen.The prevalence of HF in western countries was generally higher in male.[13,14]However, in the HF survey in 2000, prevalence of chronic HF in female was statistically higher than that in male.[5]While, the 2019 China Hypertension Survey[6]and 2021 HF survey by Wang,et al.[3]found no significant differences between male and female.In Wang’s study, male had a slightly higher prevalence than female in the 30-year-old age group to 74-year-old age group, but this gender difference changed in the ≥ 75-yearold age group.[3]In our study, male had statistically significant higher risk of HF with an OR of 1.50 compared with female.Differences in the prevalence of HF between male and female in different age groups also could been seen.In the age of 55 years and above, the prevalence of HF in male was significantly higher than that in female of the same age, especially those aged 55-65 years and≥ 75 years.These were consistent with studies in western countries, rather than previous epidemiological surveys of HF in Chinese population.[15]The reason for this difference between China in 2000 and western countries on gender might be related to the difference in the etiological spectrum of HF.[5]In western countries, coronary heart disease (CHD) and hypertension were the main causes of HF, while rheumatic valve disease is rare.[16]While in China of the same time, rheumatic VHD was still one of the main causes of HF, of which, female were more likely to have.[5]And, we also noticed that in the 2000 survey, the prevalence of HF in the southern China was significantly lower than that in the northern China.[5]The prevalence of HF in southern female was 0.7%,[5]even lower than the that in female in this study.Moreover, the 2000 HF survey was conducted more than 20 years away, during which, non-negligible change had taken places in CVD prevalence and incidence such as CHD, hypertension, and DM, due to the situation of population aging, rapid industrialization, urbanization, obesity, and lifestyle changes.In the national VHD survey in 2021,weighted VHD prevalence was 3.8%, with an estimated 25 million patients in China and the burden of rheumatic VHD was mainly derived from the older population, especially those aged 75 years and older.[17]Another fiveyear epidemiological survey of VHD reported that rheumatic VHD remains the leading etiology in southern China, with a significant increase in the prevalence of ischemic, congenital and degenerative VHD.[18]
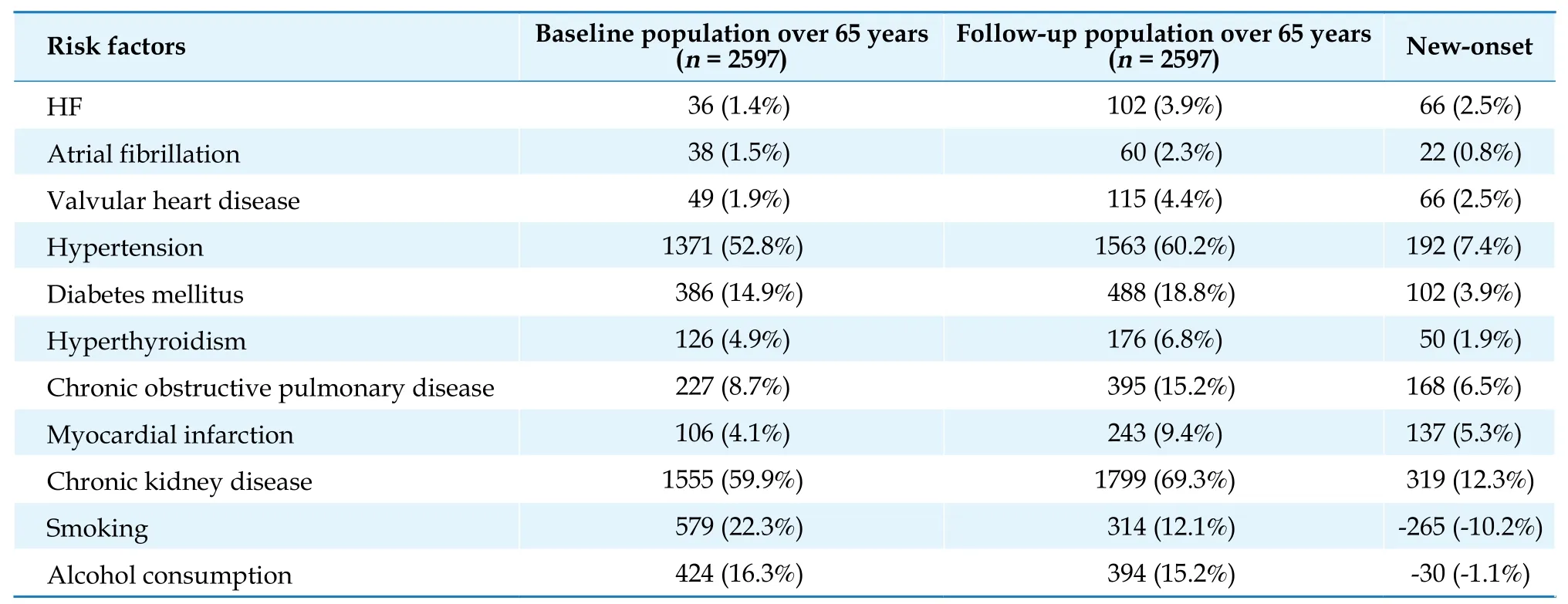
Table 2 New-onset HF and other cardiovascular comorbidities in the population over 65 years during a three-year follow-up.
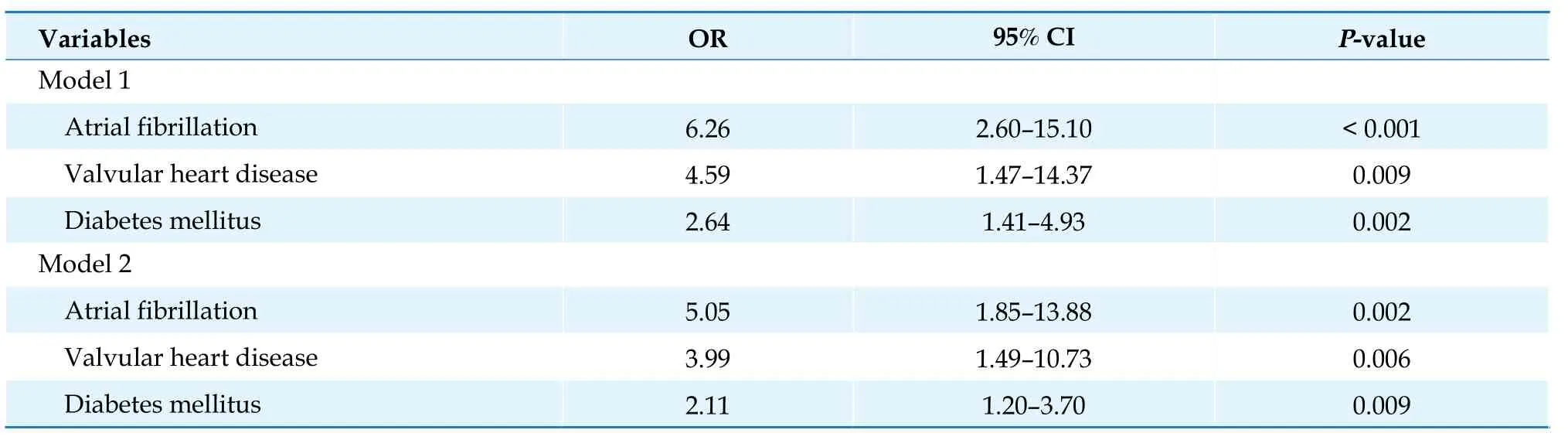
Table 3 Association between baseline risk factors and prevalence of heart failure in residents aged 65 years and above.

Table 4 Association between new-onset risk factors and heart failure incidence in residents aged 65 years and above.
Differences in social factors, environment, lifestyle, and complex interactions among these factors might take responsibility for the inconsistency of HF related comorbidities worldwide.[19]It had been reported in the ASIANHF (the Asian Sudden Cardiac Death in Heart Failure) registry study that hypertension, anemia, CKD, DM, coronary artery disease, AF and obesity were the most common comorbidities for HF in Asia.[20,21]However, results from China-HF registry study showed that common comorbidities of HF included hypertension, CHD and AF.[22]The main risk factor for HF in people aged ≥ 35 years was VHD, AF, COPD, and smoking in this study.
Incidence of HF
The incidence of HF in western countries was 200-500 per 100,000 person-years as was reported in precious studies.[23,24]Like HF prevalence, incidence is greater in males and the elderly.[23]Incidence for HF was 564 and 327 per 100,000 person-years in male and female, respectively in the Framingham Heart Study,[25]whereas comparable rates were found in Olmsted cohort.[26]The incidence of hospitalization for HF in Taiwan in 2005 was 271.2 per 100,000 population of all ages,[27]and overall HF incidence was only 70 per 100,000 population in a retrospective study in Hong Kong in 1997.[28]The overall crude incidence of HF was 248 per 100,000 patient-years among individuals aged ≥ 25 years and increased with age for both gender in the Chinese population aged ≥ 25 years from outpatient and inpatient.[3]And it was 892 per 100,000 patient-years among patients aged 65-79 years and reached 1655 per 100,000 patient-years among patients aged ≥ 80 years.[3]Besides,HF incidence differed between male and female.[3]Epidemiological study on the incidence of HF among residents in mainland China was limited.In our study, incidence of HF in individuals aged ≥ 65 years were 847 per 100,000 person-years, and no differences had been found between gender, which might be related to the unique living habits, food culture and economic level of Guangzhou, China.
As was reported in studies on western countries, major clinical risk factors for incidence of HF were age, male sex, hypertension, left ventricular hypertrophy, MI,VHD, obesity, DM; and minor clinical risk factors were smoking, dyslipidemia, CKD, albuminuria, sleep-disordered breathing, anemia, increased heart rate, dietary risk factors, sedentary lifestyle, low socioeconomic status, psychological stress.[23]In this survey, individuals with AF or VHD, no matter at baseline or new-onset, had significantly increased risk for progressing HF adjusted for age and gender.Baseline DM, as well as newly MI, were risk factors for HF incidence.
The remarkable economic growth that has occurred in China over recent decades has provided wealth and prosperity to large sections of the population.Accompanying this achievement, however, has been a shift in the patterns of disease from predominantly infectious to noncommunicable diseases, with CVD being established as the leading cause of premature morbidity and mortality in China.[29]Epidemiological investigation indicated a transition in CVD epidemiology including the rising burden from atherosclerotic CVD, varied regional epidemiological trends in the subtypes of CVD, and increasing ageing of patients with CVD, owing to interrelated changes in demography, environment, lifestyle, and health care.[30]Changes in the spectrum of these CVDs imply a potential shift in HF-related risk factors.This study provided specific and practical guidance for the current management of HF by studying the risk factors related to HF prevalence and incidence.
LIMITATIONS
The present study has limitations inherent to its design with a relatively small regional sample size from southern China, rather than the nationwide population; thus, the findings in this study represented southern China.The criteria for HF diagnosis in this study were based on the patient’s previous history and assessment of HF according to the New York Heart Association class by the cardiovascular specialist during a cross-sectional survey,[3]rather than cardiac ultrasound and blood indexes (including N-terminal pro-B-type natriuretic peptide/B-type natriuretic peptide).
CONCLUSIONS
In Guangzhou, China, prevalence and incidence of HF were high among community residents.Both pre-existing and new-onset CVDs were associated with HF incidence.It is necessary to intervene in the new-onset cardiovascular risk factors to reduce the incidence of HF, as well as manage the existing diseases of HF.
ACKNOWLEDGMENTS
This study was supported by the National Natural Science Foundation of China (No.81870254), the Guangdong Provincial Clinical Research Center for Cardiovascular Disease Foundation (No.2020B1111170011), and the Science and Technology Programs of Guangdong Province (No.2019B020230004).All authors had no conflicts of interest to disclose.
 Journal of Geriatric Cardiology2023年4期
Journal of Geriatric Cardiology2023年4期
- Journal of Geriatric Cardiology的其它文章
- Characteristics and in-hospital mortality of elderly patients with heart failure in Spanish hospitals
- Evaluation of metoprolol standard dosing pathway in Chinese patients with acute coronary syndrome: a prospective multicenter single-arm interventional study
- Feasibility and clinical benefits of the double-ProGlide technique for hemostasis after cryoballoon atrial fibrillation ablation with uninterrupted oral anticoagulants
- Minimally invasive valve surgery: pushing boundaries over the eighty
- Safety of butylphthalide and edaravone in patients with ischemic stroke: a multicenter real-world study
- How to effectively manage the refractory coronary thrombus? A systemic mini-review