
Upper gastrointestinal endoscopic findings in celiac disease at diagnosis: A multicenter international retrospective study
2022-11-25 08:16:48JuanPabloStefanoloFabianaZingoneCarolinaGizziIlariaMarsilioMarLujEspinetEdgardoGustavoSmecuolMarkKhaouliMarLauraMorenoMarPintonchezSoniaIsabelNiveloniElenaVerdCarolinaCiacciJuliosarBai
World Journal of Gastroenterology 2022年43期
Juan Pablo Stefanolo, Fabiana Zingone, Carolina Gizzi, Ilaria Marsilio, María Luján Espinet, Edgardo Gustavo Smecuol, Mark Khaouli, María Laura Moreno, María I Pinto-Sánchez, Sonia Isabel Niveloni, Elena F Verdú,Carolina Ciacci, Julio César Bai
Abstract
Key Words: Celiac disease; Upper gastrointestinal endoscopy; Concomitant endoscopic lesions;Malignancies; Multicenter study
INTRODUCTION
Celiac disease (CeD) is one of the most common life-long chronic diseases affecting people with a genetic predisposition conferred by HLA-DQ2 or DQ8[1]. Current recommendations for diagnosing CeD in adult patients involve a combination of specific serology and a duodenal biopsy demonstrating some degree of intestinal atrophy[2,3]. When CeD is clinically suspected, upper gastroduodenal endoscopy with duodenal biopsy confirms diagnosis[4]. Based on the very high specificity and predictive values of specific serology tests[5], the diagnosis of CeD without duodenal biopsy has been proposed in recent years[6-8]. Indeed, European pediatric societies recommend a non-biopsy approach under specific and strict criteria[9,10]. However, other pediatric societies (e.g., the North American Pediatric Gastroenterology Society) do not recommend this, in part because relevant comorbid diagnosis could be missed[11]. This is of particular concern in patients with alarm symptoms such as weight loss, anemia, or abdominal pain[2,12,13]. However, relatively few studies have explored this indepth, particularly in adult patients undergoing endoscopy to confirm CeD diagnosis[14-16].
Thus, we conducted a multicenter study involving four cohorts of patients diagnosed in three countries to investigate the prevalence of coincidental upper gastrointestinal endoscopic findings in CeD patients at the time of diagnosis. We also compared upper gastrointestinal mucosal injury diagnoses across centers and age groups. Finally, we studied the pathological findings in patients with a confirmed diagnosis of CeDvsthose in whom the disease was ruled out.
MATERIALS AND METHODS
Design
We conducted a descriptive multicenter retrospective study on endoscopic findings from adult patients who met standard clinical, serological, and histological criteria for CeD. Patients from four different CeD-specialized centers were included. Two European cohorts (Universities of Naples/Salerno and Padua; Italy) and a North American cohort (McMaster University, Hamilton; Canada) recruited consecutive patients enrolled in local registers. CeD was diagnosed by positive serology and confirmed by biopsy. The Naples/Salerno cohort included consecutive patients seen between 1987 and 2021, the Padua cohort between 2017 and 2021, and the Hamilton cohort between 2018 and 2020. A fourth (Small Bowel Section, Dr. C. Bonorino Udaondo Gastroenterology Hospital, Buenos Aires; Argentina) included patients referred for endoscopy and duodenal biopsy due to the presence of symptoms and/or signs compatible with CeD but, irrespective of serology, all of them part of prior research and study[7,15].Thus, the fourth cohort included CeD and non-CeD participants (controls). Figure 1 and Table 1 summarize the demographic characteristics of the cohorts. The Ethics and Research Board of the Dr. C.Bonorino Udaondo Gastroenterology Hospital approved the study because of the prospective design and intervention in the Buenos Aires cohort. Ethics approval was obtained from Hamilton Integrated Research Ethics Board (HiREB# 14460/5415). In Italy, Ethical Committee review was not required for retrospective studies while patient data remained anonymously coded.
Endoscopic procedures
In all CeD centers, experienced gastroenterologists performed upper gastrointestinal endoscopies and obtained duodenal biopsiespershared standard of care protocols. Endoscopic reports were generated using a standard format, and the data were entered into a common database. Duodenal biopsies were sent to each institution’s experienced pathologist. A standard number of biopsies were taken when any endoscopic abnormality was detected (e.g., endoscopic evidence of esophageal metaplasia). Endoscopic abnormalities were defined as follows[17]: (1) Erosive esophagitis: Esophageal mucosal damage characterized by one or more mucosal breaks that do not extend across the top of mucosal folds and confluent lesions or ulcers of any size; (2) Suspected esophageal metaplasia: Endoscopically suspected columnar mucosa without histological confirmation of specialized intestinal metaplasia; (3) Barrett’s esophagus confirmed by biopsy: Metaplastic columnar epithelium replacing the stratified squamous epithelium in biopsies from suspected metaplasia or presence of intestinal metaplasia; (4) Gastric and duodenal erosions: Presence of erythema and erosions in stomach or duodenum; (5) Esophageal, gastric, or duodenal ulcers extending into themuscularispropria; and (6) Esophageal, gastric, or duodenal cancer:Suspected endoscopic lesions were confirmed by specialized pathology.
CeD diagnosis
CeD was diagnosed based on duodenal histology (Marsh’s classification)[1,18]. Inclusion criteria were Marsh 2 enteropathy or higher and positive CeD-specific serology [presence of either anti-TTG immunoglobulin (Ig)A, Anti-EmA IgA, anti-DGP IgA/IgG]. When serology was negative, CeD was diagnosed based on histology and clinical response to the gluten free diet (GFD)[18]. If patients had known exposure to gluten before the endoscopy, intestinal biopsies were taken. As previously stated,the Buenos Aires cohort was part of a research study in which the diagnosis was made first on histological grounds and then confirmed by serology. The standard specific CeD test for all centers was IgA transglutaminase 2[5]. Patients with normal biopsy or minimal inflammation (Marsh 0 or 1) were excluded from the study, regardless of serology or GFD response. In the Hamilton cohort, diagnosis of seronegative CeD patients was based on histology and a clinical and histological response to the GFD.
Data analysis
Statistical analysis was carried out using STATA (STATA version 14.0 Corp, College Station, TX, United States). Categorical variables were reported as frequencies and percentages, while continuous variables were reported as mean ± SD and/or median and 25%-75% interquartile ranges, according to their distribution. Comparisons of categorical variables between groups were made using theχ2test or Fisher’s exact test.Pvalues < 0.05 were considered statistically significant. For comparisons of continuous variables the analysis of variance test was used. Logistic regression was used to assess the risk of endoscopic lesions. The model included the report of significant lesions in endoscopy and/or histology reports as a dependent variable and factors such as age, sex, personal history, and signs/symptoms as independent variables.
Given the different recruitment times between centers, a subgroup analysis was performed to compare results in the Naples/Salerno cohort, focusing on cases diagnosed between 2018 and 2021vsprevious endoscopies, estimating that such analysis could detect differences by using more actualized endoscopic protocols that were temporally concordant with those reported from patients collected in the Padua and Ontario cohorts.
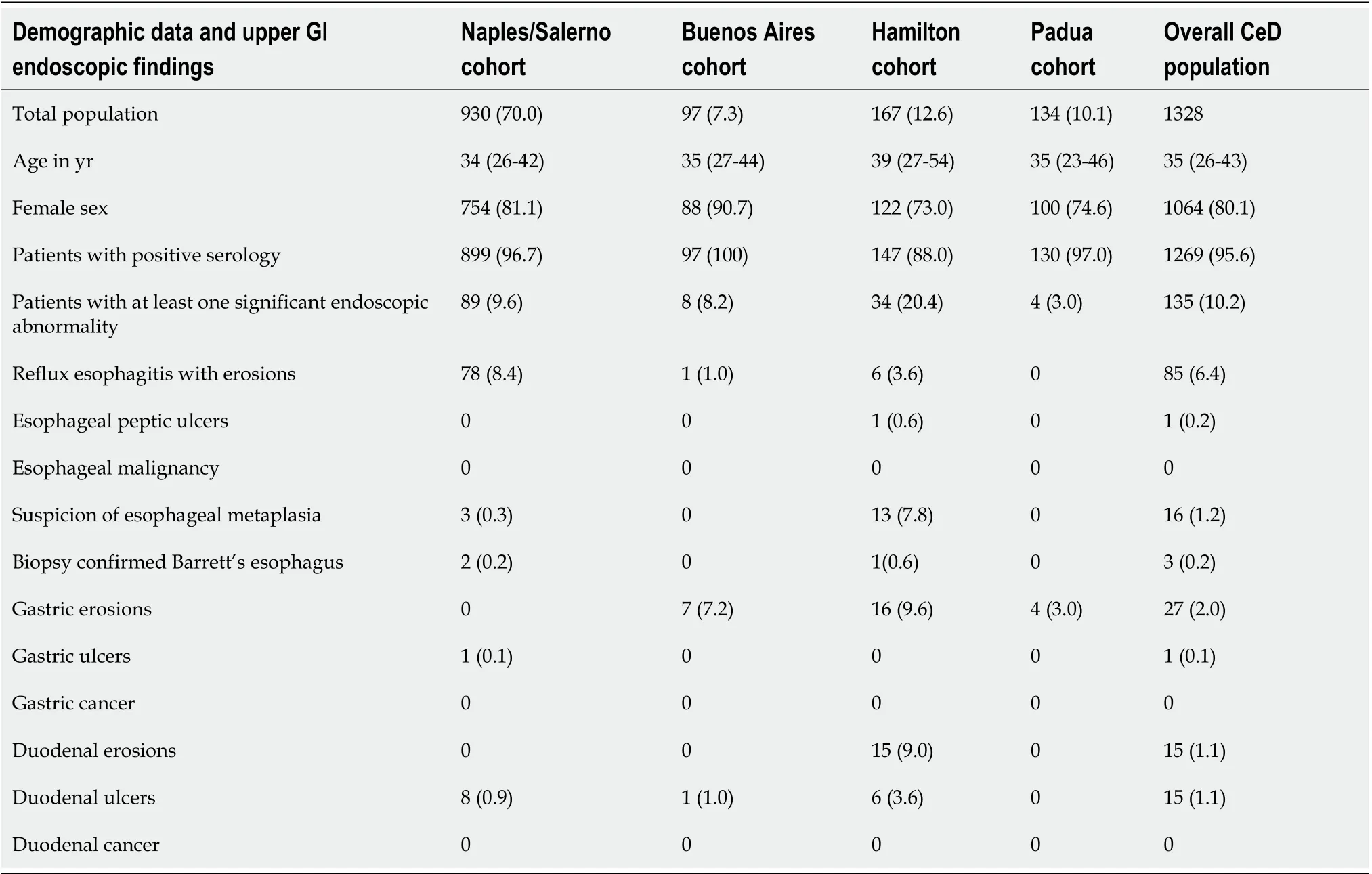
Table 1 Demography, celiac disease serology, and endoscopic findings by cohorts and the overall population
RESULTS
Overall, 1404 patients were diagnosed with CeD and 1328 of them were included in the study (Figure 1).Patients with slightly positive serology but Marsh 0 or 1 (n= 76) were not diagnosed as CeD.
Demographic and clinical characteristics
The number of participants recruited varied between centers (Tables 1 and 2). The Naples/Salerno cohort contained most (70.0%) of the patients, while the Buenos Aires cohort had the fewest patients(7.3%). The European and North American centers differed in the length of time the celiac centers had been operational. The South American center included patients and controls over a specific time previously enrolled in a different study. There was a female predominance in all groups. There was no difference in the age at which diagnostic endoscopy was performed. There were no differences in baseline demographics across centers. The percentage of patients testing positive for celiac specific antibodies ranged from 88% (Hamilton) to 100% (Buenos Aires).
Endoscopic findings in CeD patients and age-related damage
Endoscopy revealed 163 distinct abnormalities in 135 patients with CeD (10.1%) (Table 1). The most common finding was erosive reflux esophagitis (6.4%), with the highest prevalence in the Naples/Salerno cohort (8.4%) and the lowest in the Buenos Aires (1%) and Padua (0%) cohorts. Peptic esophageal ulcers were only found in 1 patient within the total cohort. Although Barrett’s esophagus was suspected in 1.2% of the patients, it was biopsy confirmed in 0.2% of cases (18.7% of those suspected and subsequently biopsied). The Hamilton cohort had a higher suspicion of metaplasia (n=13), but Barrett’s esophagus was confirmed in 1 patient (Table 1). Gastric ulcers were found in 1 patient(0.1%) within the Naples/Salerno cohort, while gastric erosions were found in 2.0% of the total population, with a higher prevalence in the Buenos Aires (7.2%) and the Hamilton (9.6%) cohorts. In the latter, 9.1% of patients with duodenal erosion were documented. Overall, 1.1% of duodenal ulcers were discovered, with a higher frequency encountered in the Hamilton cohort (3.6%). No cancers were reported at any level of the upper gastrointestinal (GI) tract of CeD patients.
Patients under the age of 50 had a lower risk of having at least one abnormality compared with patients over the age of 51 (P< 0.01). This indicated a 96.6% increase in lesions found in older patients(8.9%vs17.5%), which was primarily driven by erosive esophagitis and gastric erosions (Table 2). We performed a subgroup analysis of the Naples/Salerno cohort, including patients diagnosed between 2018 and 2021. Compared with the overall Naples/Salerno cohort, patients diagnosed recently (n= 86)had a higher percentage of at least one significant endoscopic abnormality (29.2%vs9.6%, respectively),owing to a higher proportion of cases with erosive reflux esophagitis (20.0%vs8.4%) and duodenal ulcers (8.2%vs0.9%, respectively). These endoscopic features were more common in the Naples/Salerno cohort (after 2018) than in the other cohorts (Padua and Hamilton) (P< 0.01). Compared with the Padua cohort, the Salerno cohort had a higher proportion of patients with at least one endoscopic abnormality (29.1%vs3.0%;P< 0.01) (Supplementary Table 1).
Endoscopic findings in celiac patients and non-celiac controls from the Buenos Aires cohort
We compared CeD patients (n= 97)vsnon-CeD controls (n= 674) (Table 3) using the Buenos Aires cohort. The median age at endoscopy in non-CeD controls was 11 years higher than in patients with CeD, and the percent of females was lower (P< 0.01 for both). Compared with patients with CeD, a higher proportion of controls were under the age of 50 (P< 0.001) (Table 3). CeD specific serology was positive in 1.3% of non-CeD controls. IgA transglutaminase positive levels in controls were less than three times the upper limit of normal. Endoscopic findings were more frequent in controls than in CeD patients (P< 0.001). In all age groups, gastric erosions were most common. Two control subjects, both older than 51, had a stomach adenocarcinoma and another a duodenal cancer at diagnostic endoscopy.In contrast, no cancers were discovered in CeD patients. Metaplasia was found in 1.0% of controls, with Barrett’s esophagus being confirmed after biopsy in two of these cases. Controls over the age of 51 had 12.9% more frequent mucosal damage compared with younger subjects (overall prevalence 31.4%vs27.8%, respectively).
The crude multivariate analysis based on CeD patients and non-CeD controls found that a CeD diagnosis and presence of alarm symptoms(weight loss, anemia, bleeding, dysphagia, epigastric pain, or history of malignancy) reduced the risk of having at least one lesion by 78.0% and 49.0% (P< 0.0001 for both), respectively. According to the adjusted multivariate analysis, having CeD was associated with a 72% reduction in the risk of any endoscopic lesion (P< 0.0001), and having alarm symptoms was associated with a 37% reduction in the risk of having at least one endoscopic lesion (P< 0.02; Table 4).
DISCUSSION
The study’s main finding was that upper endoscopy performed concurrently with duodenal biopsies for CeD diagnosis revealed no concomitant damage in 92.0% of cases. Only 1.6% of CeD patients had relevant findings with the potential to progress to severe disease, comprised by esophageal and gastric ulcers and Barrett’s esophagus. While 8.9% of patients demonstrated upper GI injury, only 1.3%potentially had dangerous lesions. The low yield of relevant concomitant findings in this study does not support the usefulness of upper endoscopy beyond the need of obtaining biopsies for the diagnosis of CeD.
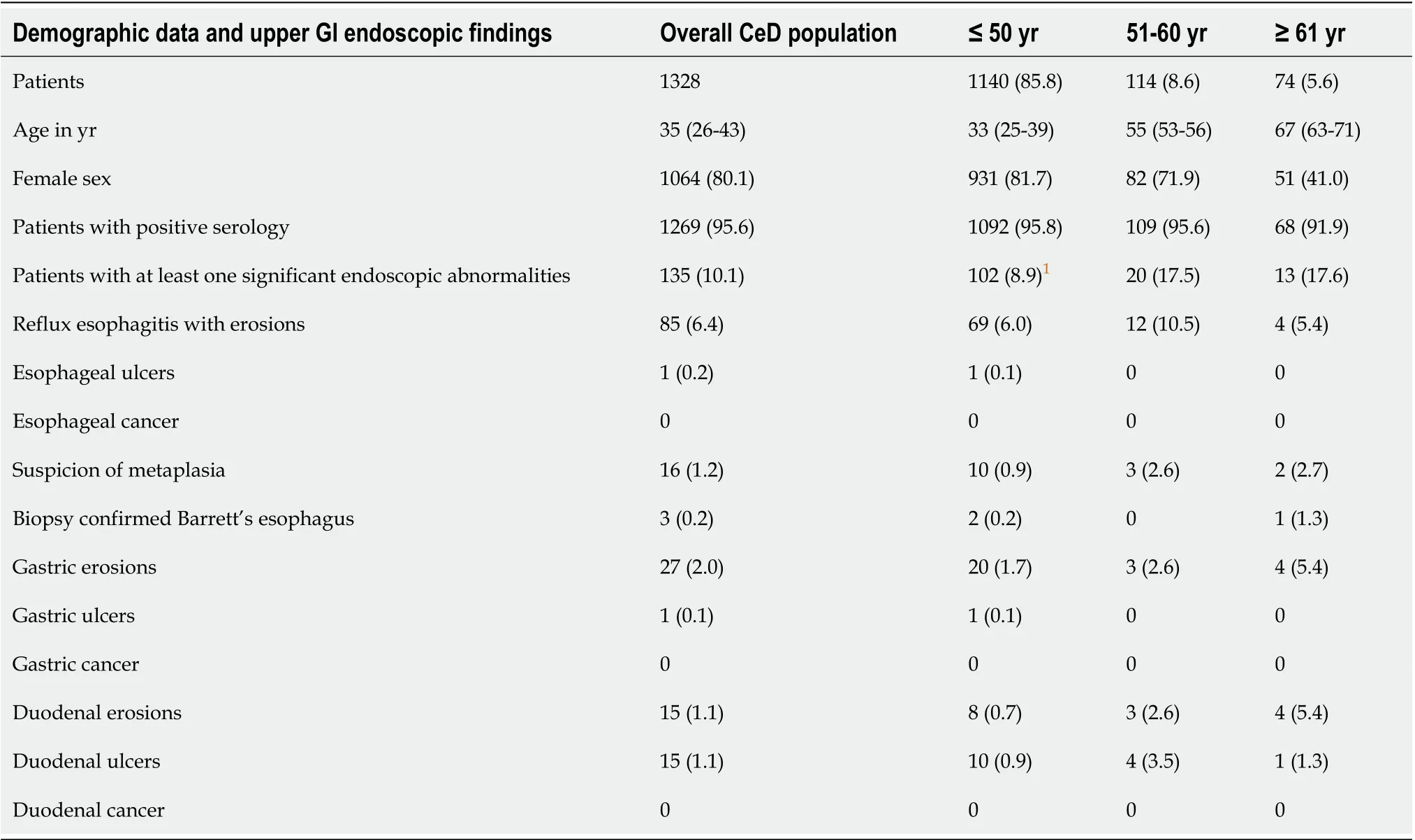
Table 2 Demography, celiac disease serology, and endoscopic findings of the overall population and by the age of diagnosis
The possibility of detecting important or relevant esophageal, gastric, or duodenal pathology during diagnostic endoscopy has been put forward as an added benefit to the confirmation of CeD. Previous findings in CeD patients include reflux esophagitis, esophageal eosinophilia or eosinophilic esophagitis(mostly in children), Barrett’s esophagus,Helicobacter pylori(H. pylori) infection and autoimmune gastritis[14-16]. These were, however, reported in small populations and single center studies. Our study, which included cohorts from the European Union, North America, and South America, gathered the largest sample of patients reported to date. The sample size collectively obtained allowed for subgroup and age category comparisons. The majority of CeD patients were young and female, as expected. The Buenos Aires cohort was prospectively designed to diagnose symptomatic patients suspected of having CeD, which allowed for comparisons between CeD patients and controls biopsy(Marsh’s 0 or 1 histology categorization).
Our findings in a large multicenter population confirm recent reports that adult patients with alarm symptoms have a very low prevalence of major endoscopic and histological findings in the upper GI tract other than CeD features at presentation and was comparable to that of patients without alarm symptoms[14,16]. The definition of what constitutes an alarming symptom for CeD at the time of diagnosis appears to be central to this analysis. Weight loss, iron deficiency anemia, pain, or malabsorption symptoms were prevalent among symptomatic patients, which constitutes the vast majority of currently diagnosed CeD patients since a case finding strategy is recommended[19]. However, our findings were limited to the upper GI tract, and the lower GI tract was not explored.
Erosive reflux esophagitis was the most common endoscopic finding at the time of diagnosis (6.4%).Notably, undiagnosed patients with classical or subclinical CeD frequently seek treatment for gastroesophageal reflux symptoms prior to diagnosis, which has been shown to be more common in subjects in whom CeD is ruled out or in those treated with the GFD[20]. We previously reported that up to 30% of newly diagnosed CeD patients perceive moderate to severe reflux symptoms, which does not respond to anti-reflux therapy prior to CeD diagnosis[21,22]. Most of these “non-responsive” patients to antireflux therapy will rapidly improve after starting the GFD. Surprisingly, between 2018 and 2021, the Naples/Salerno cohort revealed higher prevalence of overall endoscopic lesions, and specifically of erosive reflux esophagitis, compared with diagnoses made before that time. This could be attributed to the characteristics of the CeD population over time or to differences in the reporting of endoscopic and histology findings.
The possibility of missing severe lesions or potentially dangerous diseases in CeD patients if a diagnostic endoscopy is not performed has been a source of concern in CeD guidelines[2,4]. With respect to Barrett’s esophagus or esophageal metaplasia, an Italian study published in 2005 showedmetaplasia in 26.6% of CeD patients compared with 10.9% of the control population[23]. This was not confirmed in studies from the United States[24]and South America[15,21]nor by the present study.Reasons for this discrepancy could be related to differences in populations and in the definition of Barrett’s esophagus, which required confirmation by biopsy in our study.
In the present study, we did not find mucosal eosinophilic infiltration. A pediatric prospective longitudinal study based on systematic esophageal biopsies found that diagnoses of eosinophilic esophagitis and/or eosinophilia were not clinically relevant, suggesting esophageal biopsy is not necessary in the absence of clinical suspicion[25]. A 2015 cross-sectional population study in the United States based on a national pathology database involving over 88000 CeD patients with both esophageal and duodenal biopsies, reported a slight increase in comorbid eosinophilic esophagitis and CeD[24]. However, no link between reflux esophagitis or Barrett’s esophagus and CeD has been reported. Finally, autoimmune atrophic gastritis was previously modestly associated with CeD[26]. Our study, as well as other population-based studies and systematic reviews, did not confirm the association[27,28].
An earlier prospective study[15]collected consecutive patients and non-CeD controls in a high-risk population for having CeD, and gastric and duodenal biopsies were performed systematically at the time of the diagnostic endoscopy CeD and biopsy. Gastric biopsies from untreated CeD patients also revealed a significantly higher intraepithelial lymphocyte count in the antrum and corpus when compared with controls[15,29,30]. According to an Irish study, 10% of CeD patients have lymphocytic gastritis, which is twice the rate of non-CeD controls[12,14]. These findings are attributed toH. pyloriinfection, autoimmune atrophic gastritis[15,26], or a pan-mucosal gluten-related inflammation[14,15,29,30].
Our study showed only 1 CeD patient had a gastric peptic ulcer. Previous studies found 18.1% of CeD children with gastric ulcers, with a higher prevalence inH. pylorinegative patients and those with no history of nonsteroidal anti-inflammatory drug use[31,32]. The rate ofH. pyloriinfection across centers was not consistently reported here, and this could explain the difference in results. Previous research,however, has shown that high rates of biopsy-confirmedH. pyloriinfection are not associated with an increased risk of malignancy in the long term[27,33]. However, several studies have also shown that when endoscopic appearance is normal, histological evaluation (both in the stomach and the esophagus)is not cost-effective, especially when performed in experienced academic centers[34-36].
南通市的直接经济腹地主要包括南通市及其辖区和苏中盐城、淮安、泰兴等部分地区。间接经济腹地可以继续延伸至江苏、安徽、江西等地区,甚至深入至西部等内陆地区,长江中上游和苏北地区货物总量的70%在此中转。随着南北方向门户的贯通,其经济腹地可以进一步向南北延伸。同时,随着南通深入贯彻实施“一带一路”倡议,截至2017年5月,南通中天科技与59个“一带一路”沿线国家和地区进行合作。这意味着南通经济腹地将会继续往“一带一路”沿线延伸,货源基础进一步提升。
There was no diagnosis of gastric adenocarcinoma in CeD. Despite the small number of cases studied,this is consistent with previous findings that the prevalence of other cancers (breast, colon, pulmonary,and gynecological cancers) in CeD appears to be lower than in the general population[27,28]. Small bowel carcinoma is extremely rare in the general population, and CeD patients are three times more likely to develop it[1,28]. However, malignancies in the duodenum are still uncommon at the time of CeD diagnosis, which implies diagnostic CeD endoscopy should not be recommended as surveillance for upper GI cancer[28]. Overall, the current findings, as well as those from previous studies, suggest that a biopsy-avoiding approach in adult patients who meet recommended and strict serological criteria for CeD is possible[12,37-40].
Study strengths included the multicenter design, the large number of patients diagnosed at specialized centers for CeD in whom confirmatory biopsy diagnosis was obtained, as well as the use of standard endoscopic protocols. Despite the small numbers in sub-analyses, the study also provided novel data related to the association of endoscopic findings according to age and time. Study limitations included the observational design, the retrospective collection of endoscopic reports (with potential missing data), the differences in time of enrollment across the four centers, the lack of systematic collection of biopsies from the esophagus and stomach, and the limited number of non-CeD controls.Although the current study suggests that missing potentially serious events is unlikely, this should be confirmed in a larger population.
CONCLUSION
In conclusion, this multicenter, retrospective study found that comorbid upper GI endoscopic pathology is uncommon in patients with positive CeD serology at the time of diagnostic endoscopy. The risk of severe or premalignant lesions is extremely low, and no malignancies were found in patients who displayed potential warning signs. Our findings suggest that a non-biopsy strategy for diagnosing CeD in adults is unlikely to miss clinically significant concomitant endoscopic findings unrelated to CeD. The results of this study should encourage future population-based or prospective studies in this area.
ARTICLE HIGHLIGHTS
Research background
Celiac disease (CeD) is currently diagnosed in adult patients using a combination of specific serology tests and a duodenal biopsy obtained through an upper endoscopy. Upper endoscopy is also considered necessary for CeD diagnosis because non-CeD comorbidities can be missed.
Research motivation
The prevalence of upper gastrointestinal comorbidities at the time of CeD diagnosis has received little attention.
Research objectives
To investigate the prevalence of coincidental upper gastrointestinal endoscopic findings at the time of diagnostic endoscopy in four cohorts of patients diagnosed in three different countries.
Research methods
We conducted a descriptive multicenter retrospective study reporting endoscopic findings from adult patients who met standard criteria for diagnosing CeD.
Research results
Of 1328 adult patients enrolled, 95.6% had positive specific serology. In 135 patients, endoscopy revealed 163 abnormalities unrelated to CeD (10.1%). Erosive reflux esophagitis (6.4%), gastric erosions(2.0%), and suspicion of esophageal metaplasia (1.2%) were the most common findings. Biopsyconfirmed Barrett’s esophagus was infrequent (0.2%). No other neoplastic or malignancies lesions were detected. Patients with alarm symptoms or signs had a lower rate of concomitant findings.
Research conclusions
Adults with positive CeD serology had few comorbid endoscopic findings when CeD was diagnosed.
Research perspectives
These findings raise the possibility that adult patients who meet recommended and strict serological criteria for CeD could be diagnosed without undergoing endoscopy and biopsy.
FOOTNOTES
Author contributions:Stefanolo JP, Ciacci C, Zingone F, Gizzi C, Marsilio I, Espinet ML, Pinto-Sánchez MI, and Niveloni SI contributed with data acquisition; Stefanolo JP performed the statistical analysis; Stefanolo JP, Pinto-Sá nchez MI, Ciacci C, Zingone F, and Bai JC contributed to study design; Verdú EF, Smecuol EG, Moreno ML contributed to critical analysis; Bai JC, Verdú EF, Ciacci C, Pinto-Sánchez MI and Zingone F contributed to writing and critical review of the manuscript; All authors read and approved the final manuscript.
Institutional review board statement:The Ethics and Research Board of the Dr. C. Bonorino Udaondo Gastroenterology Hospital approved the study because of the prospective design and intervention in the Buenos Aires cohort. Ethics approval was obtained from the Hamilton Integrated Research Ethics Board (HiREB#14460/5415). In Italy, Ethical Committee review was not required for retrospective studies while patient data remained anonymously coded.
Informed consent statement:Informed consent was not required by the Ethics and Research Committee of the Hospital de Gastroenterología Dr. C. Bonorino Udaondo (Buenos Aires, Argentina) given the retrospective nature of the study and because this study was categorized as minimal risk by the Committee.
Conflict-of-interest statement:All the authors report no relevant conflicts of interest for this article.
Data sharing statement:Technical appendix, statistical code, and dataset available from the corresponding author at jbai@intramed.net. Consent was not obtained, but the presented data are anonymized and risk of identification is low.
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is noncommercial. See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:Argentina
ORCID number:Juan Pablo Stefanolo 0000-0003-0679-3470; Fabiana Zingone 0000-0003-1133-1502; Edgardo Gustavo Smecuol 0000-0002-4451-819X; María Laura Moreno 0000-0002-0120-8789; María I Pinto-Sánchez 0000-0002-9040-9824;Sonia Isabel Niveloni 0000-0002-1534-1604; Elena F Verdú 0000-0001-6346-2665; Carolina Ciacci 0000-0002-7426-1145;Julio César Bai 0000-0003-4159-0185.
S-Editor:Fan JR
L-Editor:Filipodia
P-Editor:Fan JR
猜你喜欢
英语世界(2023年12期)2023-12-28 03:36:06
光明少年(2023年4期)2023-04-29 00:44:03
华人时刊(2021年15期)2021-11-27 09:16:26
华人时刊(2020年15期)2020-12-14 08:10:52
华人时刊(2018年15期)2018-11-10 03:25:36
开放导报(2017年3期)2017-06-27 12:16:59
企业文化·中旬刊(2015年12期)2016-03-09 02:38:42
中国老区建设(2016年1期)2016-02-28 09:32:04
星星·散文诗(2015年34期)2015-10-26 19:25:18
财经科学(2014年5期)2015-04-13 02:28:33
 World Journal of Gastroenterology2022年43期
World Journal of Gastroenterology2022年43期
- World Journal of Gastroenterology的其它文章
- Integrity of the editing and publishing process is the basis for improving an academic journal’s Impact Factor
- Kyoto classification of gastritis: Advances and future perspectives in endoscopic diagnosis of gastritis
- Current status of minimally invasive liver surgery for cancers
- Salvia miltiorrhiza extract may exert an anti-obesity effect in rats with high-fat diet-induced obesity by modulating gut microbiome and lipid metabolism
- Correction to “MicroRNA-596 acts as a tumor suppressor in gastric cancer and is upregulated by promotor demethylation”
- Differential analysis of intestinal microbiota and metabolites in mice with dextran sulfate sodium-induced colitis