
A sutureless technique for securing leaking sclerotomies with viscoelastic substances in 23-gauge microincision vitrectomy surgery
2023-05-15 09:20MengLiQuanYongYiJingHaiMaoYanHongLiaoYanYanWangQinKangLuYanGong
Meng Li, Quan-Yong Yi, Jing-Hai Mao, Yan-Hong Liao, Yan-Yan Wang, Qin-Kang Lu,Yan Gong
1Health Science Center, Ningbo University, Ningbo 315211,Zhejiang Province, China
2Department of Ophthalmology, Ningbo Eye Hospital, Ningbo 315042, Zhejiang Province, China
3Department of Ophthalmology, The Affiliated People’s Hospital of Ningbo University, Ningbo 315040, Zhejiang Province, China
Abstract
INTRODUCTION
Minimally invasive vitreoretinal surgery has developed rapidly since O’Malley and Sr Heintz[1]developed the first transscleral three-channel 20-gauge vitrectomy system in the early 70s.Microincision vitrectomy surgery has many advantages, such as short operation time[2], low inflammation of the anterior and posterior segments of the eye after surgery[3], no conjunctival cicatrix after surgery[4-5],and reduced dry eyes after surgery[6], which improve the comfort of patients after surgery.However, various complications follow, such as bleeding from the incision,hyperplasia of incision tissue, and vitreoretinal traction[7-9].Moreover, leaking sclerotomy is prone to postoperative hypotony, and sclera-free closure also leads to a higher risk of endophthalmitis after microincision vitrectomy surgery than traditional vitrectomy[10].Suture is the most conventional treatment for the postoperative leaking sclerotomies[11].However, sutures exacerbate the postoperative inflammatory response and increase the patients’discomfort owing to the local hyperplasia of suture knots.It is recommended that highly myopia, history of previous vitrectomy, history of eye trauma, and the absence of tamponade increase the needfor suturing[12-14].Substitutes for suturing include application of tissue adhesives[15-16], conjunctival cauterization[17-18], and scleral needling[19].Nonetheless, each of these techniques have associated limitations in terms of to effectiveness, availability of materials, and excess damage.

Table 1 Preoperative characteristics of patient
In this paper, a new method is introduced to close leaking sclerotomies with 23-gauge vitrectomy combined with intraocular gas filling with viscoelastic substances.Then,the effectiveness of the new method as an alternative for the closure of incisions is assessed.
SUBJECTS AND METHODS
Ethical ApprovalThe research adhered to the principles of the Declaration of Helsinki, and was approved by the Ningbo Eye Hospital Ethics Board (2019-qtky-14).All patients received clear information about the study and signed a written informed consent.No stipend was applied through the study.Research DesignThis program is a retrospective comparative analysis.All cases were from Ningbo Eye Hospital and underwent operation by the same vitreoretinal surgeon (Gong Y) in Ningbo, China.A retrospective comparative analysis was made on the cases who underwent 23-gauge vitrectomy combined with intraocular gas filling in the control group(before the introduction of the viscoelastic substances technique, June 2019 to September 2020) and the new technique group (after the introduction of the viscoelastic substances technique, October 2020 to December 2021).Comparative data included the incidence of postoperative hypotony and other related complications.Preoperative data included the patients’age, gender, operative eye, best-corrected visual acuity, and lens status.The data obtained during the operation included the details of surgery, the number and location of sutured sclerotomies, and the use of viscoelastic substances technique.Complications, such as hypotony,subconjunctival hemorrhage, and endophthalmitis during days 1 to 2 and days 3 to 20 after surgery, were retrospectively analyzed, and the pooled data were compared.
Surgical TechniquesIn the control group, a small amount of balanced salt solution was dropped at the incision site to check the incision closure after removal of the trocar cannula postsurgery.Poor closure was indicated by the presence of bubbles at the incision, which was then massaged with a cotton swab and pressure was applied.If the incision still did not close well, the operation was repeated and extended if necessary.If the wound still could not be closed, the leaking sclerotomy was closed with sutures.In the new technique group, a small amount of viscoelastic substances was injected at the incision immediately after removal of the trocar cannula post-surgery.This was followed by gentle massage with a cotton swab for several seconds.Then, a small amount of balanced salt solution was dropped at the incision site to check the incision closure.This procedure could be repeated 2-3 times while reducing the eyelid opener and relieving eyeball pressure.If leakage was detected after three repetitions, the incision was sutured.Otherwise, the incision was considered closed.Ⅴideos of the surgical technique are provided as supplementary materials.
Statistics AnalysisThe incidences of postoperative hypotony and other postoperative complications were compared between the control group and new technique group using Chi-square test.Other variables, including postoperative intraocular pressure and best-corrected visual acuity, were described by standard deviation and compared using independent samplet‐test.Descriptive statistics are used to reflect the demographic and surgical details of the patients.SPSS software version 25.0(SPSS, Inc., USA) was used in all statistical analyses.P<0.05 was considered significantly different.
RESULTS
A total of 174 eyes, 84 were from the control group and 90 were from the new technique group, that underwent pars plana vitrectomy during the 30-month study period were reviewed and included in this study (Table 1)[20-21].The sample consisted of 39.1% (68/174) men with a mean age of 61.94.The preoperative lens status was phakic in 68.4% (119/174),intraocular lens in 31.6% (55/174), and the preoperative mean intraocular pressure was 12.01 mm Hg.The differences between the two groups were not statistically remarkable.In addition to 23-gauge vitrectomy, phacoemulsification combined with intraocular lens implantation was performed in 33.9% (59/174) cases.
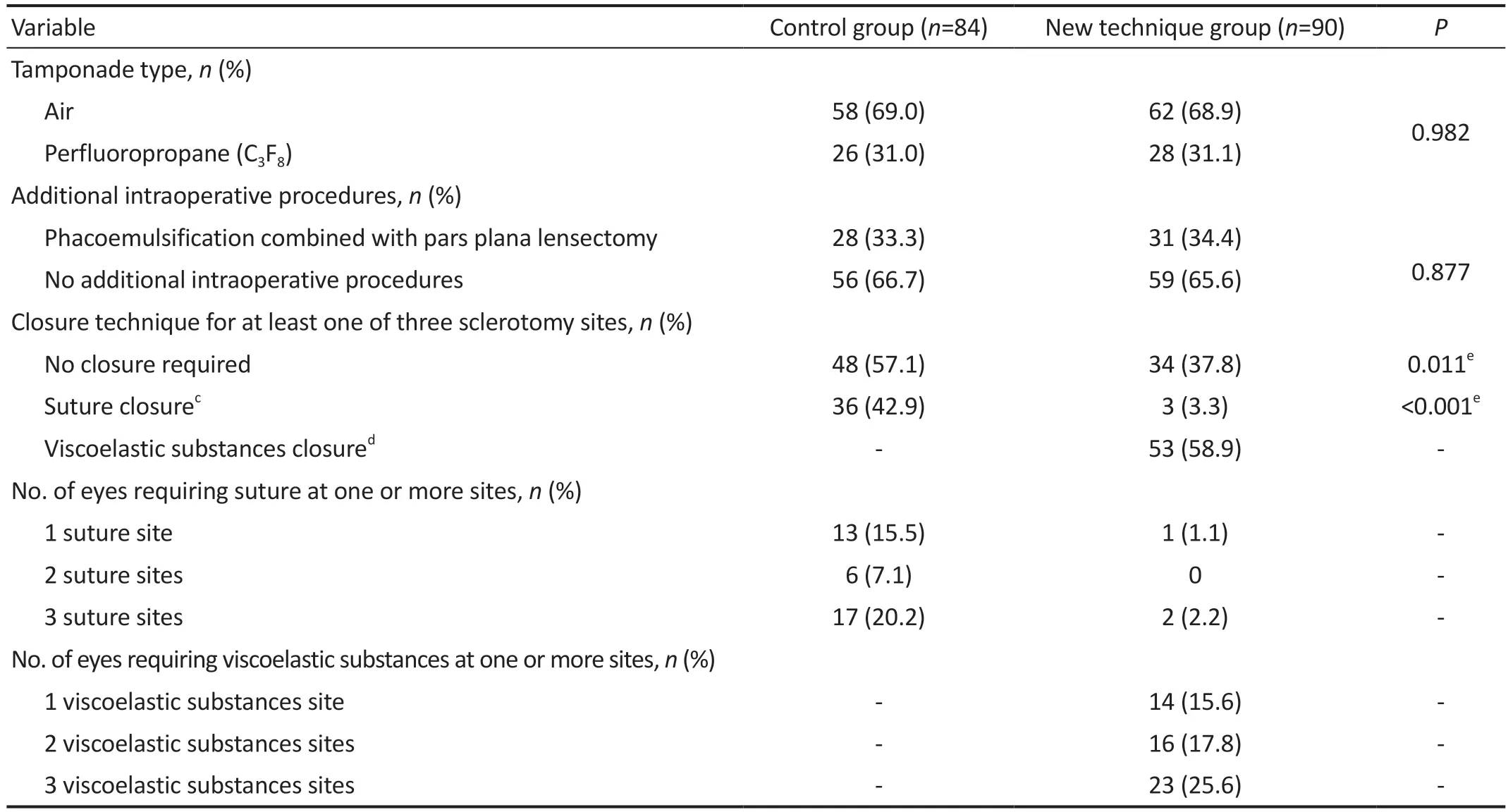
Table 2 Operative details for the control group and the new technique group
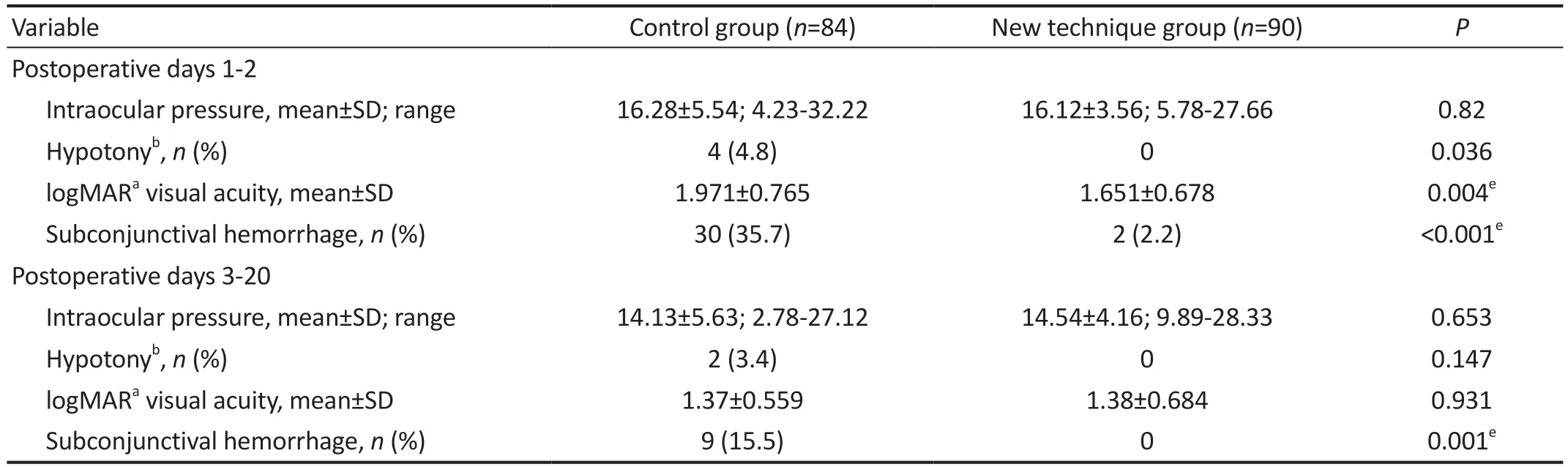
Table 3 Postoperative details for the control group and the new technique group
In control group, 42.9% (36/84) of the eyes and 30.2%(76/252) of leaking sclerotomies eventually required sutures to close, with 27.4% (23/84) of all eyes requiring more than one site sutured as shown in Table 2.By contrast, in the new technique group, the number of eyes and leaking sclerotomies requiring sutures were significantly reduced to 3.3% (3/90,P<0.001) and 2.6% (7/270,P<0.001) respectively.In the new technique group, 58.9% (53/90) of the eyes required closure of incisions with viscoelastic substances, with 41.5% (39/94)of eyes required closure of more than one leaking sclerotomy with viscoelastic substances.
The postoperative intraocular pressure during days 1 to 2(P=0.82), days 3 to 20 (P=0.653) was not significantly between the control group and new technique group (Table 3)[20-21].Hypotony did not occur in the new technique group within the first two days after surgery, which indicates that the result of the new technique group was better than that in the control group (P=0.036).No significant difference was also observed between the two groups between days 3 to 20 after surgery (P=0.147).The visual acuity of the new technique group during days 1 to 2 after surgery was significantly better than that of the control group (P=0.004).The two groups had no significant differences during days 3 to 20 after surgery(P=0.931).The incidences of subconjunctival hemorrhage in clinical examination during days 1 to 2 and days 3 to 20 after surgery in the new technique group were significantly lower than those in the control group (P<0.001,P=0.001).No other complications associated with viscoelastic substances were noted during the study period.
Postoperative days 3 to 20 data not available for 26 and 30 patients assigned to the control group and the new technique group, respectively.
DISCUSSION
The research is a retrospective study of the use of viscoelastic substances technique to close leaking sclerotomies after 23-gauge vitrectomy.According to our results, with the introduction of the viscoelastic substances technique and incorporation into surgical practice, the number of eyes that required suture for closure decreased from 42.9% to 3.3%,with the incidence of hypotony during days 1 to 2 after surgery was 0, which was considerably better than that in the control group.Moreover, no remarkable difference in the incidence of hypotony was found during days 3 to 20 after surgery compared with the control group.According to our study, the incidence of hypotony with viscoelastic substances technique during days 1 to 2 after surgery was 0, which was considerably lower than that of hypotony after small-gauge sclerostomy (3.8%-6.5%)[12,22].Notably, there were three cases in new technique group that had leaking sclerotomy which could not be closed by the viscoelastic substances and were eventually closed through sutures.These cases were all highly myopia or had eye trauma.This result means that the eye axis of highly myopia eyes is too long and the eyeball wall is weak.The poor seal of the eyeball caused by the previous injury was the possible reason for the failure of viscoelastic substances technique.In addition, we also found that in the cases of intraoperative basal vitreous resection that was relatively incomplete, which result in a small number of vitreous incarcerations in leaking sclerotomy, the incisions often have better closure.For example, eyes which lens had to be preserved in surgery to prevent intraoperative damage to the lens, or eyes which had diabetic retinopathy surgery to avoid iatrogenic tears that lead to retinal detachment all likely to have better closure.
The viscoelastic substances itself is a transparent macromolecular colloidal agent with certain adhesive, sterile,non-toxic, and non-antigenic properties[23-24].It has good biocompatibility and has the functions of maintaining anterior chamber depth, protecting corneal endothelial cells, preventing intraoperative bleeding, and separating adhesions[25-29].At present, it is widely used in many ophthalmic microsurgeries,such as phacoemulsification, penetrating keratoplasty, and ocular trauma.With the help of three characteristics of the viscoelastic substances, first of which is macromolecular colloidal feature, the second is its good biocompatibility with the human eye, and the third is its good adhesion, the leaking sclerotomies could be closed.The mechanism of wound closure in this method may be the blocking of the sclerotomy sites, thus preventing intraocular gas loss, maintaining intraocular pressure.

Figure 1 Comparison of postoperative anterior segment photographs A: Suture closure; B: Viscoelastic substances closure.
The viscoelastic substances technique is easy to use.It greatly shortens the surgery time, reduces conjunctival injury,mitigates postoperative inflammation, and improves patients’comfort.Abouammohet al[30]reported a method to close incision through using balanced salt solution at the edge of the scleral tunnel.In their study, the postoperative incidence of hypotony was 1.32%.However, no control group was established in their study.Felfeliet al[19]reported a method of sealing incisions by scleral needle technique.Although,in their study, the incidence of postoperative subconjunctival hemorrhage was higher, the viscoelastic substances method did not cause secondary damage to the eyeball.Subconjunctival hemorrhage was not observed in our cases (Figure 1).Nevertheless, the use of viscoelastic substances is limited when subconjunctival hemorrhage or subconjunctival hematoma occurs during surgery, because the edge of the scleral tunnel would be difficult to find if the surgical field is blurred, and the conjunctiva at the leaking sclerotomy might need to be cut.Furthermore, when treating patients with fragile eyeball walls,this technique may not seal the incision well and require suture for closure.There were other types of tissue glues used to close conjunctival incisions reported previously[31], which can be subdivided into synthetic tissue glues and biologic tissue glues.The synthetic tissue glues are nonbiodegradable, which may induce an inflammatory foreign body reaction.The biologic tissue glues (e.g., fibrin-based glues) are biodegradable and induce less inflammation.But these fibrin glues use human thrombin, this blood product may lead to the risk of disease transmission and anaphylactic reaction.In addition, it is very complex to prepare the fibrin-based glues.Compared with these tissue glues, viscoelastic substances are non-toxic and non-antigenic, which can reduce discomfort and the risk of allergy in patients, therefore improve safety.A limitation of our study was the small sample size.Due to various factors, some patients did not adhere to follow-up after surgery; as a result,not all complications were recorded completely.
In summary, our retrospective study shows that the suture rate of leaking sclerotomies decreased from 42.9% to 3.3% after the introduction of viscoelastic substances technique.Moreover,the proposed method had no noticeable negative impacts on intraocular pressure and postoperative visual acuity recovery.The results indicated that viscoelastic substances technique is an effective, simple, and safe method for the sutureless sealing of leaking sclerotomy in microincision vitrectomy surgery.
ACKNOWLEDGEMENTS
Foundations:Supported by General Class A of the Zhejiang Medical and Health Science and Technique Plan Project in 2020 (No.2020ky288); Zhejiang Provincial Science and Technique Program of Traditional Chinese Medicine(No.2021ZB268); Health Science and Technique Program of Zhejiang Province (No.2021PY073); Yinzhou District Agriculture and Social Development Field Science and Technique Project (No.2021AS0058; No.2020AS0080).
Conflicts of Interest: Li M,None;Yi QY,None;Mao JH,None;Liao YH,None;Wang YY,None;Lu QK,None;Gong Y,None.
 International Journal of Ophthalmology2023年5期
International Journal of Ophthalmology2023年5期
- International Journal of Ophthalmology的其它文章
- Analysis of retinal arteriolar and venular parameters in primary open angle glaucoma
- ldentification and functional analyses of a novel FOXL2 pathogenic variant causing blepharophimosis, ptosis,and epicanthus inversus syndrome
- Protective effects of ferulic acid against ionizing radiation-induced oxidative damage in rat lens through activating Nrf2 signal pathway
- Novel homozygous ADAMTS17 missense variant in Weill-Marchesani syndrome
- Cost analysis of childhood glaucoma surgeries using the US Medicaire allowable costs
- Predicting the prognosis of primary orbital lymphoma by clinical characteristics and imaging features