
Screening for hypertension-mediated organ damage and aetiology: still of value after 65 years of age?
2022-12-20 09:26:24DelphineThiolliereBrahimHarbaouiClaireFalandryMarcBonnefoyJeanChristopheLegaPierreLantelmePierreYvesCourand
Journal of Geriatric Cardiology 2022年11期
Delphine Thiolliere, Brahim Harbaoui,2, Claire Falandry, Marc Bonnefoy, Jean-Christophe Lega, Pierre Lantelme,2, Pierre-Yves Courand,2,
1. Fédération de cardiologie, Hôpital de la Croix-Rousse et Hôpital Lyon Sud, Hospices Civils de Lyon, Lyon, France;2. Université de Lyon, CREATIS; CNRS UMR5220; INSERM U1044; INSA-Lyon; Université Claude Bernard Lyon,France; 3. Service Universitaire de Gériatrie, Hôpital Lyon Sud, Hospices Civils de Lyon, Lyon, France; 4. CarMeN, Université Claude Bernard Lyon 1, Oullins, France; 5. Service de médecine interne et pathologies vasculaires, Groupe d’Etude Multidisciplinaires des Maladies Thrombotiques (GEMMAT), Hôpital Lyon Sud, Hospices Civils de Lyon, Lyon,France; 6. Université de Lyon, Equipe Evaluation et Modélisation des Effets Thérapeutiques, Laboratoire de Biologie et Biométrie Evolutive, CNRS UMR 5558; Université Claude Bernard, Lyon, France.
ABSTRACT BACKGROUND Secondary forms and hypertension-mediated organ damage (HMOD) may differ between younger and older hypertensive patients. The aim of the present study was to explore the specificity of HMOD and secondary forms in patients ≥ 65 years in comparison to younger ones in a contemporary cohort. METHODS We analysed 938 patients recruited between 2004 and 2014 (Cardiology department, Croix-Rousse Hospital, Lyon)who had at baseline HMOD and secondary forms screening among them 190 were ≥ 65 years. RESULTS The mean (2.1 ± 0.8 vs. 1.2 ± 0.9, P < 0.001) and frequency of HMOD (96.3% vs. 72.9%, P < 0.001) was higher in patients ≥ 65 years than younger ones. Carotid femoral pulse wave velocity > 10 m/s was the most frequent HMOD in patients ≥ 65 years (90.1%), while echocardiographic left ventricular hypertrophy was the most common in the younger patients (45.0%).Among ECG left ventricular indexes, only R wave in aVL lead was significantly more frequently observed in patients ≥ 65 years(32.6%) than in younger ones (19.0%, P < 0.001). The frequency of secondary hypertension was not significantly different between younger and older patients (respectively; 30.5% vs. 27.8%, P = 0.487). The most frequent aetiology was primary aldosteronism regardless of age, followed by renovascular hypertension (6.3% vs. 3.3%, P = 0.038). Among older patients, 3.2% were treated with adrenalectomy and 6.3% with percutaneous transluminal renal angioplasty. CONCLUSION Extensive screening of HMOD in older patients may be questionable as nearly all patients had one; aetiology must however be explored as a third of older patients had a secondary form.
Hypertension is one of the most common diseases; it affects more than one billion patients around the world, and almost 150 million in Europe.[1]The frequency of the disease increased proportionally with the progressive aging of the population; it affects > 60% of those aged ≥ 60-years,[2]and > 90% of individuals with normal blood pressure (BP) at 55 years of age will develop hypertension.[3]The work-up of hypertension includes the detection of secondary forms and the evaluation of cardiovascular risk based on other risk factors as well as hypertension-mediated organ damage (HMOD) screening, both of which increase drastically the frequency of cardiovascular events and mortality.[1]The pathophysiology of hypertension in older patients may be explained by arterial stiffness, unpaired neurohormonal regulation (decrease of plasma aldosterone and renin levels, increase of net basal sympathetic nervous system)and an increase salt sensitivity related to aging kidneys.[4]Based on these observations, the screening of secondary hypertension in older patients may be questionable. Furthermore, certain secondary hypertension screening tests, particularly primary aldosteronism, may require a change in antihypertensive treatment to not interfere with renin-angiotensin-aldosterone system,[5]and this may transiently induce a rise in BP that could be harmful in patients receiving secondary prevention (heart failure, stroke…), a situation frequently associated in older hypertensive patients.[6]Concerning HMOD,it has been previously demonstrated that their number may increase cardiovascular mortality,[7]but are not extensively screened in clinical practice for reasons of local availability (materials or personnel) or time constraints.[8]There is no recommendation to propose a specific screening in older hypertensive patients, however we may postulate that certain HMOD should be more frequently observed than others, particularly arterial stiffness, based on the pathophysiology previously described. A more appropriate screening may be particularly interesting for decreasing the cost of evaluation in this subgroup of patients that represents the majority of hypertensive patients.
The aim of the present study was to explore the frequency of secondary forms and HMOD including their management in patients aged ≥ 65 years in comparison to younger ones in a contemporary cohort referred in tertiary centre.
METHODS
The cohort of hypertensive patients started in 1995 (cardiology department, Hôpital de la Croix-Rousse). A total 1618 patients were included up to the end of 2014 in our tertiary centre for a work-up of hypertension. In the present study, the 938 patients recruited between 2004 and 2014 with full medical records to have complete data regarding aetiology and HMOD were included and analysed several weeks after the work-up of hypertension. Patients were divided in two groups according to age:< 65 years (n= 748) and ≥ 65 years (n= 190) or according to tertiles (≤ 42 years (n= 313), 43-57 years(n= 312) and ≥ 58 years (n= 313)). These hypertensive patients visited our department for a complete work-up of their hypertension during a 2-day hospital stay. The majority of patients were not followup in our department after achievement of BP control.
Patient Management
Patient management has been described previously.[9]In most patients (n= 774, 82.5%) drugs likely to interfere with hormone regulation were withdrawn before admission (six weeks for spironolactone; two weeks for diuretics, beta-blockers, or renin-angiotensin system inhibitors) and replaced by alpha-blockers, centrally acting drugs, or calcium antagonists according to the current guidelines.[1]Over two days of hospital stay, all the participants filled out a questionnaire (morphometric characteristics, cardiovascular risk factors, symptoms, etc…),underwent a physical examination, a 24-h BP measurement (every 15 min from 6 a.m. to 10 p.m. and every 30 min from 10 p.m. to 6 a.m. performed using the Spacelabs®90207 monitor (Spacelabs Healthcare, Issaquah, WA, US), laboratory and imaging tests.
After one night in the supine position (at around 8 a.m.), plasma renin concentration (commercial immunoradiometric kit, Renin III generation; Cisbio,Codolet, France), plasma aldosterone concentration(commercial immunoradiometric kit, Immunotech;Beckman Coulter, Villepinte, France) 24-h urinary free cortisol was measured during the hospital stay(commercial immunoradiometric kit; Beckman Coulter). Patients were carefully instructed to urinate into the container during the 24-h collection period.
Lipids (total cholesterol, low-density lipoprotein(LDL) cholesterol, high-density lipoprotein (HDL)cholesterol, triglycerides), fasting glucose, haemoglobin A1c (HbA1c), and uric acid were assessed in the plasma around 8:00 am after one night of fasting.
Obstructive sleep apnoea (OSA) was screened during one night using the ApneaLinkTM(Resmed,San Diego, USA) ambulatory sleep monitor. Patients with apnoea-hypopnoea indices ≥10 were referred to a pulmonologist to perform a polysomnography if appropriate.[10]
HMOD Assessment
Heart and vessels assessment, left ventricular hypertrophy (LVH) with electrocardiogram (ECG) or left ventricular mass index (LVMI), pulse pressure and pulse wave velocity (PWV), are detailed in supplementary data.[11,12]Data for LVMI were available only in 771 patients for technical reasons (n= 167 have unassessable LVMI). ECG and pulse pressure were available in all participants (n= 938). PWV was performed in 796 patients.
To detect HMOD at the kidney level, microalbuminuria was measured on 24-h urine collection. The estimated glomerular filtration rate (eGFR) was assessed using the Modification of Diet in Renal Disease (MDRD) formula. Kidney damage was defined by either MDRD < 60 mL/min per 1.73 m2or microalbuminuria > 30 mg/day,[1]and were available in all participants (n= 938).
A total of 796 patients (n= 645, aged < 65 years;n=151, aged ≥ 65 years) had an assessment including the 3 HMOD (heart, vessels, and kidney).
1.3 排除标准 凝血功能障碍、心功能不全等不能接受穿刺者。所有患者先US-FNAC,得到满意的细胞学检查结果后手术切除,均有手术病理诊断术前签署知情同意书。
Definition of Secondary Hypertension
Primary aldosteronism was defined as follows:plasma aldosterone-to-renin ratio > 130 pmol/L per pg/mL (46.9 ng/L), plasma aldosterone > 416 pmol/L (150 ng/L), or plasma aldosterone after saline infusion >100 pmol/L (36 ng/L) when available.[13]After this diagnosis, an abdomen computedtomography (CT)-scan was performed. Adrenal venous sampling was proposed to patients who were considering adrenalectomy in case of unilateral secretion.
Hypercortisolism was defined as a 24 h-UFC above the normal range (> 250 nmol/24 h, upper value of the normal range for the assay) confirmed by a serum cortisol > 50 nmol/L after midnight administration of 1 mg dexamethasone.[14]Such patients were referred to an endocrinologist to complete the diagnosis.
Phaeochromocytoma was screened with plasma or 24-h urinary fractionated metanephrines followed if necessary by CT-scan and nuclear imaging as appropriate;[1]definite diagnosis was based on pathology.
Renovascular hypertension was defined as follows: (1) unilateral or bilateral main, branch or accessory atherosclerotic renal artery stenosis or fibromuscular dysplasia with a decrease in renal artery diameter of > 60% detected by non-invasive imaging(Doppler ultrasound or CT-scan and confirmed by invasive renal artery angiography, and (2) treated by percutaneous renal artery angioplasty with or without stenting.[15]Percutaneous renal artery angioplasty was performed after a complete analyses of Doppler ultrasound (resistive index, kidney size),CT-scan and if necessary translesional pressure gradients measurement during renal angiography.
Renal parenchymal disease was considered after analyses of albuminuria, haematuria, eGFR, and renal ultrasound. These patients were referred to a nephrologist.
Statistical Analyses
Continuous variables approximating normal distributions were summarised by mean ± SD. Continuous variables with skewed distributions were summarised by median and interquartile range[IQR]. Categorical variables were expressed as percentages. Analysis of variance (ANOVA) or nonparametric tests were used as appropriate to compare continuous variables between subgroups.χ²testing was used for between-group comparisons of dichotomous variables. Multivariate logistic regression analyses were used to demonstrate the association between secondary forms, HMOD and age independently of confounding variables (diabetes,smoking, blood pressure, eGFR, BMI and HbA1c).The analyses were performed using SPSS v20.0.0(SPSS, Chicago, IL, USA). AP-value < 0.05 was considered as statistically significant.
RESULTS
Baseline Characteristics
Half of patients were women (48.8%) and the mean age was 50.5 ± 15.2 years. BP was not controlled under antihypertensive treatment for the majority of patients. Older patients had significantly higher median BMI, higher median systolic BP, and lower median diastolic BP while they were treated with a greater number of antihypertensive treatments. They also were less frequently smokers but have more frequently secondary prevention(heart failure and coronary artery disease) and diabetes; laboratory assessments found lower mean eGFR and median plasma aldosterone, and a higher mean HbA1c (Table 1). Similar results were obtained according to tertiles of age (Table S1, supplementary data).

Table 1 Baseline patient characteristics.
HMOD
Older patients had more frequently a kidney HMOD, both albuminuria and eGFR, in comparison to younger ones. Heart screening found higher median NT-proBNP and higher proportion of anatomical and electrical LVH in older patients (a significant difference when R wave in aVL lead [RaVL]was used and a trend towards this for Sokolow-Lyon and Cornell). For vessels, older patients had also frequently increased pulse pressure and PWV. In older patients the mean number of HMOD was 2.1 ±0.8 and 96.3% of them had ≥ 1 HMOD (Table 3 and Table S3, supplementary data). The distribution of HMOD differed according to age; in younger patients the association of vessels and heart HMOD was the most frequent situation (20.5%), followed by isolated vessel HMOD (16.0%; Figure 1A); in older patients the association of 3 HMOD was the most frequent situation (37.9%), followed by the association of vessels and heart HMOD (28.4%;Figure 1B). In younger patients, the overlap between anatomical and electrical LVH was 57.7%(Figure 2A); in older patients this was 33.8%(Figure 2B). In both age groups, all patients with unknown anatomical LVH had electrical LVH(Figure 2). Kidney and vessels HMOD were independently associated with age after adjustment to major confounders (Table S4 and S5, supplementary data).
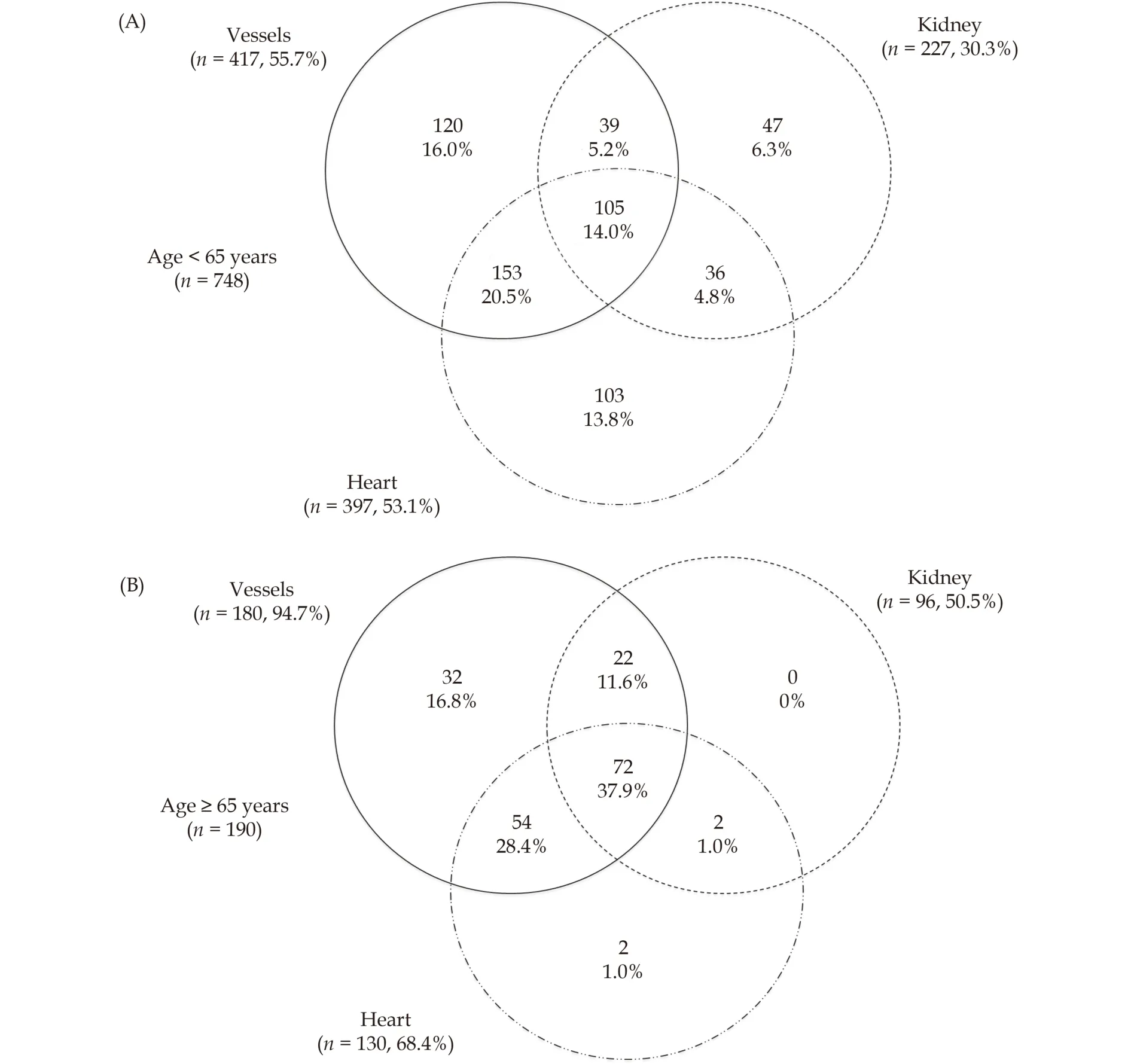
Figure 1 Association between different hypertension-mediated organ damages in patients < 65 years (A) and ≥ 65 years (B)

Figure 2 Overlap between electrical and anatomical left ventricular hypertrophy in patients < 65 years (A) and ≥ 65 years (B).HMOD: hypertension-mediated organ damage; LVH: left ventricular hypertrophy.

Table 2 Antihypertensive treatment at baseline.
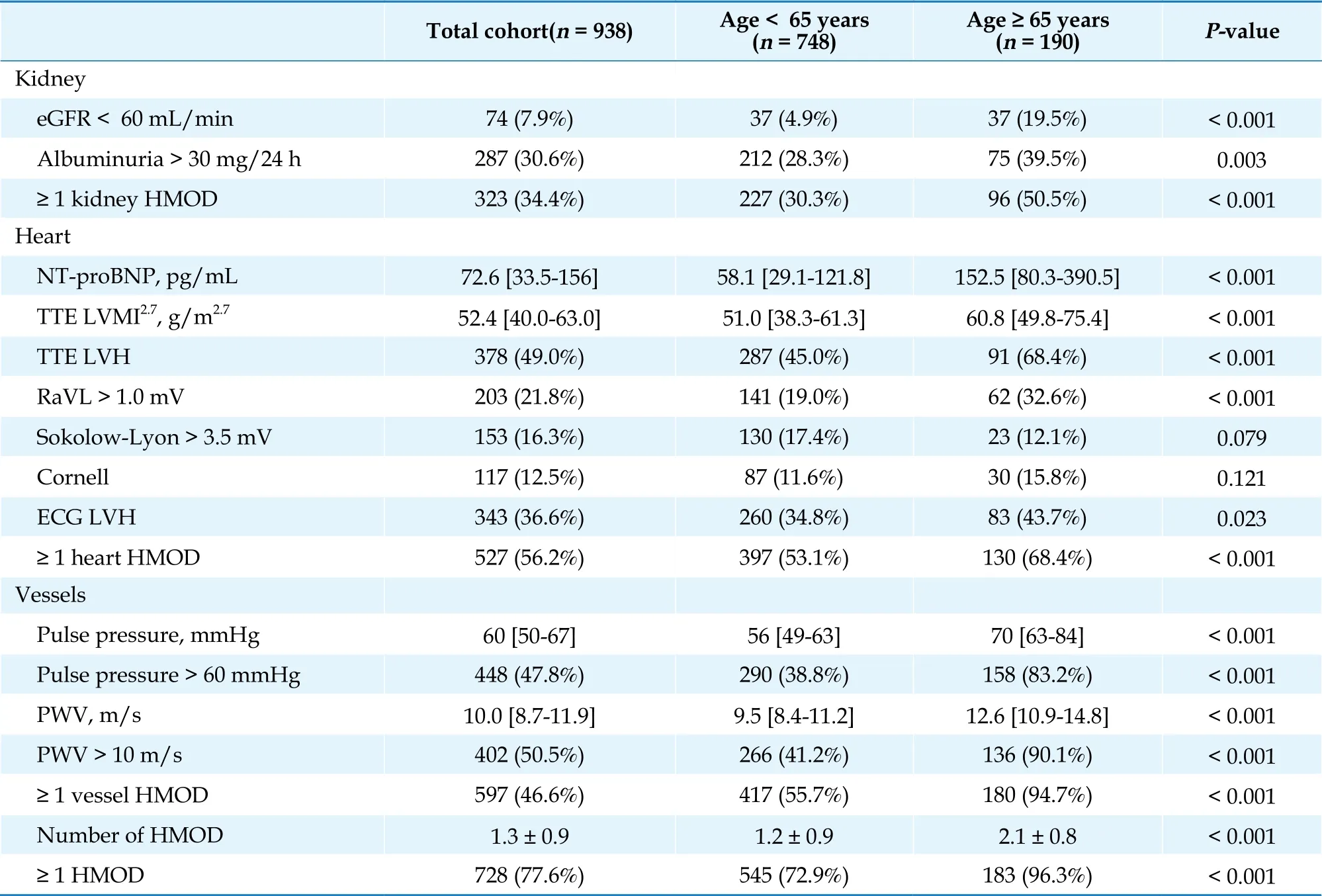
Table 3 Description of hypertension-mediated organ damage.
Secondary Forms of Hypertension
Essential hypertension was diagnosed in 70.0% of patients; there was no significant difference between age groups. In the total cohort, the most frequent secondary form was primary aldosteronism(20.6%), followed by renal disease (4.2%) and renovascular hypertension (3.2%). Reno-vascular hypertension and renal disease were more often observed in older patients; conversely primary aldosteronism was more frequent in younger patients.Patients with reno-vascular hypertension were all treated with percutaneous transluminal renal angioplasty: 8 with balloon (fibromuscular dysplasia)and 22 with stents (atherosclerotic renal artery stenosis). Adrenalectomy for primary aldosteronism was performed in 5/28 (17.8%) of patients ≥ 65 years and 44/165 (26.7%) of patients < 65 years. In the total cohort 5.3% of patients were diagnosed with obstructive sleep apnoea during their work-up of hypertension, and there was no significant difference between age groups; 38/50 (76%) were treated with automatic airway pressure, and there was no significant difference between age groups (Table 4 and Table S6 supplementary data). Secondary forms of hypertension were independently associated with age after adjustment to major confounders (Table S7, supplementary data).

Table 4 Aetiology and specific treatments.
DISCUSSION
In the present cohort, the prevalence of HMOD was 72.9% and 96.3% in patients aged < 65 years and ≥ 65 years, respectively. The most frequently detected HMOD in older patients were PWV and pulse pressure (that affected nearly all patients), followed by transthoracic echocardiography LVH. By contrast in those aged < 65 years, echocardiography LVH followed by PWV were the most frequent HMOD observed, but in less than half of patients. Of note, the high frequency of increased aortic stiffness in older hypertensive patients was expected since the mean PWV value was > 10 m/s in
the general population of the same age[12]and > 15.0 m/s in normotensive and hypertensive patients > 80 years.[16]From a patho-physiological point of view,various mechanisms are involved in aortic stiffening, in response to age and cardiovascular risk factors; they include breaks in elastin fibres, cross-links of the elastin network, and accumulation of collagen.[17]Carotid-femoral PWV may be the more relevant HMOD to screen in older hypertensive patients because of its high frequency observed herein, its pathophysiological mechanism, and its strong prognostic value to predict cardiovascular events and mortality.[18]However, PWV assessment requires a specific device that is mostly only available in tertiary centres, and is time consuming. Pulse pressure is widely available, may be used as a surrogate of PWV, and was also very frequently observed in patients ≥ 65 years herein. Similarly, but at the heart level, ECG is a widely available tool which may performed by general practitioners in the baseline work-up of hypertensive patients; herein, around three-quarters of ECG LVH was detected using the simple index RaVL >1.0 mV in older patients. Interestingly, the Sokolow-Lyon and Cornell indexes were above normal values twice less frequently than RaVL. It has also been reported that RaVL was a good index of LVH compared with cardiac magnetic resonance imaging (MRI) and has the advantage of a univocal threshold of 1.0 mV in various clinical conditions and in both sexes;[11]it is associated with major cardiovascular events, as well as cardiovascular and all-cause mortality in several cohorts of hypertensive patients and had better performance of other LVH ECG indexes.[19-21]The observations made herein suggest that the first method to screen LVH in patients aged ≥ 65 years is the ECG and that among the indexes available it is the RaVL that should be used. The second method to screen LVH is transthoracic echocardiography to explore more precisely the anatomical compound.Anatomical LVH was more frequently detected than electrical LVH in both age groups herein. This is in line with previous reports that found low sensitivity of electrical LVH (usually < 25%), albeit high specificity (up to 95%) of ECG criteria for diagnosis of LVH compared to echocardiography or MRI.[22,23]However, these two subtypes of LVH may be clinically distinct entities, each may provide distinct prognostic and, potentially, mechanistic information.[24]The overlap between electrical and anatomical LVH was less frequent in older patients, but LVMI unassessable by transthoracic echocardiography was relatively frequent in older patients. Kidney HMOD was less frequent than either heart or vessel HMOD her-ein (present in a third of younger patients, and half of older patients), but this may be explained by the inclusion of patients addressed to a cardiology department. A more general note is that more than 90% of older patients addressed to our department had ≥ 1 HMOD; this questions the need for screening for HMOD in this population and whether it would not be more pertinent to consider that all patients are at high risk. However, these results may not be generalizable as patients were addressed for resistant or difficult-to-treat hypertension.
Secondary hypertension affects only 5%-10% of hypertensive patients and their screening may be expensive and time consuming.[25]Extensive screening is usually proposed to patients with high clinical suspicion (young adults, resistant or severe hypertension, low plasma potassium, reduction of eGFR after initiation of a renin-angiotensin-system blockers…).[25]In the present cohort, we observed that the frequency of secondary hypertension was similar in younger and older patients. The frequency of primary aldosteronism in both age groups was very close to that previously described in resistant hypertension (6%-23%);[26]it was, however,less frequent in older patients. Adrenalectomy for primary aldosteronism was less frequently performed in older patients than in the younger ones,indicating a higher frequency of bilateral secretion of aldosterone. Nevertheless, it may be important to screen for unilateral secretion because it has been demonstrated that adrenalectomy after selection by adrenal venous sampling in older hypertensive patients contributes to a biochemical improvement of aldosterone secretion, as well as a decrease of antihypertensive treatment and BP.[27]However, antihypertensive treatment need to be continued in around three-quarters of patients aged ≥ 65 years despite adrenalectomy.[27]In case of bilateral secretion, the diagnosis of primary aldosteronism remains of particular importance to introduce spironolactone which may be difficult to use in elderly hypertensive patients with frequent side effects (hyperkalemia, worsening renal function).[28]The second most frequent aetiology in older patients herein was reno-vascular hypertension; the frequency of which was significantly higher than in younger patients. Percutaneous transluminal renal angioplasty was performed in all older patients in whom this was indicated; recognition of patients who may benefit for this procedure to improve BP control and reduce antihypertensive treatment may be challenging and needs a multidisciplinary approach.The CORAL and ASTRAL trials failed to identify substantial BP differences in patients treated with percutaneous transluminal renal angioplasty in comparison to patients with medical treatment alone.[29,30]Nonetheless, the considerable limitations have been highlighted on several occasion.[31]Recently, it has been demonstrated that patients with true resistant hypertension may benefit from percutaneous transluminal renal angioplasty by a substantial decrease of ambulatory BP and number of hypertensive treatments.[15]
Limitations
This study was performed in a tertiary healthcare institution and most patients were addressed for difficult-to-treat hypertension, resistant hypertension or suspected secondary hypertension; this might have reduced the generalizability of the results for a first screening in all-comers hypertensive patients, by overestimating the prevalence of HMOD,as well as an over-representation of secondary hypertension cannot be ruled out in the realization of our cohort. However, the baseline characteristics of this population indicated a fairly low-risk profile.Another limit to mention is the absence of specific follow-up in our department for patients treated for secondary forms (adrenalectomy, renal angioplasty)to assess the BP reduction. In fact, most of them were addressed to their cardiologist after the procedure. Finally, multiple statistical test may be associated with type 1 error (i.e., false positive results).
Conclusion
An extensive screening of HMOD in older patients may be questionable as nearly all patients had one. However, aetiology in older patients must be explored in the same way as younger patients as a third of patients over 65 years addressed for resistant or difficult to treat hypertension had a secondary form.
Acknowledgments
We thank Philip Robinson (Direction de la Recherche Clinique et de l’Innovation, Hospices Civils de Lyon) for thorough editing of the article. We thank Fatou Langevin, Fatma Zourane and Bianca Baluyot for methodological support.
Sources of Funding
None external to the authors' affiliations.
Conflict(s) of interest/Disclosure(s)
None.
猜你喜欢
保健与生活(2022年16期)2022-08-06 08:37:42
上海医学(2019年8期)2019-02-12 16:10:44
小演奏家(2016年5期)2016-05-14 15:11:12
中国麻业科学(2015年5期)2015-12-28 06:22:07
哈尔滨医药(2015年6期)2015-12-01 03:58:22
天津人大(2015年9期)2015-11-24 03:26:13
肿瘤预防与治疗(2015年1期)2015-09-26 07:26:22
中国卫生标准管理(2015年25期)2015-01-27 01:05:38
分忧(2014年9期)2014-09-22 04:55:36
湖北科技学院学报(医学版)(2014年2期)2014-02-28 19:42:33
 Journal of Geriatric Cardiology2022年11期
Journal of Geriatric Cardiology2022年11期
- Journal of Geriatric Cardiology的其它文章
- Review on the management of cardiovascular risk factors in the elderly
- Observation of performance measures of STEMI in elderly after implementation of an updated protocol: results from a single center without coronary interventions
- Migration of intra-aortic balloon pump causing obstruction of the superior mesenteric artery
- Device-based neuromodulation for cardiovascular diseases and patient’ s age
- Methodology in coronary artery bypass surgery quality assessment
- Small-molecule 7,8-dihydroxyflavone counteracts compensated and decompensated cardiac hypertrophy via AMPK activation