
Analysis of postoperative ocular surface changes and intervention effect after pars plana vitrectomy in meibomian gland dysfunction dry eye patients
2023-05-15 09:20BoShiLiuJiaoTingWeiZeTongNieMengYangShaoFangPangWenBoLiXiaoRongLiBoJieHuTianjinKeyLaboratoryofRetinalFunctionsandDiseasesTianjinInternationalJointResearchandDevelopmentCentreofSchoolofOptometryTianjinMedicalUniv
Bo-Shi Liu, Jiao-Ting Wei, Ze-Tong Nie, Meng Yang, Shao-Fang Pang, Wen-Bo Li,Xiao-Rong Li, Bo-Jie Hu Tianjin Key Laboratory of Retinal Functions and Diseases,Tianjin International Joint Research and Development Centre of School of Optometry, Tianjin Medical University Eye Hospital,Tianjin 300384, China
Abstract
INTRODUCTION
Meibomian gland dysfunction (MGD) is characterized by chronic and diffuse meibomian gland lesions whose main pathological basis is obstruction of the terminal duct and/or a change in the quality or quantity of eyelid esters.This condition can not only cause abnormal tear film properties, eye irritation, and ocular surface inflammation but also damage the ocular surface and affect visual function; in fact, MGD is the most common cause of severe evaporative dry eye[1].With the aging of the population and the increasing use of video displays, the incidence of MGD in people over 60 years of age within the Asian population is now as high as 46.2% to 69.3%[1-2], and this condition is the main cause of dry eye in this demographic.Eyelid cleaning, application of hot compresses and massage to the meibomian glands,local artificial tear supplements, and local anti-inflammatory treatment can improve patients’ocular symptoms, and these are currently the most commonly used treatment methods[2-4].The Keratograph 5M (K5M), an ocular surface analyser, can non-invasively and objectively capture relevant parameters of the ocular surface, such as average non-invasive tear film break‐up time (NⅠTBUTav), first non‐invasive tear film break‐up time (NITBUTf), and measured tear meniscus height(NTMH).In addition, the K5M is equipped with a noninvasive meibomian gland imaging system, which can clearly observe various types of meibomian gland abnormalities,including loss, shortening, expansion and distortion.The LipiⅤiew interferometer can accurately and non‐invasively measure the thickness of the lipid layer, which is of great significance for the diagnosis and evaluation of MGD.
Studies have shown that the incidence of MGD before cataract is as high as 52%[5].Although postoperative vision improved, as a result, the tear film quality of patients decreased, dry eye symptoms were aggravated, and subjective experience deteriorated, which was very serious in people with preoperative dry eye.Hanet al[6]and El Ameenet al[7]suggested that cataract surgery may damage the meibomian gland, but the mechanism was not clear.In MGD patients with cataracts, researchers found that preoperative meibomian gland cleaning, hot compresses and massage were more effective in alleviating the development of postoperative dry eye than postoperative strengthening of anti-inflammatory drug treatment[8-9].
Ⅴitrectomy, coming into the era of minimally invasive surgery,is becoming the main surgical method for vitreous and retinal disease.Compared with the 20G pars plana vitrectomy(PPⅤ) system, the results show that the minimally invasive system causes less damage to patients, saves operation time and reduces postoperative inflammation[10].However, some scholars have proposed that the density of conjunctival cup cells decreases[11]or the distribution of mucin changes after vitrectomy[12], suggesting the development of dry eye after this procedure.For patients over 60 years old with fundus lesions combined with cataracts, vitrectomy is usually performed along with phacoemulsification and intraocular lens implantation.
In clinical practice, doctors focus primarily on fundus changes and postoperative visual acuity; ocular surface changes are easily overlooked.However, many patients have reported that postoperative itching, redness and dryness are aggravated after PPⅤ, which seriously affects postoperative quality of life and decreases surgical satisfaction.There have been many studies of dry eye after corneal surgery[13], cataract surgery[14]and glaucoma surgery[15], but few studies have examined dry eye after phacovitrectomy.The purpose of this study was to observe the changes in the eye surface after vitrectomy combined with cataract surgery in patients with mild to moderate MGD by two new ocular surface detection instruments, the K5M ocular surface analyser and the LipiⅤiew interferometer, and to evaluate the changes in objective indexes after preoperative hot compress application and meibomian gland massage as well as preoperative and postoperative supplementation with 0.1%sodium hyaluronate to evaluate whether relevant treatment measures can improve the ocular surface condition of patients with MGD.
SUBJECTS AND METHODS
Ethical ApprovalThe Institutional Review Board approved this prospective experiment (No.2020KY(L)-31), which was registered at http://www.clinicaltrials.gov (No.NCT05771194).We explained the principles and methods and complications of treatment to the patient, and obtained the patient’s informed consent.All procedures were conducted in accordance with the principles of the Declaration of Helsinki.
Study SubjectsThis was a prospectively randomized study.Sixty people diagnosed with vitreoretinal disease with mild to moderate MGD who planned to undergo posterior vitrectomy combined with intraocular lens implantation were included from February 2021 to November 2021 and were randomly divided into control group A and treatment group B.The classification criteria for MGD were based on the consensus of experts on MGD diagnosis and treatment in China in 2017[16].Patients who complained of one of the subjective symptoms,such as dry eye, foreign body sensation, burning sensation,fatigue, discomfort, redness of the eyes, visual fluctuation, etc.,as well as Ocular Surface Disease Index (OSDI) questionnaire≥13 points and NⅠTBUT<10, were diagnosed with dry eye.Patients with abnormal meibomian gland openings and eyelid,as well as abnormal meibomian ester secretion and ocular symptoms, were diagnosed with meibomian gland dysfunction.The criteria for mild MGD were as follows: mild symptoms,intermittently normal eyelid margin or mild hyperaemia,lipid cap formation, cloudy secretion, secretion of 3-4 glands when squeezing the 5 lower eyelid glands, meibomian gland loss of less than 1/3, normal cornea and no epithelial injury.Additionally, the criteria for moderate MGD were as follows:mild or moderate symptoms, continuous, blunt and thickened eyelid margin, obstruction and swelling of meibomian gland orifice, cloudy and granular secretions, extrusion of 5 glands in the middle of the lower eyelid, secretion of 1-2 glands when squeezing the 5 lower eyelid glands, meibomian gland loss of 1/3 to 2/3, mild to moderate corneal epithelial injury, occurring in a peripheral location.The patients had no objection to treatment and agreed to complete follow-up.The exclusion criteria were as follows: 1) eye trauma or eye surgery within the prior 6mo; 2) use of drugs that affect tear secretion and the stability of the tear film (including anti-glaucoma drugs,cortisol drugs,etc.) within the prior 6mo; 3) other diseases that affect the function of the eye surface, such as meibomian gland cysts, blepharitis, eyelid valgus, incomplete closure, chronic tear cystitis, corneal disease, glaucoma, or optic neuropathy;4) intraoperative suture fixation or closure of a corneal,conjunctival, or scleral incision; 5) long-term postoperative intraocular hypertension that could not be controlled easily with oral drugs and required puncture and drainage through the anterior chamber; 6) postoperative corneal epithelial defects lasting more than 1wk or necessitating the use of contact lenses for treatment; 7) the need for a second operation during the study follow-up.
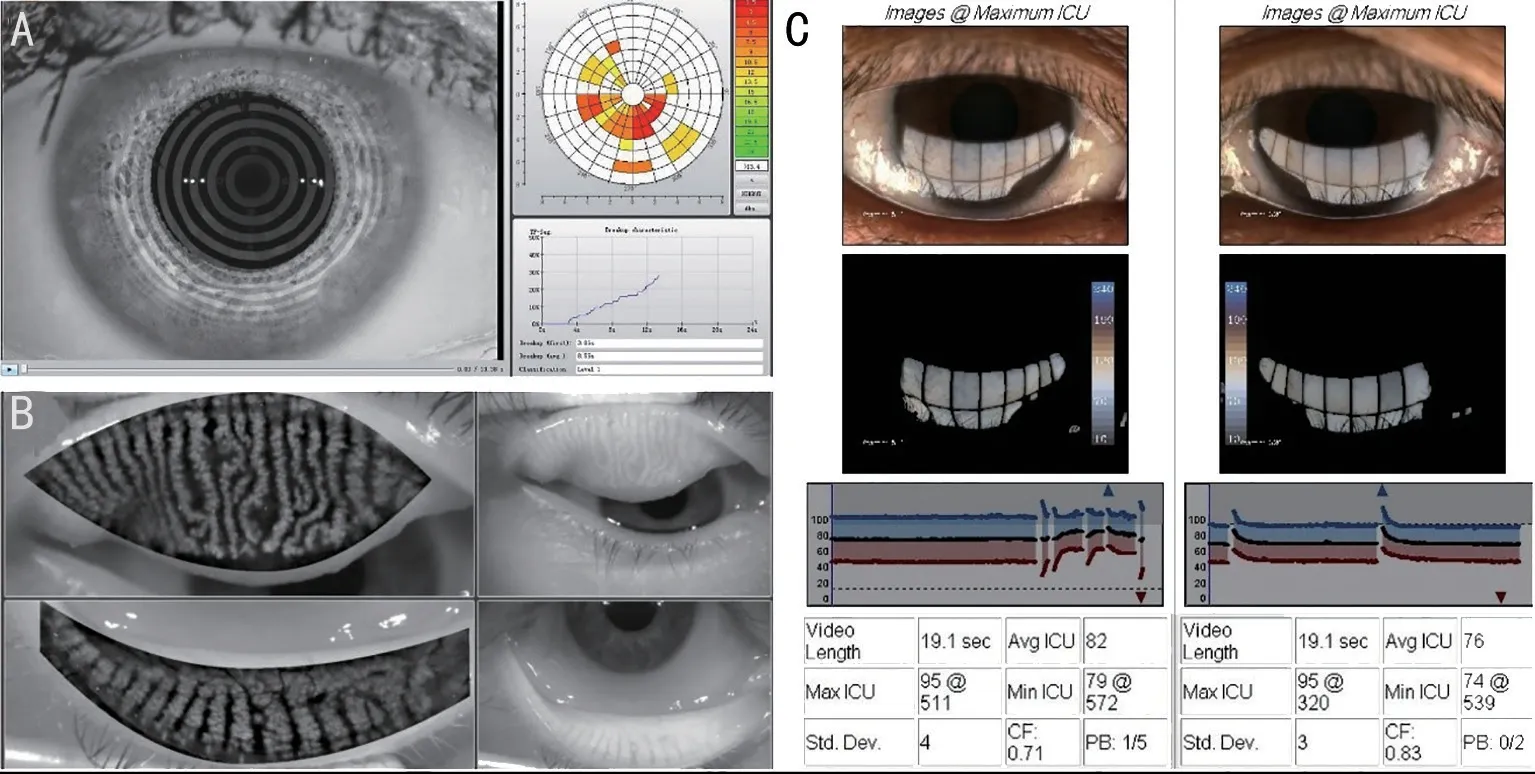
Figure 1 Test result page A: NITBUT measurement results; B: Meibomian gland photography results; C: LLT measurement results.NITBUT: Noninvasively measured tear film break-up time; LLT: Lipid layer thickness.
Eye ExaminationsAll patients underwent NITBUTav,NITBUTf, and NTMH measurement as well as meibomian gland photography with a non-invasive, comprehensive eyesurface analyser (Oculus, Germany); lipid layer thickness (LLT)and partial blink rate (PBR) were measured with a LipiⅤiew Eye Surface Interferometer (Tearscience, USA).These measurements were taken before surgery (in the case of Group B, before hot compresses and meibomian gland massage)and 1wk, 1, and 3mo after surgery.Slit-lamp microscopy was used to examine the anterior segment and the anterior 1/3 of the vitreous.After mydriasis, the fundus was examined in detail with the help of a 90 D anterior lens (ⅤOLK, USA).Uncorrected visual acuity, best corrected visual acuity, and intraocular pressure were recorded.
The NITBUT values were measured using a non-invasive ophthalmic analyser; the patients were instructed to blink 2 times after a normal blink, focus their eyes, and then refrain from blinking until the Placido ring projected onto the cornea was broken; the duration was recorded.On this basis,tear film quality can be divided into three grades: Level 0:NⅠTBUTf≥10s, NⅠTBUTav≥14s, normal; Level 1: NⅠTBUTf:6‐9s, NⅠTBUTav: 7‐13s, critical; Level 2: NⅠTBUTf≤5s,NⅠTBUTav≤7s, dry eye (Figure 1A).The lacrimal river was imaged, and the height of the lacrimal river directly below the centre of the pupil was measured with the built-in measurement tool of the system.Each patient was examined by the same ophthalmologist three times, and the average of the three measurements was used as the final result.The Meibo-Scan mode was selected.Then, the upper and lower eyelids were turned outward, and morphological images of the meibomian glands were obtained under an infrared light source.The shortening and loss of meibomian glands were observed and recorded on the following scale: The absence of meibomian gland loss (MGL) corresponded to a score of 0 point, an MGL ratio of less than 1/3 was assigned 1 point, an MGL ratio of 1/3 to 2/3 received 2 points, and a ratio of >2/3 received 3 points.The upper and lower eyelids of the examined eyes were scored in this manner, and the scores were added to obtain the final score (Figure 1B).
The LipiⅤiew interferometer was used for examination under natural light.The patient was in a sitting position, and the mandible and forehead were against the jaw bracket and the forehead bracket, respectively.The aiming frame was aligned between the pupil and the lower eyelid margin; the position was adjusted until the reflection of the lower eyelashes was clear.Patients were asked to gaze at the light source for approximately 20s and blink normally.The average LLT and PBR were recorded.The C-factor (CF) was calculated as an index of reliability, and the measurements were repeated when CF<0.7 (Figure 1C).
Cleaning, Hot Compresses and Massage of the Meibomian GlandGroup B used a steam eye mask (Your Ga Run Fang,Shang Hai Run Mu Industrial Co., Ltd., China) for 20min 3d before surgery.Sterile cotton swabs were used to apply physiological saline to the eyelid for local cleaning, and the secretions and phosphorus debris on the surface of the eyelid margin were removed to fully expose the meibomian gland.After surface anaesthesia with 0.1% lidocaine eye drops (Alcon,USA), the eyelid margin was disinfected, and the eyelid was opened.Meibomian gland tweezers were used to squeeze from the root of the gland toward the opening to expel the secretions; each gland was expressed twice.A sterilized cotton swab with a small amount of normal saline was swept along the roots of the eyelashes from the inner canthus to the outer canthus.The conjunctival sac was rinsed with normal saline to dislodge any attached bacteria that may have been present in the secretions.After the operation, an appropriate amount of gatifloxacin cream (Shen Yang Xing Qi Pharmaceutical Co.,Ltd., China) was applied to the conjunctival sac to prevent infection.Hot towels (40℃) were applied to the eyes for 10min every morning and evening for 3d before the operation.Surgical MethodsAll operations were performed by the same experienced surgeon, who specialized in ocular fundus surgery.Disinfectant was routinely applied with a cloth, and the eyelids were retracted with an eyelid speculum.After satisfactory retrobulbar anaesthesia was established, conventional phacoemulsification was performed.A 25G three-channel vitrectomy instrument (Alcon, Constellation Ⅴitrectomy System) was applied to the pars plana 3.5 mm posterior to the corneal limbus.The three channels were oriented in the superior nasal, superior temporal and inferior temporal directions, respectively.The non-contact Resight fundus imaging system was used for surgery.During the operation,fundus laser irradiation, injection of inert gas or silicone oil fillers, fundus membrane stripping,etc., could be carried out according to the situation.After fundus treatment, a foldable intraocular lens was implanted into the capsule.The puncture cannula was pulled out, and the scleral and conjunctival punctures were closed by massage with cotton swabs.After the operation, tobramycin dexamethasone eye ointment was placed into the conjunctival sac, and a gauze dressing was kept over the eye.On the second day, the gauze was removed, normal saline was used to flush the eyes, and a postoperative course of eye medicine was started.Patients were instructed not to apply pressure to their eyes after surgery.
Eye MedicationGroup A received gatifloxacin eye drops(Otsuka Pharmaceutical Co., Ltd., Japan) 4 times daily and gatifloxacin eye ointment once every night (Shenyang Xing Qi Pharmaceutical Co., Ltd., China) for 3d before surgery.Postoperatively, gatifloxacin eye drops were administered 4 times daily, 0.1% fluorometholone (San Tian Pharmaceutical Co., Ltd., China) was administered 4 times daily, and pranoprofen (Qian Su Pharmaceutical Co., Ltd., Japan) was administered 4 times daily.The doses of the above three drugs were reduced each week.The compound tropicamide was administered once a day (Shentian Pharmaceutical Co., Ltd.,China).All of the above procedures were stopped 1mo after surgery.In addition to these drugs, Group B was given 0.1%sodium hyaluronate eye drops 4 times daily for 3d before surgery (Jiang Xi, Zhen Shiming Pharmaceutical Co., Ltd.,China) and 3mo after surgery.
Statistical AnalysisSPSS software was used to analyse the gender composition ratio and eye type of the patients using theχ2test.Normally distributed pre- and post-treatment data are expressed as the mean±standard error.Data with skewed distributions are expressed as the median (M) and the first and third quartiles (P25-P75).Repeated measures analysis of variance was used for intra-group and inter-group change trends, and Tukey’s least significant difference (LSD) was used as a post hoc test.Data were statistically analysed by independent-samplettests or Mann-WhitneyUtests for comparisons between groups.P<0.05 was considered statistically significant.
RESULTS
Basic InformationAll 60 patients completed surgery.Three patients underwent a second operation within 2mo after surgery, and 2 patients underwent conjunctival suturing during surgery.Fifteen patients were lost to follow-up due to restrictions imposed in response to the coronavirus disease 2019.All of the above patients were removed from the group.The rest of 40 patients who completed follow-up comprised 20 patients in the control group (group A) and 20 in the treatment group (group B).Among the 20 patients in group A,there were 8 cases of epiretinal membrane (ERM), 3 cases of malignant hypertension (MHT), 1 case of vitreous hemorrhage(ⅤH) with polypoid choroidal vasculopathy (PCⅤ), 1 case of ⅤH with proliferative diabetic retinopathy (PDR), 1 case of ⅤH with branch retinal vein occlusion (BRⅤO), 5 cases of rhegmatogenous retinal detachment (RRD), and 1 case of vitreous macular traction (ⅤMT).Among the 20 patients in group B, there were 3 cases of ERM, 4 cases of MH, 5 cases of RRD, 3 cases of ⅤH with PDR, 3 cases of ⅤH with BRⅤO,1 case of ⅤH with peripheral retinal phlebitis (Eales’disease),and 1 case of ⅤMT.None of the patients previously underwent eye surgery.We hope to reduce data errors by excluding patients who had multiple surgeries before and after operation.The preoperative details of the two groups are shown in Table 1.The measurements of each observation index at each timepoint are shown in Table 2.
Changes in NITBUTav and NITBUTfThere was no statistically significant difference in preoperative NITBUT between the two groups (P>0.05).The NITBUTav of group A was significantly lower than that of group B at 1wk, 1 and 3mo after surgery, and these differences were statistically significant(P<0.05; Table 3).The NITBUTav of group A decreased significantly 1wk after surgery compared with the preoperative value (P=0.007), recovered to the preoperative level 1mo after surgery (P=0.890), and remained unchanged at the last followup 3mo after surgery (P=0.417).The NITBUTav of group Bshowed no significant change 1wk after surgery compared with the preoperative value (P=0.764) and maintained a slow upwards trend 1 and 3mo after surgery (P=0.012, 0.000).The change trend of NITBUTf was similar to that of NITBUTav.Preoperative and postoperative changes in NITBUTav and NITBUTf in group A and group B are shown in Figure 2.
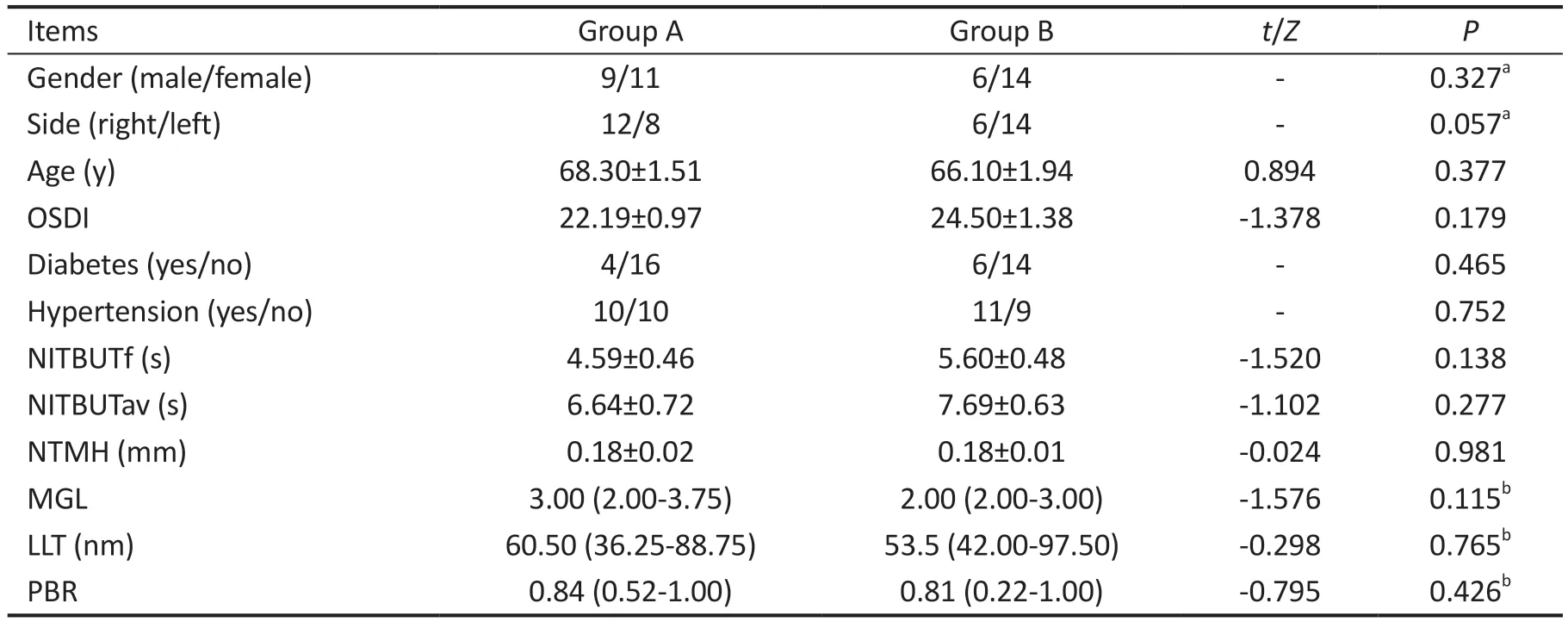
Table 1 Baseline data of the 40 patients who completed follow-up mean±SEM

Table 2 Repeated-measures analysis of variance of various indicators
Changes in NTMHThere was no significant difference in preoperative NTMH between the 2 groups (P>0.05).The NTMH of group A was significantly lower than that of group B 1wk and 1mo after surgery (P=0.008 andP<0.001,respectively), and the NTMH values of the two groups tended to be consistent 3mo after surgery (t=-1.516,P=0.138)(Table 4).There was no significant difference between the preoperative and postoperative NTMH measurements of group A, while the NTMH of group B was significantly higher 3mo after surgery than before surgery (P=0.010).
Changes in MGL scoresThe MGL scores of group A before surgery and 1wk, 1 and 3mo after surgery were 3.00 (2.00-3.75), 3.00 (2.00-3.75), 3.00 (2.30-3.75), and 3.00 (2.00-3.75), respectively.The MGL scores of group B before surgery and 1wk, 1 and 3mo after surgery were 2.00 (2.00-3.00), 3.00 (2.00-3.00), 3.00 (2.00-3.00), and 2.50 (2.00-3.00),respectively.There were no statistically significant differences in MGL scores between the two groups before surgery or 1wk,1 or 3mo after surgery (P=0.115, 0.257, 0.088, and 0.102,respectively).Additionally, there was no significant difference in MGL between the preoperative and 1-week, 1-month or 3-month postoperative values in either group (P>0.05).
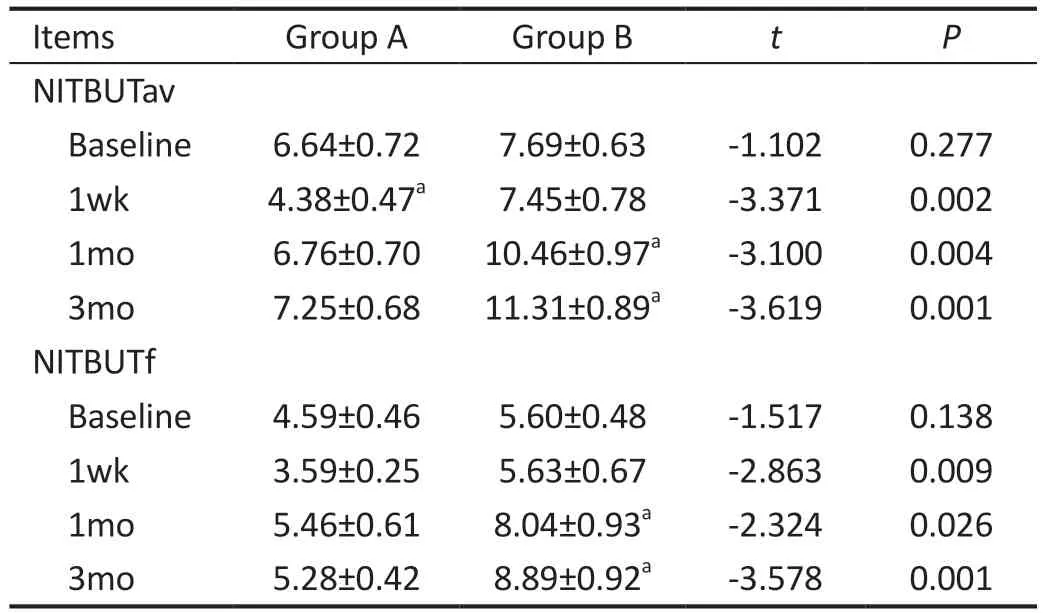
Table 3 Comparison of NITBUT between groups A and B mean±SEM, s
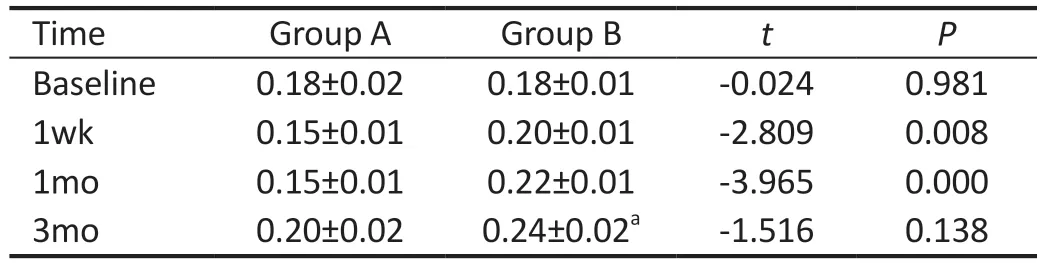
Table 4 Change in NTMH between group A and group B mean±SEM, mm

Figure 2 Comparisons of the changes in all observation indexes before and after the operation A: Control group; B: Treatment group.aP<0.05,bP<0.01, cP<0.001.NITBUTav: Average non-invasive tear film break-up time; NITBUTf: First non-invasively measured tear film break-up time;NTMH: Non-invasive tear meniscus height; MGL: Meibomian gland loss; LLT: Lipid layer thickness; PBR: Partial blink rate.
Changes in LLTThere were no significant differences between the two groups preoperatively, 1wk postoperatively,or 1mo postoperatively (P>0.05; Table 5).The LLT of group A was significantly lower than that of group B 3mo after surgery(Z=-2.379,P=0.017).There was no significant change in LLT at 1wk, 1 or 3mo after surgery in group A and no significant change in LLT at 1wk or 1mo after surgery in group B, but the LLT of group B was increased at 3mo after surgery (P<0.001).
Changes in the Partial Blink RateThere was no significant difference in PBR between the 2 groups before surgery or 1wk, 1mo, or 3mo after surgery (P=0.426, 0.606, 0.115, and 0.428, respectively) [group A: baseline 0.84 (0.52-1.00), 1wk 0.71 (0.50-1.00), 1mo 1.00 (0.71-1.00), 3mo 0.59 (0.50-0.85);group B: baseline 0.81 (0.22-1.00), 1wk 0.80 (0.53-1.00), 1mo 0.86 (0.24-1.00), 3mo 0.62 (0.00-0.92)].
There was no significant difference in PBR between the preoperative and 1-week, 1-month or 3-month postoperative values in either group (P>0.05).The preoperative and postoperative ocular parameters of the two groups are shown in Figure 2.
Local and Systemic ComplicationsDuring the treatment,the incidence of adverse reactions before and after surgery in the two groups was observed and recorded.One patient in group A developed conjunctivitis three days after surgery.Fluorometholone (0.1%) was replaced with prednisoloneacetate eye drops (Allergan Ireland Pharmaceuticals);prednisolone was discontinued onewk later, and 0.1%fluorometholone was provided again.One patient complained of dry eye during follow-up 3mo after the operation, and local sodium hyaluronate treatment was given to two patients in group B, who had a small amount of recurrent vitreous haemorrhage.The standard oral drug regimen was provided during follow-up.During the follow-up period, some patients had mild subconjunctival bleeding one day after surgery,specifically, limited bleeding at the site where the sclera had been punctured during surgery; the bleeding required no special treatment and was resolved within 1wk after surgery.The remaining patients did not have severe local bleeding,low intraocular pressure, endophthalmitis, high intraocular pressure, iatrogenic hiatus or other complications, such as a need for secondary surgery.
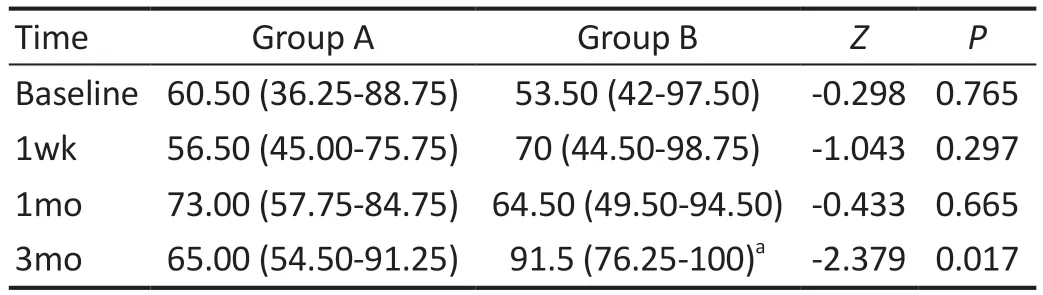
Table 5 LLT changes in groups A and B M (Q1, Q3), nm
DISCUSSION
Our study suggested that the trend of postoperative dry eye in MGD patients was aggravated in the short term and returned to the preoperative level one month after surgery.However,supplementation with artificial tears and a regimen of cleaning,hot compresses and massage applied to the meibomian gland can facilitate the rapid reconstruction of the tear film stability.The NITBUTav and NITBUTf of group A were lower than those of group B at 1wk, 1 and 3mo after surgery.Compared with the preoperative value, the NITBUT of group A decreased significantly one week after surgery, indicating that the stability of the tear film decreased after surgery and returned to the preoperative level at one month.In group B,the NITBUT continued to increase slowly until 3mo after surgery, indicating that tear film stability gradually improved.Tear break-up time (TBUT) and the Schirmer I test are still the most commonly used detection methods at present, and their repeatability is recognized in normal healthy people, but there are controversies regarding their use in patients with dry eye[11].NITBUTav and NITBUTf measurements made using the K5M have higher true positive rates, higher specificity, and lower false positive rates than ordinary TBUT measurements[17-18].
In this experiment, the NTMH of group A was significantly lower than that of group B one week and 1mo after surgery;however, the two groups were consistent 3mo after surgery.There was no significant change from the preoperative value in group A, but there was a significant increase from preoperative to postoperative in group B.It can be seen that the tear river in group B was improved slowly in the short term compared with group A.NTMH reductions mainly reflect dry eye resulting from insufficient tear production; therefore, NTMH is not a specific index of meibomian gland function.However, the effectiveness of the treatment is still evident.
In this study, group A showed no significant changes in the MGL between the preoperative and postoperative timepoints.We consider MGL to be the morphological manifestation of long-term development of meibomian gland blockage, but this variable is relatively stable in the short term.Therefore,in line with previous reports in the literature, our short-term observation did not show significant changes.The MGL of group B was not significantly improved compared with its preoperative value.It was speculated that although the patients had received preoperative nursing care for the meibomian glands, the short duration of the treatment course compromised its efficacy.Additionally, it is possible that unblocking the meibomian glands is not sufficient to reverse existing loss or atrophy of the gland structure.
The LLT mainly reflects the secretory function of the meibomian glands.The LLT of group B was significantly higher than that of group A 3mo after surgery and was also significantly higher than the preoperative value, indicating that meibomian gland secretion slowly improved.The literature has reported a downturn in LLT after cataract surgery[19-20],but there was no statistically significant decline in our group A.We speculate that the discrepancy was related to the antiinflammatory effect of low-concentration steroids and other anti-inflammatory drugs in both groups.Although the main purpose of these drugs was to suppress the inflammatory response after surgery, the relationship between MGD and inflammation also has the support of numerous studies in the literature[2,21].Therefore, an improvement in meibomian gland function as a result of local anti‐inflammatory drugs cannot be ruled out.
In addition, blinking can increase the thickness of the lipid layer on the ocular surface, and incomplete blinking can cause decreased thickness and uneven distribution of the lipid layer,leading to MGD dry eye[22].Neither of the two groups showed any difference after surgery, but the relatively high PBRs in both groups suggested that dry eye in these patients might be related to poor blinking habits in ordinary life.
In MGD, blockage of secretions in the duct can lead to obstruction,inflammation and atrophy of the entire gland, as well as decreased integrity of the lipid layer, resulting in excessive tear evaporation and decreased tear film stability.Hyperosmolar tears and inflammatory responses follow, along with further epithelial damage, goblet cell loss and disordered mucin expression.This exacerbates pre‐existing tear film instability and water evaporation, perpetuating the vicious cycle of dry eye[23-24].Inflammation plays a very important role in MGD; thus,incidental treatment of MGD as a by-product of postoperative antibiotics and hormone eye drops (used for 1mo) was inevitable.For safety reasons, we could not set up a group without postoperative anti‐inflammatory drugs as a comparison.
Ⅰn this study, we found that the decrease in tear film stability after phacovitrectomy was related to the following factors.Although a minimally invasive vitrectomy system was used to shorten the surgical time compared with previous procedures,long-term corneal exposure and tear film evaporation were relatively enhanced.Intraoperative scraping injury of the corneal epithelium may occur, and repeated liquid flushing may lead to a decrease in microvilli and microfolds in corneal epithelium, affecting the adhesion function of the hydrated mucin layer in tear film stability.The light of the microscope could also cause intraoperative injury.Silicone oil in the vitreous could enter the anterior chamber and damage corneal endothelial cells, causing subconjunctival damage to conjunctival goblet cells, while conjunctival incision also damaged goblet cells, affected mucin secretion and decreased adhesion function.
Ⅴitrectomy and cataract surgery can damage the corneal nerve,decrease light transmission through the cornea, reduce reflex secretion of tears, reduce blinking, and prolong exposure time, leading to excessive evaporation.Of course, eye drops containing benzalkonium chlorine ammonia have direct toxic effects on corneal cells when used as a postoperative disinfectant.In addition, many surgeons have the supplies and expertise for only a limited range of medical and surgical options and have no alternative to bandage contact lenses for postoperative healing; these lenses can easily harm the corneal epithelium.Other procedures, including intraoperative corneal epithelial debridement to create a clear visual field, can also cause damage to corneal tissue.In addition, intraoperative corneal or conjunctival sutures damage local tissues, resulting in conjunctiva oedema and congestion.The secretion of mucin was affected, the adhesion function decreased, and the stability of the tear film decreased.Postoperative high intraocular pressure corneal oedema followed by regular corneal changes affects tear film stability.To control variables, a 25G cutting system was used in our surgery to avoid conjunctival incision and conjunctival suturing, and a Resight fundus imaging system was used to reduce the chance of contact with the cornea.We excluded cases with intraoperative epithelial scraping, corneal or conjunctival sutures and abnormal 1-week intraocular pressure.
The lipids inside a blocked meibomian gland are sticky and have an elevated melting point.Local heat was applied at about 40°C[25], a temperature, above the melting point to soften secretions impacted in the ducts.After mechanical massage, the blockage at the eyelid margin was removed,and the lipid secretions of the meibomian gland were able to flow more freely.As a result, tear film stability increased,NITBUT was extended, and LLT increased.Sodium hyaluronate is the main component of artificial tears, which reduce the osmotic pressure of tears by diluting inflammatory substances and prolonging the NⅠTBUT.Continuous artificial tear supplementation helps to improve the ocular surface microenvironment.In addition, the anti-inflammatory effect of a routine postoperative anti-inflammatory drug regimen should not be ignored.The optimization of postoperative living habits can also have a noticeable effect on dry eye: reducing the use of video displays and scheduling adequate sleep or rest help alleviate dry eye symptoms[26-27], as does the reduction of exposure to UⅤ[28]and kitchen smoke.
This study is innovative in that we focus on the changes in patients’ocular surface after vitrectomy and propose that surgery has an impact on the ocular surface, whereas most physicians focus only on fundus recovery.In addition, we confirmed the short-term negative effects of surgery on tear film stability by using two new dry eye detection instruments,the K5M non‐contact ocular surface analyser and the LipiⅤiew interferometer.Additionally, effective treatment was provided before and after surgery, including preoperative hot compresses and meibomian gland massage as well as preoperative and postoperative artificial tear supplementation, providing double protection for the eye surface in MGD patients and producing objective clinical improvement, which is rare in current studies.
The present study still had some shortcomings in that this prospective trial had an insufficient sample size and a short observation time.Besides, on the basis that cataract and fundus disease greatly affect the visual acuity of patients, most patients tended to ignore the symptoms of dry eye, and their visual function was unstable in the short term after surgery,so we did not carry out continuous OSDI score follow-up for patients.In consideration of postoperative safety, we did not include invasive Schirmer test as criteria.As we know, diabetes can affect ocular surface and cause or aggravate dry eye as an independent risk factor[29], which may affect metrical data.
Among the patients included in our study, diabetic accounted for an indispensable part, so we did not exclude it.And we did a comparison between the two groups and there was no significant difference.Finally, it seems that anterior segment ophthalmic computed tomography, Scheimpflug analysis,tear film osmolarity orin vivoconfocal microscopy,etc.[30],can help us observe more morphological features, but it is unavailable now.These weaknesses may have introduced bias in the analysis of ocular surface changes before and after surgery or the differences between preoperative and postoperative treatment.
Despite these drawbacks, we obtained convincing evidence that phacovitrectomy reduced tear film stability in the short term and aggravated dry eye in patients with mild to moderate MGD dry eye; preoperative levels were mostly restored one month after surgery.Preoperative meibomian gland cleaning,hot compresses and massage as well as postoperative artificial tear supplementation can effectively relieve postoperative dry eye, maintain tear film stability, improve the microenvironment of the eye surface, and increase tear film duration and lipid layer thickness.Furthermore, these precautions are clinically feasible for both doctors and patients.If conditions permit,we will improve the relevant details to get more in-depth and accurate results in future.
ACKNOWLEDGEMENTS
Foundations:Supported by the Natural Science Foundation of Tianjin City (No.20JCZXJC00040); Tianjin Key Medical Discipline (No.Specialty) Construction Project (No.TJYXZDXK-037A); The Science & Technology Development Fund of Tianjin Education Commission for Higher Education(No.2022ZD058).
Conflicts of Interest: Liu BS,None;Wei JT,None;Nie ZT,None;Yang M, None;Pang SF, None;Li WB, None;Li XR,None;Hu BJ, None.
 International Journal of Ophthalmology2023年5期
International Journal of Ophthalmology2023年5期
- International Journal of Ophthalmology的其它文章
- Analysis of retinal arteriolar and venular parameters in primary open angle glaucoma
- ldentification and functional analyses of a novel FOXL2 pathogenic variant causing blepharophimosis, ptosis,and epicanthus inversus syndrome
- Protective effects of ferulic acid against ionizing radiation-induced oxidative damage in rat lens through activating Nrf2 signal pathway
- Novel homozygous ADAMTS17 missense variant in Weill-Marchesani syndrome
- Cost analysis of childhood glaucoma surgeries using the US Medicaire allowable costs
- Predicting the prognosis of primary orbital lymphoma by clinical characteristics and imaging features