
Analysis of imaging characteristics of blunt traumatic aortic dissection: an 8-year experience
2022-09-01 05:20LiLiLiyingLinYuanqiangLu
Li Li ,Li-ying Lin ,Yuan-qiang Lu
1 Department of Emergency Medicine,the First Affiliated Hospital,School of Medicine,Zhejiang University,Hangzhou 310003,China
2 The Key Laboratory for Diagnosis and Treatment of Aging and Physic-chemical Injury Diseases of Zhejiang Province,Hangzhou 310003,China
BACKGROUND: Traumatic aortic dissection (TAD) has a low incidence but extremely high mortality.It always presents atypical clinical manifestations that are easily missed or misdiagnosed.This study mainly aims to describe the imaging characteristics and management of TAD patients.METHODS: A retrospective analysis of 27 blunt TAD patients was performed between 2013 and 2020.Demographic features,imaging characteristics,and management were analyzed.RESULTS: Twenty-seven patients with type B aortic dissection (age 56.04±16.07 years,20 men) were included.Aortic intimal tears were mostly initiated from the aortic isthmus.The sizes of the proximal intimal tears in the greater curvature were larger than those in the lesser curvature (1.78±0.56 cm vs.1.24±0.52 cm,P=0.031).Compared with those in the control group,the maximum diameters of the aortic arch,thoracic aorta,and abdominal aorta in the TAD patients were all significantly widened (all P<0.050).Multivariate logistic regression analysis showed that the maximum diameter of the thoracic aorta was an independent risk factor for TAD,with a predictive value with an area under the receiver operating characteristic curve(AUC) of 0.673.Finally,26 patients successfully underwent delayed thoracic endovascular aortic repair(TEVAR),and the remaining one patient was treated conservatively.No progression of aortic dissection or death occurred during the six-month follow-up period.CONCLUSIONS: In blunt trauma,the aortic isthmus is the most common site of proximal intimal tears.An accurate diagnosis of TAD requires an overall consideration of medical history and imaging characteristics.Delayed TEVAR might be an effective therapeutic option for TAD.
KEYWORDS: Blunt trauma;Traumatic aortic dissection;Imaging characteristic;Diagnosis;Delayed thoracic endovascular aortic repair
INTRODUCTION
Blunt traumatic aortic injury (BTAI) remains a rare but potentially devastating disease.Approximately 75% of patients with BTAI die before arriving at the hospital,and over half of the survivors die within 24 h after admission.A previous study showed that more than 80% of traumatic aortic injuries were accompanied by varying degrees of multiple injuries.The clinical manifestations of trauma patients range from non-specific symptoms to chest and back pain or even coma,which significantly increases the difficulty of an early diagnosis of BTAI.
As one type of BTAI,traumatic aortic dissection (TAD)is easily overlooked or misdiagnosed,and the rate of missed diagnosis is as high as 60%.Furthermore,the mortality of TAD increases significantly if not recognized early.Thus,the prompt and precise diagnosis of TAD is particularly important for the survival and prognosis of trauma patients.Owing to its rapidity and high diagnostic accuracy,computed tomography angiography (CTA) has become the most common examination method in patients with aortic dissection.Therefore,understanding the CTA imaging features and clinical features of TAD is strongly conducive to its clinical diagnosis.Currently,thoracic endovascular aortic repair (TEVAR) has become a standard treatment for aortic injuries.Cheng et alhas recommended TEVAR as a preferred treatment option for TAD.Furthermore,the timing of TEVAR is crucial.Compared with early endovascular repair,delayed TEVAR (> 24 h from time of admission) for BTAI can effectively reduce mortality.This study mainly aims to describe the imaging characteristics of TAD for rapid and accurate diagnosis and timely treatment.
METHODS
Patients
In our study,TAD was defined as acute aortic dissection induced by various types of trauma.We included patients who were diagnosed with TAD at our hospital from May 13,2013,to October 21,2020.Patients who met the following inclusion criteria were enrolled: (1) patients with age ≥18 years; (2) blunt trauma as the mechanism of injury,such as that resulting from motor-vehicle accidents (MVAs),falls,and strikes;and (3) aortic CTA was performed immediately after admission if aortic dissection was suspected or confirmed.The exclusion criteria were as follows: (1)patients with age <18 years;(2) patients who were previously diagnosed with aortic dissection;(3) patients who had repeated chest and back pain and did not undergo aortic CTA examination before blunt trauma;(4) patients with a family history of aortic disease and inflammatory diseases of the aorta;(5) patients with concomitant serious diseases,such as heart,lung,hepatic,and renal failure,inherited connective-tissue disease (e.g.,Marfan syndrome,Ehlers-Danlos syndrome,and Turner syndrome),blood system diseases,and malignancies;and (6) patients with incomplete clinical data. Additionally,we conducted a six-month followup of the enrolled patients after discharge.
Data extraction
Demographic characteristics and clinical data were acquired from the electronic clinical notes of our hospital.The data mainly comprised age,sex,routine blood tests,biochemical test indexes,type of trauma,accompanying injuries,type of aortic dissection,imaging characteristics,admission injury severity (Injury Severity Score [ISS] and Abbreviated Injury Scale [AIS]),treatments,and outcomes.Laboratory data were collected from the patient’s first admission.Data were mainly manually extracted by LL and LYL and verified by YQL.
Main outcome measures and definitions
Multiplanar reformation (MPR) was applied to measure the maximum diameters of the ascending aorta,aortic arch,thoracic aorta,and abdominal aorta,and the size of the proximal intimal tear.To measure the aortic diameter,the aorta was fully exposed at the axial position,and the intersection of the rotation axis was placed at the midpoint of the aorta.The rotation axis was rotated to fully expose the aorta to be measured on the coronal plane,and the maximum diameter of the aorta was measured (supplementary Figures 1 A1 and A2).To measure the proximal intimal laceration,the intimal tear was fully exposed in the axial position,and the rotation axis was placed at the midpoint of the initial tear.The rotation axis was then rotated to fully expose the initial tear to be measured on the coronal plane,and the maximum length of the initial tear was measured(supplementary Figures 1 B1 and B2).Moreover,the length of aortic dissection was measured on the coronal plane after the aorta was fully exposed.These measurements were obtained after receiving training from senior doctors in the imaging department.An experienced radiologist supervised and guided the measurement process of the maximum aortic diameter and proximal intimal tear size.
The parameters were as follows: (1) lesser curvature the inner arc of the aortic arch (direction of the black arrow)(supplementary Figure 1 C1);(2) greater curvature the outer arc of the aortic arch (direction of the black arrow)(supplementary Figure 1 C2),and both black arrows showing typical aortic intimal tears;(3) Range 1 aortic dissection distally involving the upper layers of the celiac trunk;(4) Range 2 aortic dissection distally involving the artery between the celiac trunk and the common iliac artery;(5) Range 3 aortic dissection distally involving the iliac artery segment.The location and extent of the initial tear of the aortic dissection were confirmed using CTA.
Statistical analyses
Continuous variables conforming to a normal distribution are presented as the mean±standard deviation (SD),and others are presented as medians (interquartile ranges,IQRs).Categorical data are expressed as number and percentages.An independent sample-test or Mann-Whitney-test was applied to evaluate continuous data,and the Chi-square test was used to analyze categorical variables.Multivariate logistic regression analyses identified independent risk factors for TAD.The area under the receiver operating characteristic curve (AUC) was calculated to assess the predictive power of the thoracic aortic maximum diameter in diagnosing TAD.The statistical analysis of all the obtained data was conducted using SPSS software (version 21.0).
RESULTS
Clinical characteristics
Twenty-seven patients were included in the study(supplementary Figure 2),including 20 men and 7 women,with a mean age of 56.04±16.07 years (range 28-86 years).Twenty-one patients were transferred from other hospitals,and the remaining 6 patients were hospitalized directly.Over 40%of the patients had a history of smoking.Approximately 30%of the patients had hypertension or atherosclerosis.Twenty-four patients had chest pain,two were admitted to the hospital with a coma,and one showed abdominal pain due to a significant history of abdominal impact.The chest was the common site of injury with AIS ≥3.MVAs and falling injuries were the two main types of trauma (Table 1 and supplementary Table 1).
The body temperature of 20 patients was within the normal range,while fluctuated between 37.4 and 38.8 °C in the other seven patients.Only four patients (14.81%)had a systolic blood pressure greater than 140 mmHg (1 mmHg=0.133 kPa).The breathing and heart rates were within the normal range in more than 90% of patients.The levels of D-dimer (=27,100%),C-reactive protein (CRP,=25,92.59%),and neutrophil-to-lymphocyte ratio (NLR,=13,48.15%) significantly exceeded the upper limit of normal values.The remaining laboratory results showed no obvious abnormalities in most patients (supplementary Table 2).
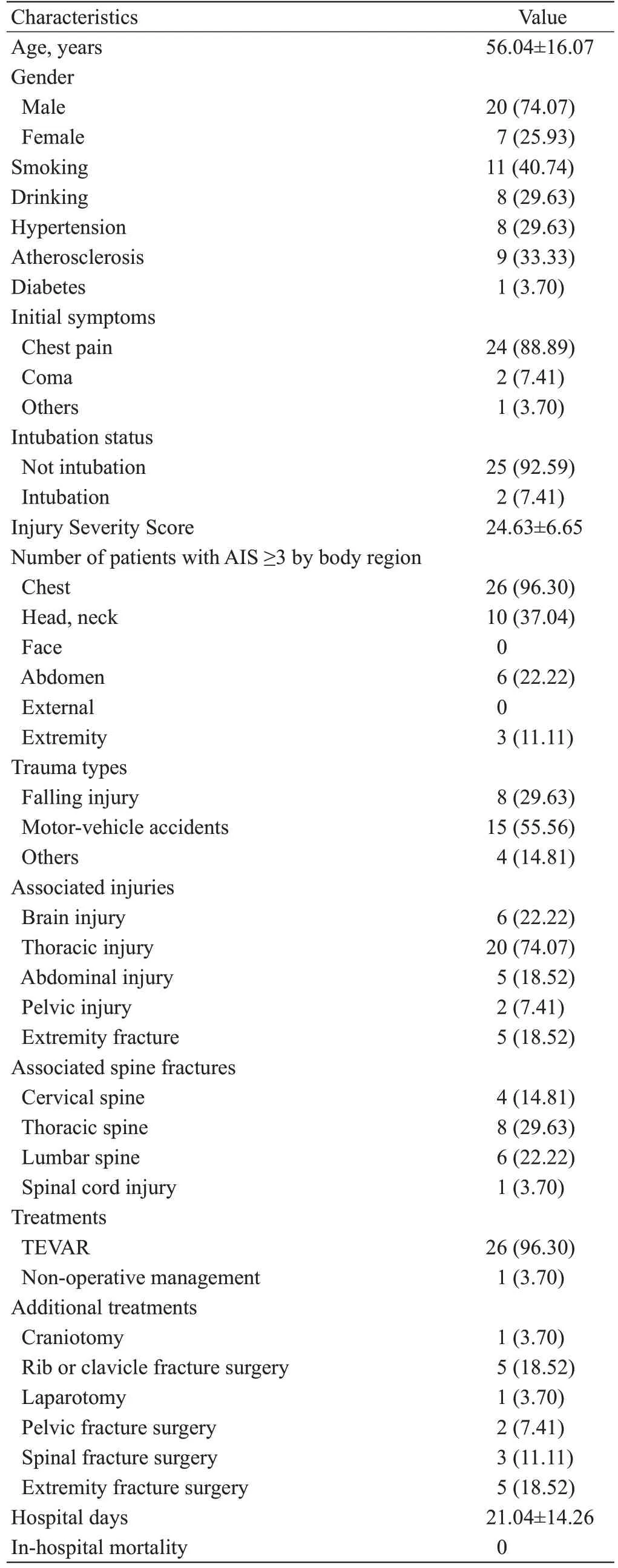
Table 1. Baseline characteristics of patients with TAD (n=27)
Imaging characteristics of TAD
In our series,27 patients were all classified with DeBakey III aortic dissection.Proximal aortic intimal tears were mainly initiated from the aortic isthmus,with 18 patients from the lesser curvature and seven patients from the greater curvature.The intimal tears of the remaining two patients were initiated from the distal thoracic aorta (T10 level) and the abdominal aorta (superior mesenteric artery branch level),respectively (Figure 1A).The sizes of the intimal tears in the greater curvature (1.78±0.56 cm) were larger than those in the lesser curvature (1.24±0.52 cm),with a significant difference(=0.031) (Figure 1B).The age of patients with intimal tears initiated from the greater curvature (62.86±15.38 years) was older than that of patients with intimal tears initiated from the lesser curvature (52.29±16.50 years).However,there was no significant difference (=0.175) (Figure 1C).Additionally,there were no significant differences in injury patterns or the extent of dissection involved between patients with intimal tears initiated from the lesser and greater curvature,respectively (Figures 1 D and E).
The maximum diameter in each segment of the aorta
Ninety age-and sex-matched individuals who underwent CTA for chest pain were included in the control group.All patients underwent CTA examination without significant aortic abnormalities.There was no statistically significant difference in sex between the TAD patients and the healthy control group (both>0.05).Compared with the healthy control group,TAD patients showed varying degrees of widening of the aortic diameter in the aortic arch(2.85±0.34 cm vs.2.65±0.30 cm,=0.003),thoracic aorta(2.99±0.56 cm vs.2.66±0.35 cm,=0.007),and abdominal aorta (2.25±0.42 cm vs.2.06±0.22 cm,=0.041).However,no significant changes were found between the TAD patients and the control group in the maximum diameter of the ascending aorta (3.61±0.62 cm vs.3.44±0.39 cm,=0.194)(Figure 2A).After a preliminary analysis,the maximum aortic diameter of the aortic arch,thoracic aorta,and abdominal aorta (all<0.050) were included in the multivariate logistic regression analysis.With the use of the forward stepwise method,the maximum diameter of the thoracic aorta (oddsratio [] 6.604,<0.001) was considered an independent risk factor for TAD.To evaluate the predictive value of thoracic-aortic diameter in the accurate diagnosis of TAD,ROC curve analysis was conducted with an AUC of 0.673(95% confidence interval [95%] 0.540-0.807,<0.001)(Figure 2B).The optimal cut-off value of the thoracic-aortic diameter was 2.89 cm (sensitivity 60%,specificity 76.7%,and Euclidean index 0.220).This result indicates that the widening of the thoracic-aortic diameter might have a predictive value in diagnosing TAD.

Figure 1. Locations of proximal aortic intimal tears and features of intimal tears in the isthmus.A: each black dot represents a patient,and the area where the black dot is located is the approximate location where the aortic intimal tear is initiated;B: comparison of aortic intimal tear size in patients with intimal tears initiated from the lesser curvature and greater curvature,respectively;C: comparison of age in patients with intimal tears initiated from the lesser curvature and greater curvature,respectively;D: injury patterns in patients with intimal tears initiated from the lesser curvature and greater curvature,respectively;E: range of intimal tears in patients with intimal tears initiated from the lesser curvature and greater curvature,respectively.

Figure 2. Comparison of maximum aortic diameter and receiver operating characteristic curves.A: comparison of the maximum diameter of the ascending aorta,aortic arch,thoracic aorta,and abdominal aorta between traumatic aortic dissection (TAD) patients and the control group;B:receiver operating characteristic curves of thoracic aorta maximum diameter.
Treatments and clinical outcomes
All patients received symptomatic and supportive treatment on admission,including sustaining systolic blood pressure within 80-110 mmHg and a heart rate of approximately 60 beats/min,sedation and analgesia,and corresponding trauma management.Twenty-six patients successfully underwent TEVAR within 3-7 d after admission and fracture surgery approximately seven days after stent implantation.One patient underwent intestinal surgery due to intestinal rupture.The length of aortic dissection and intimal tear size of the patient were 2.91 cm and 0.80 cm,respectively.He and his family members strongly refused surgical treatment or TEVAR for TAD.The patient was eventually treated conservative ly.Obvious endo-graft migration and intimal leakage were not observed in patients who underwent TEVAR.All patients survived during the six-month follow-up.
DISCUSSI ON
TAD patients often present other concomitant bodily injuries.An investigation that enrolled 24,010 BTAI patients reported that most patients had chest injury,with rib fractures and pulmonary contusion occurring most frequently.In a nationwide case series,Sheehan et aldiscovered that rib fractures,spine fractures,a nd trunk abrasion were risk factors for blunt abdominal aortic injury (BAAI).Moreover,previous research has found that MVAs are a common cause of traumatic aortic injury.In our analysis,over 70% of patients presented with rib fractures,and more than 48%of patients presented with spinal fractures.MVAs were responsible for 55.56% of the TADs.Thus,the index of suspicion for TAD might be raised in blunt trauma patients when injured in MVAs and in the presence of rib fractures and spinal fractures.Further prospective randomized controlled studies with larger sample sizes need to be conducted to arrive at a definite conclusion.Previous studies indicated that plasma D-dimer,CRP,and NLR may have predictive value for diagnosing or assessing the severity of acute aortic dissection (AAD).Likewise,the levels of plasma D-dimer and CRP are both dramatically elevated in most of the above 27 TAD patients,with an increased NLR in 13 patients.
Due to the existence of the arterial ligament,the isthmus located at the area between the moveable and fixed aspects of the aorta is more susceptible to various mechanical forces.Therefore,over 54.0%-91.4% of BTAIs involve the aortic isth mus.In our study,approximately 93%of proximal intimal tears were initiated from the aortic isthmus,especially in the lesser curvature.Moreover,ancircuit model of chronic type-B aortic dissection found that the risk of false lumen expansion increased with the enlargement of aortic intimal-tear size.In this study,the proximal intimal-tear size in the greater curvature was generally larger than that in the lesser curvature.However,there was no significant difference in the intimal tear range.Additionally,the injury pattern and the extent of dissection between patients with intimal tears initiated from the lesser curvature and greater curvature showed no obvious difference.
The maximum diameter in each segment of the aorta was also measured and compared between TAD patients and healthy controls.We found that the aortic diameters of the TAD aorta were widened to varying degrees in the aortic arch,thoracic aorta,and abdominal aorta.Moreove r,the maximum diameter of the thoracic aorta may be an independent predictive indicator for the diagnosis of TAD.This reason might be that DeBakey III aortic dissection was the major type in our cases.Several risk factors for inducing spontaneous aortic dissection have been recognized,such as smoking,hypertension,and atherosclerosis.In our cases,approximately 30%-40% of patients had a history of smoking,hypertension,or atherosclerosi s.
Regarding treatment strategies for BTAI,major methods include medical management,TEVAR,and a surgical approach.Because TEVAR is a less invasive treatment for BTAI,its favorable early outcomes have been described.Research suggests that the mortality of BTAI is remarkably lower in patients treated with delayed repair than in those with immediate repair.In our study,aft er the strict control of blood pressure and no obvious progression of aortic dissection,26 TAD patients underwent delayed TEVAR.Obvious endograft migration and intimal leakage were not observed in patients who underwent TEVAR during the six-month followup.One patient underwent intestinal surgery due to intestinal rupture.In addition,because the length of aortic dissection and intimal tear size were small,he and his family members strongly refused surgical treatment or TEVAR for TAD.Therefore,the patient received conservative treatment.A previous study also suggested that regular observation and non-operative management (NOM) might be a reasonable therapeutic option for grade III BTAI.Ultimately,all patients survived with satisfactory clinical outcomes during the six-month follow-up.
Limitations
First,this was a single-center,retrospective study with a limited sample size.Larger and multi-center prospective studies are needed to further represent the clinical characteristics of blunt-TAD patients.Second,some patients had not undergone aortic CTA examination in the past,so we could not determine whether it was a new dissection after trauma or an internal subclinical dissection worsening after trauma.Thus,our cases were enrolled under strict inclusion and exclusion criteria.Third,the long-term efficacy and complications of TEVAR in these patients remain unknown.Therefore,the follow-up time should be extended to as long as possible in future research.
CONCLUSIONS
The proximal aortic intimal tears are mainly initiated from the lesser curvature of the aortic isthmus.The rapid and correct diagnosis of TAD mostly depends on a deep understanding of the mechanism of injury and on maintaining high vigilance.Notably,the maximum diameter of the thoracic aorta might have predictive value in diagnosing TAD.In addition,delayed TEVAR may be an ideal choice for treating TAD.
ACKNOWLEDGMENTS
We truly appreciate the kind support of Prof.Ling-xiang Ruan in the measurement of the maximum aortic diameter and intimal tear size.
This study was supported by the National Natural Science Foundation of China (81272075 and 81801572) and the Foundation of Key Discipline Construction of Zhejiang Province for Traditional Chinese Medicine (2017-XK-A36).
The Ethical Committee of the First Affiliated Hospital,School of Medicine,Zhejiang University,approved this retrospective observational study (code number 2021288).The patients/participants provided written informed consent to participate in this study.
None.
LL and LYL contributed equally to this study.LL collected data,analyzed,and completed the manuscript.LYL offered statistical advice on analyzing the data.YQL supervised and revised the manuscript.
 World Journal of Emergency Medicine2022年5期
World Journal of Emergency Medicine2022年5期
- World Journal of Emergency Medicine的其它文章
- Intestinal microcirculation dysfunction in sepsis:pathophysiology,clinical monitoring,and therapeutic interventions
- Timing of brain computed tomography for predicting neurological prognosis in comatose cardiac arrest survivors: a retrospective observational study
- Development and evaluation of a predictive nomogram for survival in heat stroke patients: a retrospective cohort study
- Is rosuvastatin protective against sepsis-associated encephalopathy? A secondary analysis of the SAILS trial
- Arctigenin attenuates paraquat-induced human lung epithelial A549 cell injury by suppressing ROS/p38 mitogen-activated protein kinases-mediated apoptosis
- Hepatocellular carcinoma-derived exosomal miRNA-761 regulates the tumor microenvironment by targeting the SOCS2/JAK2/STAT3 pathway