
肝移植术后重度高乳酸血症影响因素分析
2023-04-29 15:17赵金鑫ImranMuhammad李新强朱存乐王承钰王峰徐庆国蔡金贞
精准医学杂志 2023年5期
赵金鑫 Imran Muhammad 李新强 朱存乐 王承钰 王峰 徐庆国 蔡金贞
[摘要] 目的 分析肝移植术后重度高乳酸血症的危险因素,为临床采取有效预防措施提供依据。方法 回顾性分析2021年1—12月于我院行肝移植手术的120例患者的临床资料,根据其术后动脉血乳酸(LAC)值分为重度高乳酸血症组与非重度高乳酸血症组。绘制趋势折线图分析所有患者围术期血生化指标与动脉血LAC水平的关系,采用χ2检验、t检验、非参数检验及多因素logistic回归模型分析上述指标对肝移植术后重度高乳酸血症的影响。结果 趋势折线图显示,所有患者手术前3 d至手术后第3天的血清谷丙转氨酶水平、谷草转氨酶水平、白蛋白水平及血浆国际标准化比值、凝血酶原时间随时间变化的趋势与动脉血LAC变化一致。單因素分析结果显示,两组患者的原发病构成比、术中无肝期时间、术中总入量、术中出血量、术中输注红细胞量比较均差异有显著性(χ2=10.579,U=-2.811~-2.183,P<0.05)。多因素logistic回归分析显示,术中无肝期时间延长和术中输注红细胞量增多为肝移植患者术后重度高乳酸血症的独立危险因素(P<0.05)。结论 肝移植术中无肝期时间延长及术中输注红细胞量增多是肝移植术后重度高乳酸血症的独立危险因素。
[关键词] 肝移植;高乳酸血症;再灌注;红细胞输注;脂肪肝;危险因素
[中图分类号] R617
[文献标志码] A
INFLUENCING FACTORS FOR SEVERE HYPERLACTACIDEMIA AFTER LIVER TRANSPLANTATION\ ZHAO Jinxin, Imran Muhammad, LI Xinqiang, ZHU Cunle, WANG Chengyu, WANG Feng, XU Qingguo, CAI Jinzhen (Organ Transplantation Center, The Affiliated Hospital of Qingdao University, Qingdao 266100, China)
[ABSTRACT] Objective To investigate the risk factors for severe hyperlactacidemia after liver transplantation, and to provide a basis for adopting effective preventative strategies in clinical practice. Methods A retrospective analysis was performed for the clinical data of 120 patients who underwent liver transplantation in our hospital from January to December, 2021, and according to the value of arterial lactic acid (LAC) after surgery, they were divided into severe hyperlactacidemia group and non-severe hyperlactacidemia group. The trend line chart was plotted to analyze the association between blood biochemical parameters and arterial LAC level in the perioperative period; the chi-square test, the t-test, the non-parametric test, and the multivariate logistic regression model analysis were used to investigate the effect of the above indicators on severe hyperlactacidemia after liver transplantation. Results The trend line chart showed that in all patients, the changing trend of serum alanine aminotransferase, serum aspartate aminotransferase, serum albumin, plasma international normalized ratio, and prothrombin time was consistent with that of arterial LAC level from day 3 before surgery to day 3 after surgery. The univariate analysis showed that there were significant differences between the two groups in the constituent ratio of primary disease, duration of anhepatic phase during surgery, total intraoperative intake, intraoperative blood loss, and intraoperative red blood cell transfusion (χ2=10.579,U=-2.811--2.183,P<0.05). The multivariate logistic regression analysis showed that prolonged duration of anhepatic phase during surgery and increased intraoperative red blood cell transfusion were independent risk factors for severe hyperlactacidemia after liver transplantation (P<0.05). Conclusion The prolonging duration of anhepatic phase during surgery and increasing intraoperative red blood cell transfusion are independent risk factors for severe hyperlactacidemia after liver transplantation.
[KEY WORDS] Liver transplantation; Hyperlactatemia; Reperfusion; Erythrocyte transfusion; Fatty liver; Risk factors
研究显示,目前全球成人肝移植术后1年生存率达96%,10年生存率达71%[1-2],肝移植术已成为终末期肝病、急性暴发性肝衰竭、肝细胞癌、肝门胆管癌和多种代谢性疾病最有效的治疗方法。肝移植手术中最重要的步骤是病肝摘除和供肝植入,这一过程中患者的下腔静脉及门静脉将被阻断,由于门静脉高压症、肝硬化心肌病、手术出血和再灌注综合征等因素影响,患者血流动力学不稳定的情况经常发生,可导致机体主要器官灌注不足,造成体内代谢产物的堆积,其中动脉血乳酸(LAC)堆积造成的高乳酸血症对患者预后可产生严重影响。已有的研究发现,较高的LAC水平是导致移植术后患者死亡的重要因素之一[3]。CHEONG等[4]的研究通过分析2008年1月—2019年2月间韩国肝移植登记的2 002例患者,发现移植术前高乳酸血症是影响肝移植患者术后生存率的危险因素,且与循环衰竭和呼吸衰竭的发生均相关。本研究探究肝移植术后重度高乳酸血症的危险因素,旨在为肝移植术后重度高乳酸血症预防及治疗的临床决策提供依据。
1 资料和方法
1.1 一般资料
本研究回顾性分析2021年1—12月于我院器官移植中心行肝移植手术治疗的120例患者的临床资料。患者纳入标准:①年龄≥18岁者;②术前有完善的血常规、电解质、肝肾功能、血凝常规、血气分析等检查者。排除标准:①术中及术后临床指标监测不完整或其他所需临床资料不完整者;②多器官联合移植者。依据患者移植术后动脉血LAC水平是否≥5 mmol/L[4],将所有的患者分为重度高乳酸血症组(LAC≥5 mmol/L)与非重度高乳酸血症组(LAC<5 mmol/L)。
收集两组患者的临床资料,包括年龄、性别、体质量指数(BMI)、原发病、MELD评分、Child评分及分级、手术方式、并发症(是否合并肝性脑病、腹水、消化道出血等),收集患者围手术期(手术前3 d、手术开始时、术中阻断门静脉前、术中开放门静脉后、术后入ICU时及术后第1、2、3天)的全血血红蛋白(HB)、血清谷丙转氨酶(ALT)、血清谷草转氨酶(AST)、血清总胆红素(TB)、血清白蛋白(ALB)、血清肌酐(CR)水平及血浆凝血酶原时间(PT)、血浆国际标准化比值(INR)、动脉血LAC水平、动脉血pH值,同时收集患者手术时间、术中受体是否缺血预处理、术中无肝期时间、术中冷缺血时间、术中总入量、术中输注红细胞量、术中出血量、术中尿量,并收集患者移植物質量与受体体质量比(GRWR)及供肝病理检查结果(供肝弹性值、脂肪肝程度)。
1.2 统计学方法
采用SPSS 26.0统计软件对数据进行统计学分析处理。正态分布的计量资料以x?±s表示,组间比较采用独立样本t检验;偏态分布的计量资料采用M(P25,P75)表示,组间比较采用非参数检验;定性资料以例(率)表示,组间比较采用χ2检验;多因素分析使用logistic回归模型,自变量采用强制进入法。以P<0.05为差异有统计学意义。
2 结果
2.1 所有患者围术期动脉血LAC水平与血清中ALT、AST、ALB及血浆中INR、PT水平变化趋势间的关系
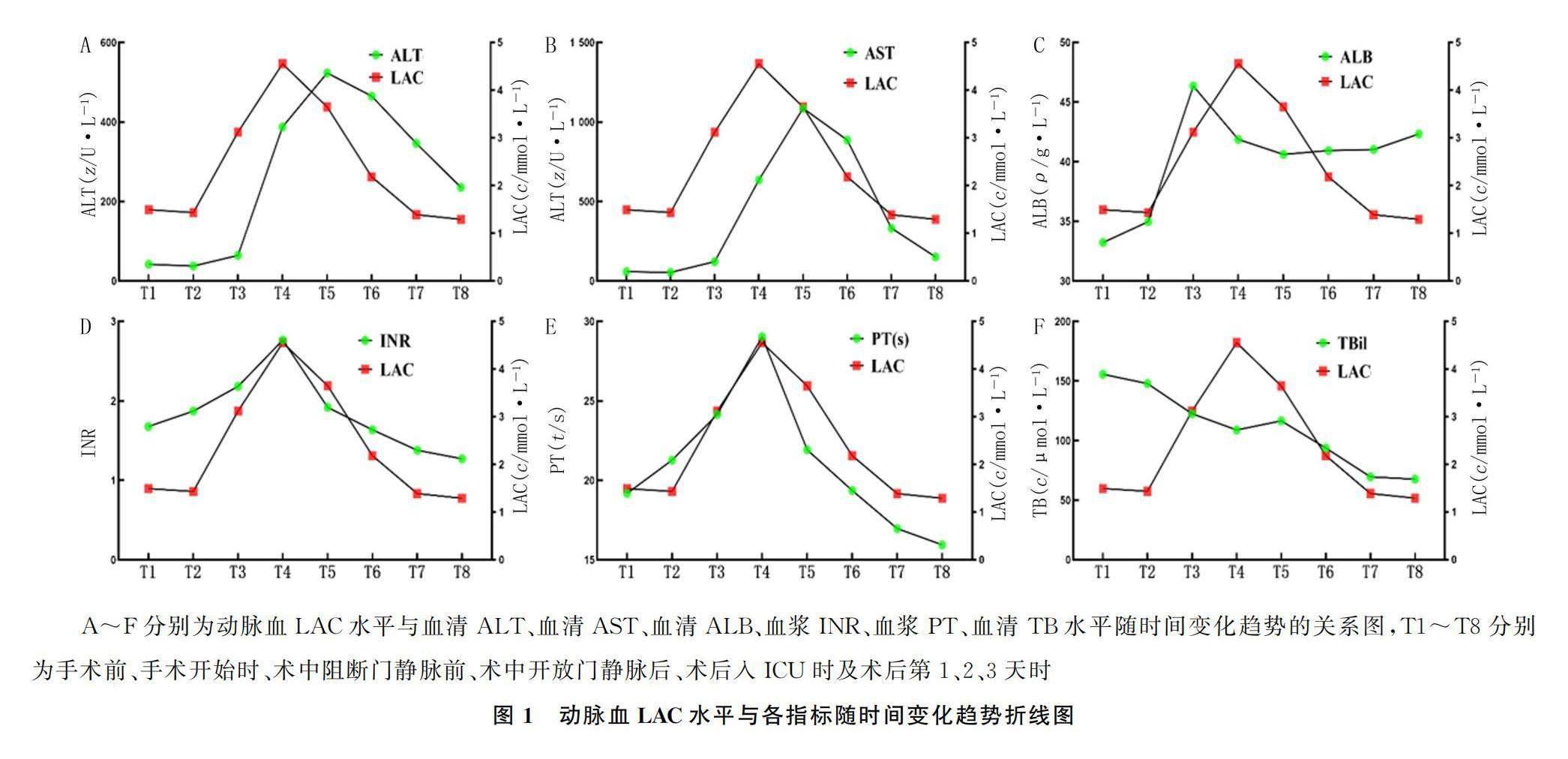
折线图显示LAC水平在手术开始后逐渐升高,在开放门静脉后达到峰值,随后逐渐下降。血清ALT、AST、ALB及血浆INR、PT水平在术中变化趋势与LAC水平一致,血清ALT、AST水平在患者术后入ICU时达到峰值,略晚于LAC达峰时间,血清TB与动脉血LAC水平变化趋势未见明显一致。见图1。
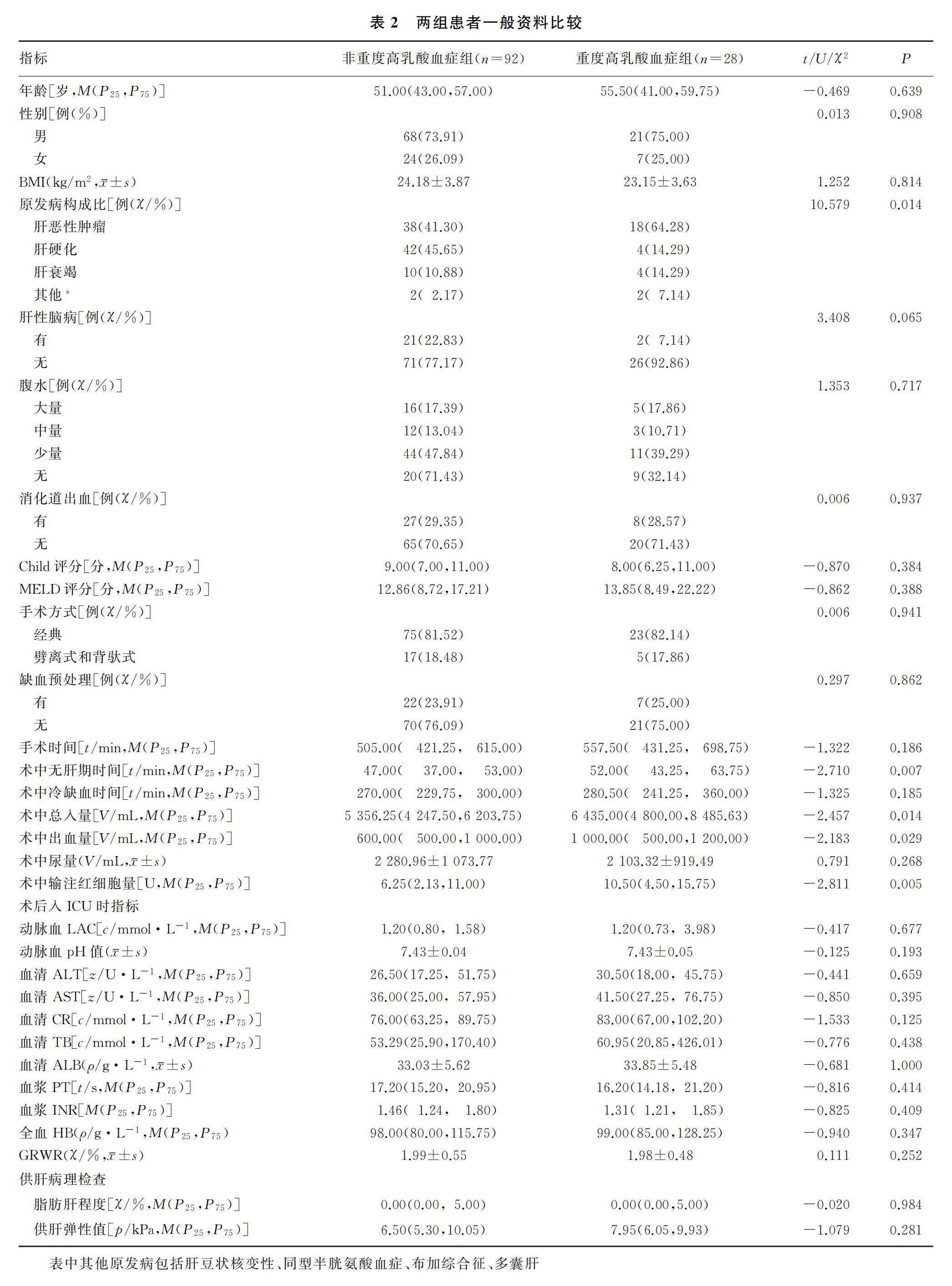
2.2 两组患者一般资料比较
两组患者原发病构成比、术中无肝期时间、术中总入量、术中出血量、术中输注红细胞量均差异具有显著(χ2=10.579,U=-2.811~-2.183,P<0.05)。见表2。
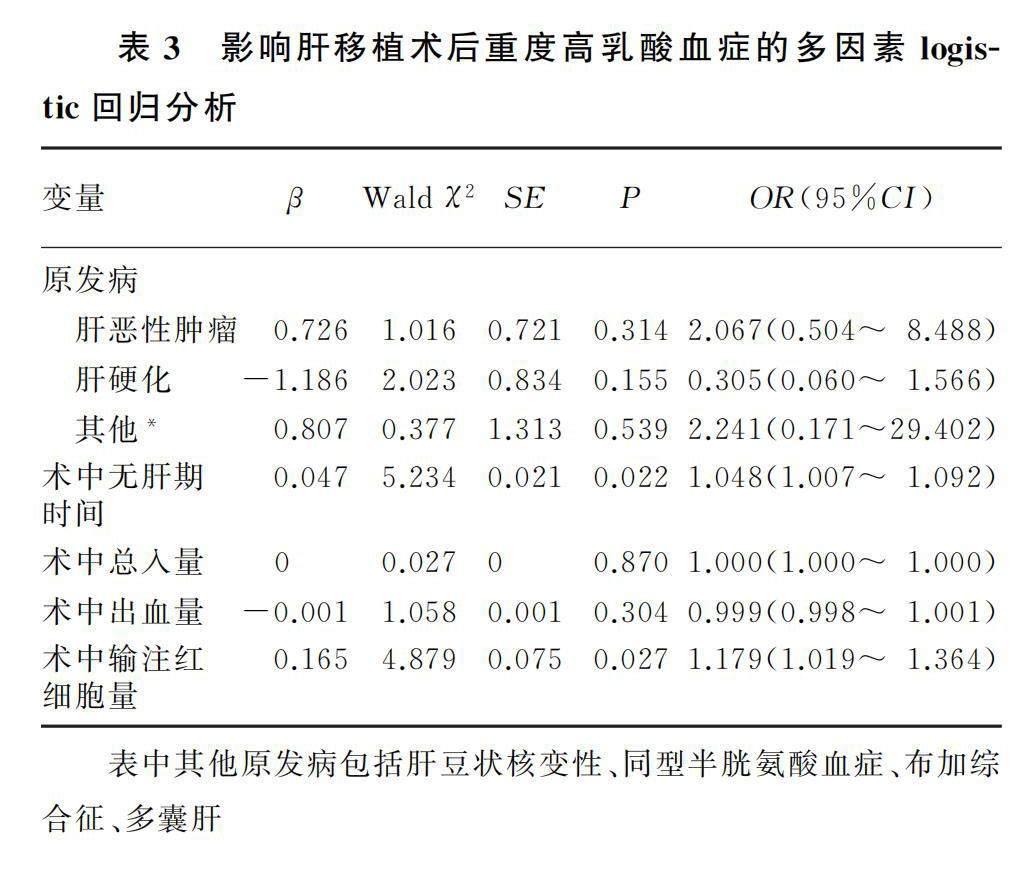
2.3 影响肝移植术后重度高乳酸血症的多因素logistic回归分析
将单因素分析中P<0.05的因素作为自变量进
A~F分别为动脉血LAC水平与血清ALT、血清AST、血清ALB、血浆INR、血浆PT、血清TB水平随时间变化趋势的关系图,T1~T8分别为手术前、手术开始时、术中阻断门静脉前、术中开放门静脉后、术后入ICU时及术后第1、2、3天时行多因素logistic回归分析,原发病统计中以肝衰竭为参照。多因素logistic回归分析显示,术中无肝期时间延长和术中输注红细胞量增多为肝移植术后重度高乳酸血症的独立危险因素(P<0.05)。见表3。
3 讨论
高乳酸血症或乳酸酸中毒与肝移植术后早期肝功能不全有关[5]。人体中LAC大部分经过肝脏代谢,小部分经肾脏代谢。肝移植术中无肝期静脉氧饱和度降低会导致移植术后急性肾损伤[6],LAC两大代谢途径在无肝期均受影响,导致LAC在体内聚集。本研究结果显示,动脉血LAC在无肝期结束后达到峰值,在手术结束入ICU时,所有患者血清ALT、AST达到峰值,其达峰时间略晚于LAC达峰时间,但动态变化趋势与动脉血LAC水平较为一致。某些肿瘤也可导致高乳酸血症[7-8]。有研究结果表明,恶性肿瘤不仅可以通过无氧葡萄糖代谢途径产生LAC,而且还可以通过有氧糖酵解途径产生LAC,以提供适合肿瘤生长的微环境,该过程称为WARBURG效应[9]。在本研究中,术后发生重度高乳酸血症的患者原发病为恶性肿瘤的占比达到了64.28%,但其是否与肝脏恶性肿瘤的葡萄糖代谢及LAC代谢状态改变有关,需要进一步的研究论证。
术中无肝期时间是评价肝移植手术质量的重要指标。有研究显示,无肝期超过100 min的肝移植患者,移植物功能障碍发生率较高[10];另外,过长的无肝期时间也是肝移植术后胆道并发症及术后大量腹水的独立危险因素[11-12]。本研究结果显示,过长的无肝期时间会增加肝移植患者术后重度高乳酸血症的可能。MIYAMOTO等[13]回顾性分析了190例接受肝移植的成年(>16岁)患者的临床资料,发现背驮式肝移植较经典原位肝移植温缺血时间均显著缩短。因此,采用背驮式手术方式可能会缩短无肝期的时间,减少术后重度高乳酸血症的发生。本研究中采用背驮式手术的病例较少,且在分组中将其与劈离式手术方式合并,未发现不同手术方式间重度高乳酸血症发生的差异;在未来的研究中我们需要更详细的分组,以证明不同手术方式是否会对移植术后重度高乳酸血症的发生产生影响。
肝移植术中大量输血作为移植术后患者死亡的重要危险因素已经被大量研究证实[14-15]。既往研究表明,不仅是术中输血量,肝移植术后48 h内输注红细胞≥10 U也会导致移植术后30 d病死率升高,且使患者术后肺部感染、腹腔出血、胸腔积液、急性肾损伤等并发症发生率升高[16]。有研究表明,无输血肝移植术后第7天的血清ALT水平更低,提示无输血肝移植有利于移植肝功能恢复[17]。本研究结果显示,肝移植术后重度高乳酸血症组患者术中输注红细胞量显著高于非重度高乳酸血症组,说明肝移植术中输注红细胞量过多将增加术后重度高乳酸血症发生可能,影响患者预后。因此临床上有必要采取一些措施以减少移植术中输注红细胞量。低中心静脉压技术作为减少肝移植术中出血的关键措施目前已被广泛使用,可在降低患者术中中心静脉压的同时减少出血引起的血红蛋白损失,达到减少术中输血的目的[18],术中维持较高的每搏变异量也可以在不影响肝移植预后的情况下减少术中输血量[19]。此外,术中即时检测可实现更及时的止血和输血管理,从而更快地维持血流动力学稳定,且基于即时检测的止血治疗在肝移植中可以减少输血并改善预后[20]。有研究指出使用供肝者来源的红细胞可减少受者对其他来源浓缩红细胞的需求[21],且输注供血可在一定程度上降低移植术后血清中AST的水平[22],从而诱导受者对于同种异体肝移植的免疫耐受[23-24]。
综上所述,本研究通过对120例肝移植患者的临床资料进行回顾性分析,发现肝移植围术期动脉血LAC水平与血清ALT、AST、ALB水平及血浆INR、PT等5项指标变化趋势一致,且证实了术中无肝期时间延长和术中輸注红细胞量增多为肝移植术后患者重度高乳酸血症的独立危险因素。
伦理批准和知情同意:本研究涉及的所有试验均已通过青岛大学附属医院医学伦理委员会的审核批准(文件号QYFYWZLL27788)。所有试验过程均遵照《赫尔辛基宣言》的条例进行。受试对象或其亲属已经签署知情同意书。
作者声明:赵金鑫、王峰、徐庆国、蔡金贞参与了研究设计;赵金鑫、IMRAN MUHAMMAD、李新强、朱存乐、王承钰参与了论文的写作和修改。所有作者均阅读并同意发表该论文,且均声明不存在利益冲突。
[参考文献]
[1]ADAM R, KARAM V, DELVART V, et al. Evolution of indications and results of liver transplantation in Europe. A report from the European Liver Transplant Registry (ELTR)[J]. J Hepatol, 2012,57(3):675-688.
[2]EUROPEAN ASSOCIATION FOR THE STUDY OF THE LIVER ELECTRONIC ADDRESS: EASLOFFICE EU. EASL clinical practice guidelines: Liver transplantation[J]. J Hepatol, 2016,64(2):433-485.
[3]KIM K S, LEE S H, SANG B H, et al. Intraoperative lactic acid concentration during liver transplantation and cutoff va-lues to predict early mortality: A retrospective analysis of 3, 338 cases[J]. Anesth Pain Med, 2022,17(2):213-220.
[4]CHEONG Y, LEE S, LEE D K, et al. Preoperative hyperlactatemia and early mortality after liver transplantation: Selection of important variables using random forest survival analysis[J]. Anesth Pain Med, 2021,16(4):353-359.
[5]SILVA M A, MIRZA D F, MURPHY N, et al. Intrahepatic complement activation, sinusoidal endothelial injury, and lactic acidosis are associated with initial poor function of the liver after transplantation[J]. Transplantation, 2008,85(5):718-725.
[6]KIM W H, OH H W, YANG S M, et al. Intraoperative hemodynamic parameters and acute kidney injury after living donor liver transplantation[J]. Transplantation, 2019,103(9):1877-1886.
[7]BRANCO M, LINHARES P, CARVALHO B, et al. Serum lactate levels are associated with glioma malignancy grade[J]. Clin Neurol Neurosurg, 2019,186:105546.
[8]MAHER S A, TEMKIT M, BURAS M R, et al. Serum lactate and mortality in emergency department patients with cancer[J]. West J Emerg Med, 2018,19(5):827-833.
[9]ROMERO-GARCIA S, MORENO-ALTAMIRANO M M, PRADO-GARCIA H, et al. Lactate contribution to the tumor microenvironment: Mechanisms, effects on immune cells and therapeutic relevance[J]. Front Immunol, 2016,7:52.
[10]IJTSMA A J, VAN DER HILST C S, DE BOER M T, et al. The clinical relevance of the anhepatic phase during liver transplantation[J]. Liver Transpl, 2009,15(9):1050-1055.
[11]YUAN D, WEI Y G, LIN H M, et al. Risk factors of biliary complications following liver transplantation: Retrospective analysis of a single centre[J]. Postgrad Med J, 2009,85(1001):119-123.
[12]ITO D, AKAMATSU N, TOGASHI J, et al. Behavior and clinical impact of ascites after living donor liver transplantation: Risk factors associated with massive ascites[J]. J Hepatobiliary Pancreat Sci, 2016,23(11):688-696.
[13]MIYAMOTO S, POLAK W G, GEUKEN E, et al. Liver transplantation with preservation of the inferior vena cava. A comparison of conventional and piggyback techniques in adults[J]. Clin Transplant, 2004,18(6):686-693.
[14]JIN S J, KIM S K, CHOI S S, et al. Risk factors for intrao-perative massive transfusion in pediatric liver transplantation: A multivariate analysis[J]. Int J Med Sci, 2017,14(2):173-180.
[15]GORDON K, FIGUEIRA E R R, ROCHA-FILHO J A, et al. Perioperative blood transfusion decreases long-term survival in pediatric living donor liver transplantation[J]. World J Gast-roenterol, 2021,27(12):1161-1181.
[16]TAN L C, WEI X Z, YUE J M, et al. Impact of perioperative massive transfusion on long term outcomes of liver transplantation: A retrospective cohort study[J]. Int J Med Sci, 2021,18(16):3780-3787.
[17]田大治,滕大洪,于楊,等. 无输血肝移植的临床初步探索研究[J]. 中华外科杂志, 2021,59(5):348-352.
[18]RAMOS H C. Liver transplantation without the use of blood products[J]. Arch Surg, 1994,129(5):528.
[19]CHOI J M, LEE Y K, YOO H, et al. Relationship between stroke volume variation and blood transfusion during liver transplantation[J]. Int J Med Sci, 2016,13(3):235-239.
[20]LEON-JUSTEL A, NOVAL-PADILLO J A, ALVAREZ-RIOS A I, et al. Point-of-care haemostasis monitoring during liver transplantation reduces transfusion requirements and improves patient outcome[J]. Clin Chim Acta, 2015,446:277-283.
[21]SHAYLOR R, DESMOND F, LEE D K, et al. The impact of intraoperative donor blood on packed red blood cell transfusion during deceased donor liver transplantation: A retrospective cohort study[J]. Transplantation, 2021,105(7):1556-1563.
[22]LV T, XU X, SONG J L, et al. Use of donor-specific red blood cell transfusions for patients undergoing liver transplantation during the COVID-19 pandemic[J]. Hepatobiliary Surg Nutr, 2021,10(4):486-497.
[23]SATO Y, ICHIDA T, WATANABE H, et al. Repeating intraportal donor-specific transfusion may induce tolerance following adult living-related donor liver transplantation[J]. He-patogastroenterology, 2003,50(51):601-606.
[24]SATO Y, CHIKAKO T, OYA H, et al. Regulatory T-cell activation among patients who displayed operational tolerance following intraportal administration of donor-specific antigents in living doner liver transplantation[J]. Transplant Proc, 2012,44(2):560-564.
(本文編辑 范睿心 厉建强)
猜你喜欢
中老年保健(2022年5期)2022-11-25
中老年保健(2022年1期)2022-08-17
保健医苑(2021年7期)2021-08-13
家庭医学(下半月)(2020年7期)2020-08-24
科技资讯(2016年19期)2016-11-15
中国实用医药(2016年24期)2016-10-17
肝胆胰外科杂志(2015年5期)2015-02-27
肝博士(2015年2期)2015-02-27
河北医科大学学报(2011年12期)2011-03-25
祝您健康(1989年1期)1989-12-30
