
Death related to ethyl chloride inhalation abuse: a case report
2022-09-01 05:20IanZhiruiHongPonampalam
Ian Zhirui Hong,R Ponampalam
Department of Emergency Medicine,Singapore General Hospital,169608,Singapore
Dear editor,
Human exposure to hydrocarbons (HCs) is unavoidable given their wide usage in a variety of common products.Ethyl chloride (EC),a type of halogenated HC,has been used in the production of pharmaceuticals,dyes,and other chemicals used for industrial purposes.EC was used as an anesthetic induction agent in the early 1900s.Although its use as an inhalational agent has fallen out of favour,EC is still used as a topical pain medication today.
The sale of EC as a topical analgesic agent is not regulated in Singapore.This means that it can be acquired over the counter (OTC) with relative ease,thus making it a convenient choice as a volatile substance of abuse in Singapore.Deaths related to EC inhalation abuse are uncommon,with only a handful of reported cases.This case report of death related to EC inhalation abuse highlights the dangers of this substance of abuse.
CASE
A 25-year-old woman was evacuated by emergency ambulance service to the emergency department (ED)in cardiorespiratory arrest following suspected EC inhalation.On arrival of paramedics at the scene,she was in cardiac arrest.There was no bystander cardiopulmonary resuscitation (CPR).The initial electrocardiogram (ECG) rhythm was asystole.Paramedics initiated CPR and instituted airway management using laryngeal mask airway (LMA).Return of spontaneous circulation (ROSC) was achieved on scene after a brief period of CPR,and no shocks or adrenaline were administered.On arrival to the ED,she was unresponsive,and her pupils were fixed and dilated with no spontaneous breathing.Her initial blood pressure(BP) was 77/40 mmHg (1 mmHg=0.133 kPa).Her heart rate (HR) was 155 beats/min,and her ECG showed sinus tachycardia.She was afebrile (temperature 36 °C),with a respiratory rate (RR) of 24 breaths/min and a pulse oximetry reading of 100%.Her airway was secured via endotracheal intubation upon arrival.Fluid resuscitation was started,and adrenaline was added to support her blood pressure.Lung fields were clear on chest X-ray with the endotracheal tube in proper position.Computed tomography (CT) of the brain revealed cerebral edema suggestive of early hypoxic-ischemic encephalopathy(HIE).Laboratory values (Tables 1 and 2) on arrival to the ED showed severe metabolic acidosis with transaminitis,mildly elevated chloride and glucose levels,and a normal creatinine.Paracetamol and salicylate levels were not elevated.A blood toxicology screen despatched from the ED was positive for EC (<1 mg/100 mL),fentanyl(<1 ng/mL),and citalopram (0.04 μg/mL).
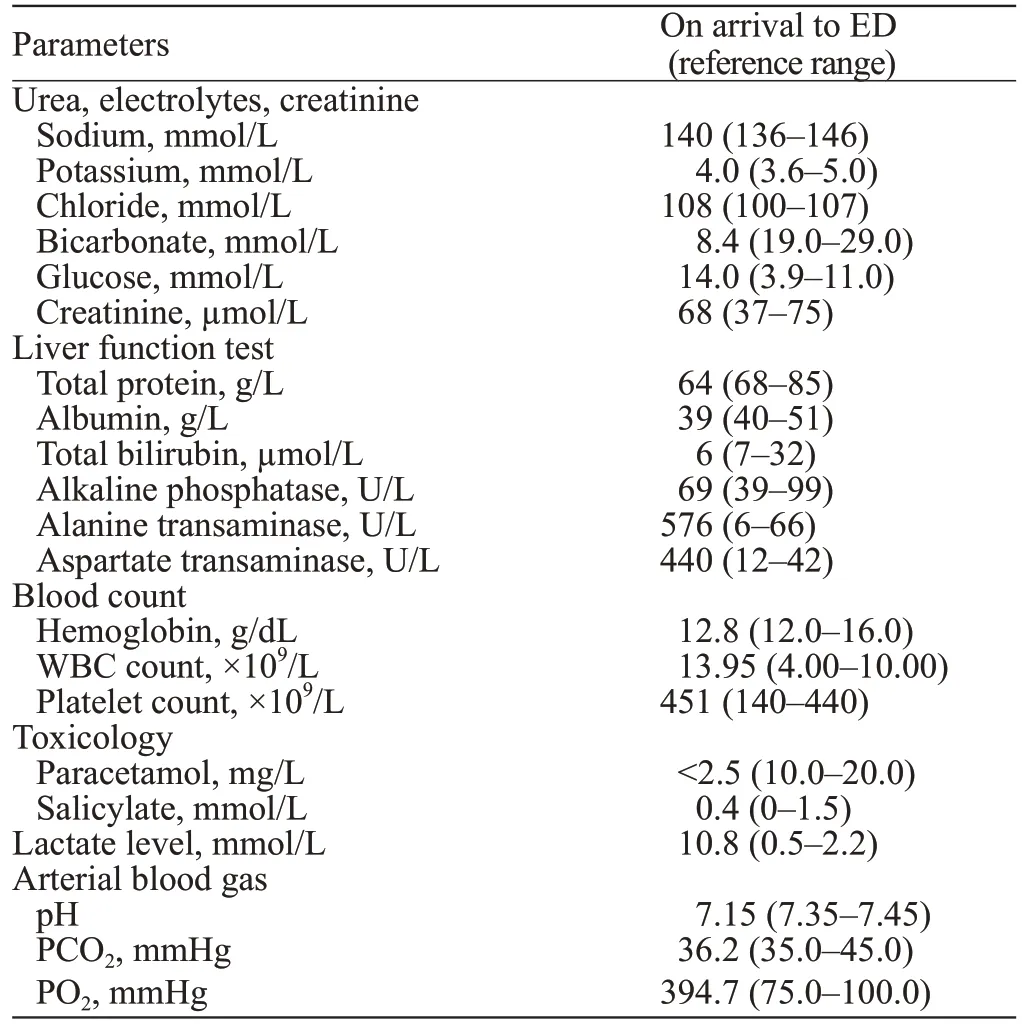
Table 1. Laboratory values on arrival to the emergency department
Although paramedics did not find drug paraphernalia at the scene,a receipt for a recent purchase of four cans of EC spray was found on her.A total of 11 cans of EC sprays were also found in her possession,of which eight were empty and three were partially used.A review of her electronic medical records showed a past history of inhalant abuse for which she was on follow-up.
She was admitted to the intensive care unit (ICU)and started on a therapeutic hypothermia protocol for targeted temperature management (cooled to 36 °C).Upon admission to the ICU,her vitals were stable (HR 118 beats/min,BP 125/104 mmHg,SpO100%,RR 28 breaths/min),and the initial hypotension resolved without further need for inotropes.The indwelling urinary catheter inserted in the ED drained clear urine,and dialysis was held off as her metabolic acidosis improved.
She had exhibited myoclonic jerks approximately 3 h after arrival to the ED,and these were also observed intermittently when she was in the ICU.She later developed seizure-like activity approximately 12 h after presentation,which was aborted after 2 mg of midazolam.Her seizures were subsequently managed with levetiracetam 1 g every eight hours.No further seizure activity was noted after starting levetiracetam.An electroencephalogram (EEG) suggested the presence of severe encephalopathy.
She developed a fever 3 d later with elevated inflammatory markers and was treated for sepsis.The chest X-ray was unremarkable,and urine culture showed coagulase-negativespecies.On the fourth day of admission,her sodium levels increased rapidly to 160 mmol/L (reference range 136-146 mmol/L) and persisted despite free water treatment via nasogastric tube (NGT) and intravenous (IV) dextrose drip.Magnetic resonance imaging (MRI) performed for neuroprognostication showed HIE with early encephalopathy.She subsequently became persistently hypotensive despite fluid resuscitation and died on day five of her admission without regaining consciousness.
DISCUSSION
The use of EC in medicine has a long history dating back to the early 1900s as an inhalational anesthetic agent.However,its use as an inhaled anesthetic fell into disrepute due to fatalities potentially related to its toxic effects.Currently,EC is mainly used as a topical analgesic.The analgesic effects of EC are achieved due to its physical properties of having a low boiling point(~12 °C),which creates an evaporative cooling effect when used as a spray.
The use and stages of the effect of EC inhalation have been described by Lawson.According to Lawson,the anesthetic effects of EC are achieved within minutes when used as an induction agent.When inhaled,EC is readily absorbed to produce unconsciousness within minutes.It is also rapidly excreted by the lungs,accounting for its quick reversal and cessation of effects.A patient with EC inhalation abuse that initially presented with neurological effects appeared to achieve complete recovery shortly upon cessation of its use.While the effects of EC inhalation are self-limiting and prolonged acute effects may not be common,deaths resulting from EC inhalation have been reported (supplementary Table 1).
Deaths due to EC inhalation are likely a result of cardiorespiratory arrest.The cardiac effect was,in part,the reason for the decline in EC use as an anesthetic agent.Cardiovascular (CV) depression has been noted to occur simultaneously with respiratory depression.Although respiratory depression effects were quickly reversed when EC inhalation was ceased,CV depression effects were unlikely to resolve spontaneously without external interventions.The patient presented in this case report had persistently elevated levels of Troponin and CKMB levels (Table 2) suggestive of cardiac ischemia.A study with dogs showed that EC inhalation led to vagal stimulation and affected the myocardium directly,resulting in arrhythmias.A cohort study by Assadi noted ECG changes and arrhythmias to be common in workers with occupational exposure to solvents and suggested that such changes were likely due to cardiac sensitisation.Similar to other solvents,EC inhalation may result in cardiac sensitisation and fatal arrhythmias.

Table 2. Trend of cardiac enzymes
Due to the serious consequences of EC inhalation,education and awareness to highlight such effects needto be promoted.This is an important approach in curbing the use of EC as a recreational drug of abuse.EC appears to be the choice volatile substance of abuse among youths,possibly due to its relatively low cost and easy availability.This has prompted some countries,such as the United Arab Emirates (UAE),to monitor the sale of EC and raise awareness amongst the public of such practices.The prevalence of EC inhalational abuse in Singapore is not known,although occasional reports of this form of volatile substance abuse have surfaced in the news previously.Death related to EC inhalational abuse has not been reported in Singapore before,and there have only been a handful of reported deaths in the literature.A concerted effort among various agencies is essential in raising awareness and promoting education to curb the spread of EC inhalational abuse.
CONCLUSIONS
The OTC sale of EC spray will need to be reexamined to curb the relative ease in acquiring EC,which may be used as a convenient option in volatile substance abuse.In view of the potential dangers of recreational EC inhalation,education is important in highlighting these dangers and the associated forms of volatile substance abuse.
None.
Not needed.
The authors declared no potential conflicts of interest with respect to the research,authorship,and/or publication of this article.
IZH proposed and wrote the paper.All authors read and approved the final version.
All the supplementary files in this paper are available at http://wjem.com.cn.
 World Journal of Emergency Medicine2022年5期
World Journal of Emergency Medicine2022年5期
- World Journal of Emergency Medicine的其它文章
- Intestinal microcirculation dysfunction in sepsis:pathophysiology,clinical monitoring,and therapeutic interventions
- Timing of brain computed tomography for predicting neurological prognosis in comatose cardiac arrest survivors: a retrospective observational study
- Development and evaluation of a predictive nomogram for survival in heat stroke patients: a retrospective cohort study
- Analysis of imaging characteristics of blunt traumatic aortic dissection: an 8-year experience
- Is rosuvastatin protective against sepsis-associated encephalopathy? A secondary analysis of the SAILS trial
- Arctigenin attenuates paraquat-induced human lung epithelial A549 cell injury by suppressing ROS/p38 mitogen-activated protein kinases-mediated apoptosis