
Gender inequalities in physical activity among adolescents from 64 Global South countries
2022-07-29 12:10LuizIsnriCrosoRiroAnreWentCrolineosSntosCostGregoreIvenMielkeJvierBrzoSyverAsuzzmnKhnTryKoleAlexnerInioCrohemoreSilv
Luiz Isnri Croso Riro,Anre Went,Croline os Sntos Cost,Gregore Iven Mielke,Jvier Brzo-Syver,Asuzzmn Khn,Try L Kole-Alexner,In′io Crohemore-Silv
a Federal University of Pelotas,Pelotas,RS 96010-040,Brazil
b University of S~ao Paulo,S~ao Paulo,SP 01153-000,Brazil
c School of Public Health,The University of Queensland,Herston,QLD 4006,Australia
d University of the Republic,Montevideo,Montevideo 11200,Uruguay
Abstract Purpose:The aims of this study were to(a)describe gender inequalities in physical activity (PA)among adolescents from Global South countries, and (b) investigate the relationship between gender inequalities in PA and contextual factors, such as geographic region, human development index,gender inequality index,and unemployment rates.Methods:We analyzed cross-sectional data from the Global School-Based Student Health Survey conducted in Global South countries between 2010 and 2020 among 13- to 17-year-old adolescents. Country-context variables were retrieved from secondary data sources (World Health Organization, World Bank, and Human Development Reports). PA was assessed by a self-administered questionnaire querying the number of days in the past week in which participants were physically active for a total of at least 60 min.PA absolute gender inequalities were evaluated by the differences in the prevalence between boys and girls, 95% confidence intervals (95%CIs) were estimated using the bootstrap method.Relative inequalities were obtained through Poisson regression. Meta-analyses with random effects were used to calculate pooled estimates of absolute and relative inequalities.Results:Based on 64 Global South countries/surveys,the prevalence of PA was 6.7 percentage points(p.p.)higher in boys than in girls,ranging from 0.5 p.p. in Afghanistan to 15.6 p.p. in Laos (I2= 85.1%). The pooled ratio for all countries showed that boys presented a PA prevalence 1.58 times higher than girls(95%CI:1.47-1.70)on average.The highest absolute and relative inequalities were observed in high income countries. Countries with higher Human Development Index rankings and lower Gender Inequality Index rankings also presented greater gender differences.Conclusion: Given that girls are overall less active than boys across the globe, the findings of this study reinforce that macro- and micro-level changes should be actively sought if we aim to increase population levels of PA in adolescents and promote equity in PA.
Keywords: Adolescents;Gender differences;Physical activity;Social inequalities;Students
1.Background
Adolescence is a critical period for health promotion,resulting in increased health benefits during adolescence,across the life course, and into the next generation.1,2During adolescence several physical, biological, and psychosocial changes occur,which could lead to changes in the adolescent’s overall health and negatively impact well-being throughout their life course.3,4Physical activity (PA) is an example of a healthy behavior severely impacted by the increasing academic, household, and occupational responsibilities in this period,5all of which are closely related to the social context of the adolescent.6Despite the several advantages of PA for health,7it is estimated that only around 20% of adolescents meet the former recommendation of at least 60 min of moderate-to-vigorous intensity PA (MVPA) daily, and these already concerning levels are declining in most countries.8In 2020,the PA guidelines were updated based on new evidence,resulting in a small change: adolescents are now required to do,on average,60 min of MVPA per day.9
Given that PA is a complex behavior determined by individual, social, and environmental factors, systems-based approaches targeting specific population groups that are more likely to be inactive are necessary to tackle physical inactivity worldwide. It is well known that gender, age, and socioeconomic status are important correlates of PA.10However, a large portion of the PA inequalities are due to the gender gap.Also, recent global estimates indicate an increase in the PA gender gap over time.11It is estimated that a decrease in inactivity levels of 4.8 percentage points (p.p.) among women across the world would be sufficient to achieve the World Health Organization’s(WHO)target of reducing global levels of inactivity by 15%by 2030.12
In addition to individual level approaches, contextual factors related to PA gender inequalities might also be relevant.Evidence suggests that societal gender inequality relates to gender differences in adolescent PA, where countries with higher Gender Inequality Index (GII) rankings tend to present low levels of PA and more gender inequalities.13,14Overall,different country contexts,such as country income,geographic region,15and global indices (Human Development Index(HDI), Gini coefficient, improved drinking water coverage,GII, public health expenditure, and mean years of schooling),could also be linked with PA in youth;16however, we are unaware of any previous publications that have investigated such contextual drivers of gender inequalities.
In this context, Global South countries face a wide discrepancy in distribution and access to health when compared to those in the Global North.17Historical colonialism and imperialism have resulted in persistent and increasing inequalities as well as a lack of social justice and human rights policies in these countries,18,19including the underrepresentation of women in several areas.20Furthermore,global surveillance of adolescents’PA is still limited,21especially in lowerincome countries22such as those in the Global South.
To comprehensively address inequalities in PA, analyzing absolute and relative measures of inequality is recommended given that these measures are complementary to each other in providing valuable insights about which groups may require greater attention.23,24Thus, the aims of this study were to (a)describe gender inequalities in PA among adolescents from Global South countries based on absolute and relative measures, and (b) investigate the relationship between gender inequalities in PA and contextual factors, such as geographic region,HDI,GII,and unemployment rates.
2.Methods
2.1. Study design and sample
This study uses cross-sectional data from the Global School-Based Student Health Survey(GSHS). The GSHS is a collaborative surveillance project between WHO, the U.S.Centers for Disease Control and Prevention, and participant countries. It uses standardized methods across multiple countries to monitor risk and protective factors in students.
In the GSHS, a 2-stage sampling design is applied to identify participants by stratum and school. First, schools are selected by cluster sampling,and,in the selected schools,classes that students aged 13-17 years attend are randomly chosen. All the students in the chosen classrooms are invited to participate in the study regardless of age(a small proportion of students could be outside of the target age range in some countries) by answering the self-administered questionnaire. The sample is representative of students aged 13-17 years in each country.
Ethical approval for the GSHS was obtained from both a national government(the Ministry of Health or Education)and an institutional review board or ethics committee in each country. In all cases, a consent form is obtained from the students and/or parents, depending on the national laws and practices,and from the schools.More detailed information about the survey is available elsewhere.25,26
2.2. Inclusion criteria
This study used publicly available data from the WHO website. Surveys linked to the GSHS conducted in Global South countries between 2010 and 2020 were included. All GSHS surveys conducted before 2013 included adolescents aged 13 to 15 years, while surveys conducted from 2013 onwards included adolescents aged 16-17 years as well. In countries where multiple surveys were available,only information from the most recent survey was included.
2.3. Country context variables
For each country with PA data available,information available on contextual variables were retrieved from secondary sources (i.e., World Bank and the Human Development Reports from the United Nations).27,28The following countrycontext variables extracted from secondary sources and correspondent to the same year of each survey were included:country income, gross domestic product (GDP), unemployment rate,WHO regions,HDI,and GII.
Data about country income, GDP, and unemployment rate were extracted from the World Bank.27Countries were classified by income level into low, lower-middle, upper-middle,and high-income countries based on gross national income(GNI) per capita from the previous year calculated in current US dollars(using the Atlas method exchange rates).GDP represents the total monetary or market value of all the final goods and services produced within a country’s borders during a specific period. The unemployment rate represents the number of unemployed working-age people as a percentage of the labor force (total number of unemployed people plus those in employment), seasonally adjusted. The WHO regions,retrieved from the WHO (https://www.who.int/countries),were defined as African Region, Eastern Mediterranean Region, Region for the Americas, South-East Asia Region,and Western Pacific Region.
Data about HDI and GII were extracted from the Human Development Reports.28The HDI is a summary measure of average achievement in key dimensions of human development, i.e., a long and healthy life, being knowledgeable, and having a decent standard of living. The GII measures gender inequalities in reproductive health(measured by maternal mortality ratio and adolescent birth rates), empowerment (measured by proportion of parliamentary seats occupied by females and proportion of adult females and males aged 25 years and older with at least some secondary education),and economic status (expressed as labor market participation and measured by labor force participation rate of female and male populations aged 15 years and older).The higher the GII value,the more disparities between females and males and the more loss to human development.
2.4. PA
In each survey, total PA was assessed using the following self-administered question: “During the past 7 days, on how many days were you physically active for a total of at least 60 minutes per day?” Adolescents who answered the option “7 days”were considered sufficiently physically active.
2.5. Statistical analyses
First, we described the national prevalence of PA across the countries.To evaluate inequality at the individual level,we considered gender (boys or girls) as the stratifying variable based on the self-reported question “What is your sex?” from the GSHS survey,25with the following response options:(a)male or(b)female.Differences in the prevalence of PA by gender were presented for each country using equiplot graphs,which provide visual representation of absolute inequalities(https://equidade.org/equiplot).
Absolute and relative inequalities in PA were calculated for each country using standardized methods.23,24Absolute inequalities(gender differences)were calculated by subtracting PA prevalence among girls from PA prevalence among boys in order to obtain an absolute gap between boys and girls in p.p. Negative values indicate higher prevalence among girls, while positive values indicate higher prevalence among boys,and zero indicates equality. We estimated the 95% confidence intervals (95%CIs)for these differences using the bootstrap method, which provides the standard errors of the differences based on resampling strategy. Relative inequalities were obtained through Poisson regression using the prevalence in girls as the reference category.Values above 1 indicate higher prevalence among boys, values lower than 1 indicate higher prevalence among girls, and 1 indicates equality. These 2 indicators could provide different information about gender inequalities in PA, depending on the prevalence of PA in each country.
Meta-analyses with random effects were used to calculate the global pooled estimates of absolute and relative inequalities according to country income level and WHO regions.Heterogeneity was estimated using the I2test.29Additionally,we presented smooth curves from polynomial regression for gender ratio according to GDP, HDI, GII, and unemployment rate. All analyses were conducted in Stata (Version 16;StataCorp.,College Station,TX,USA)using expansion factors or sample weights,including the svy command.
3. Results
This study includes data from 64 Global South countries.Sample size varied from 500 in Nauru to 27,189 in Argentina,with percentage of girls ranging from 26.8% in Benin to 56.6%in Nauru and overall response rates ranging from 57% in Vanuatu to 97%in Syrian Arab Republic(Table 1).The national prevalence of PA in adolescents varied widely across the countries (Fig. 1). The lowest prevalence of PA was found in the Philippines(total:7.4%,boys:7.9%,girls:6.9%)and the highest in Bangladesh(total:41.4%,boys:41.7%,girls:40.6%).

Table 1(Continued)
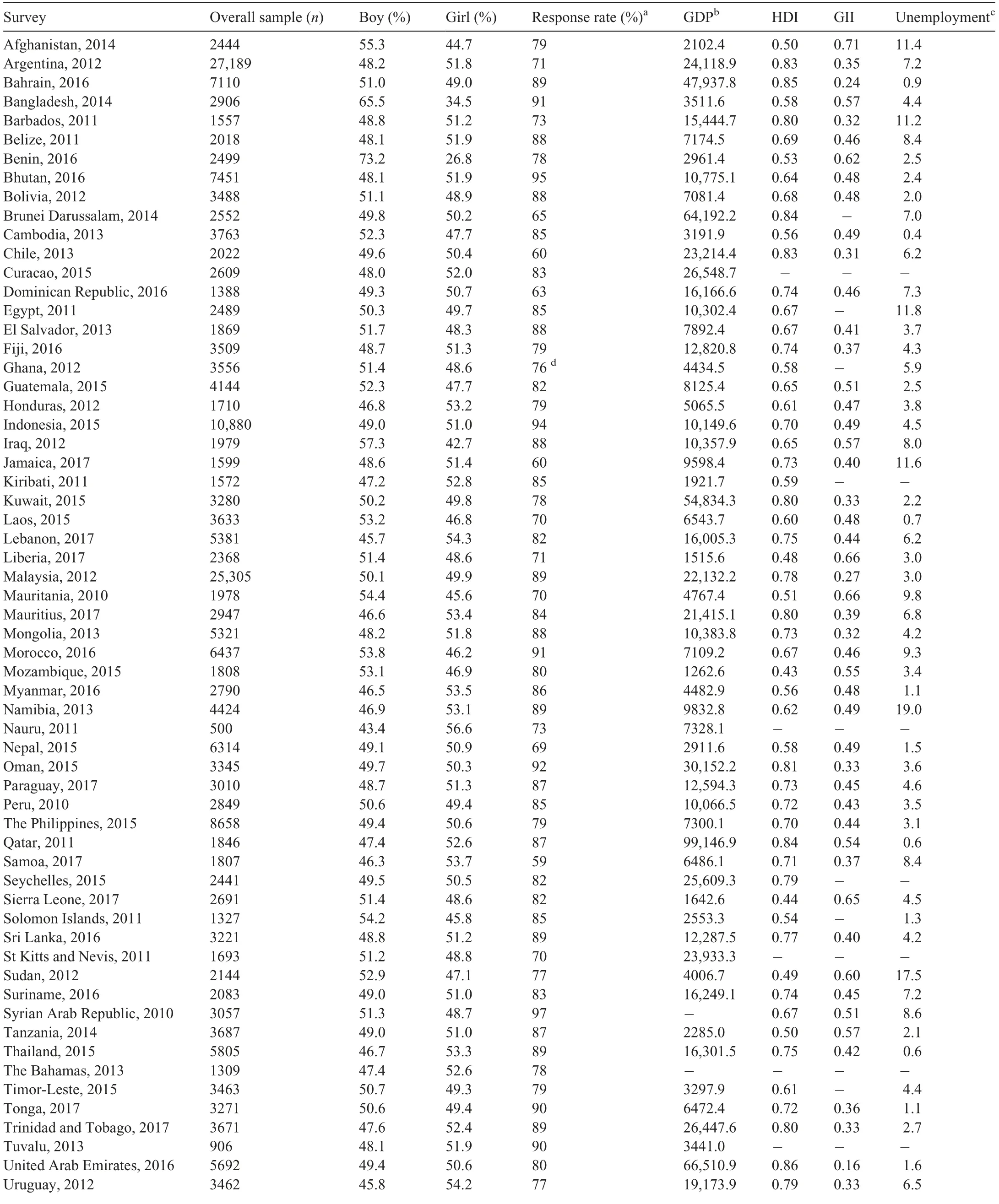
Table 1 Sample characteristics of adolescents included in the Global School-Based Student Health Survey in 64 Global South countries.
Fig. 2 shows the prevalence of PA for boys and girls. The countries with the highest absolute gender gap were Laos,Uruguay, and Brunei, with boys presenting PA prevalences more than 14 p.p.higher than girls.In 13 countries(20.3%)the absolute difference in PA prevalence between boys and girls was lower than 3 p.p. (Vanuatu, Afghanistan, the Philippines,Sudan, Bangladesh, Tonga, Indonesia, Ghana, Namibia,Jamaica, Bhutan, Peru, and Tuvalu). Eighteen countries(28.1%)had a difference between PA prevalence for boys and girls ranging from 3 p.p. to <6 p.p., and in 20 countries(31.3%) it ranged from 6 p.p. to <9 p.p. Absolute differences in PA between boys and girls higher than 10 p.p. were observed in 13 countries (Paraguay, Mozambique, Lebanon,Iraq, Barbados, Egypt, Malaysia, Thailand, Bahrain, Mauritius,Brunei,Uruguay,and Laos).
Fig.3 shows the absolute gender inequality for PA according to country income group. Overall, the prevalence of PA was 6.61 p.p.higher in boys than in girls,with large heterogeneity between countries(I2=85.1%).The highest absolute gap was observed in high-income countries, with a pooled difference of 8.98 p.p. between the boys’ and girls’ PA (95%CI:7.24-10.72). In low-income countries, boys presented a PA prevalence 5.31 p.p.higher than girls(95%CI:2.96-7.66).
Fig. 4 shows the relative gender inequality for PA. The pooled ratio for all countries showed that boys presented a PA prevalence 1.58 times higher than girls (95%CI: 1.47-1.70)on average. The relative inequality was similar across the income groups but was highest in the high-income countries(1.82, 95%CI: 1.62-2.05). Regarding heterogenity, lowincome countries presented the lowest(I2=50.0%)and uppermiddle-income countries, the highest (I2=92.9%). Absolute and relative gender inequality were very similar across WHO regions(Supplementary Figs.1 and 2).
The relationship between absolute gender inequality for PA and country-level variables is presented in Fig. 5. Countries with higher HDI rankings also presented higher gender differences in PA behavior, with an almost linear relationship. In general, countries with higher GDP presented the highest inequalities. Countries with a higher GII presented a lower gender inequality for PA.No pattern was found for unemployment rates. Supplementary Fig. 3 shows the same analysis for relative inequality according to the same indicators, and the patterns were very similar to Fig.5.
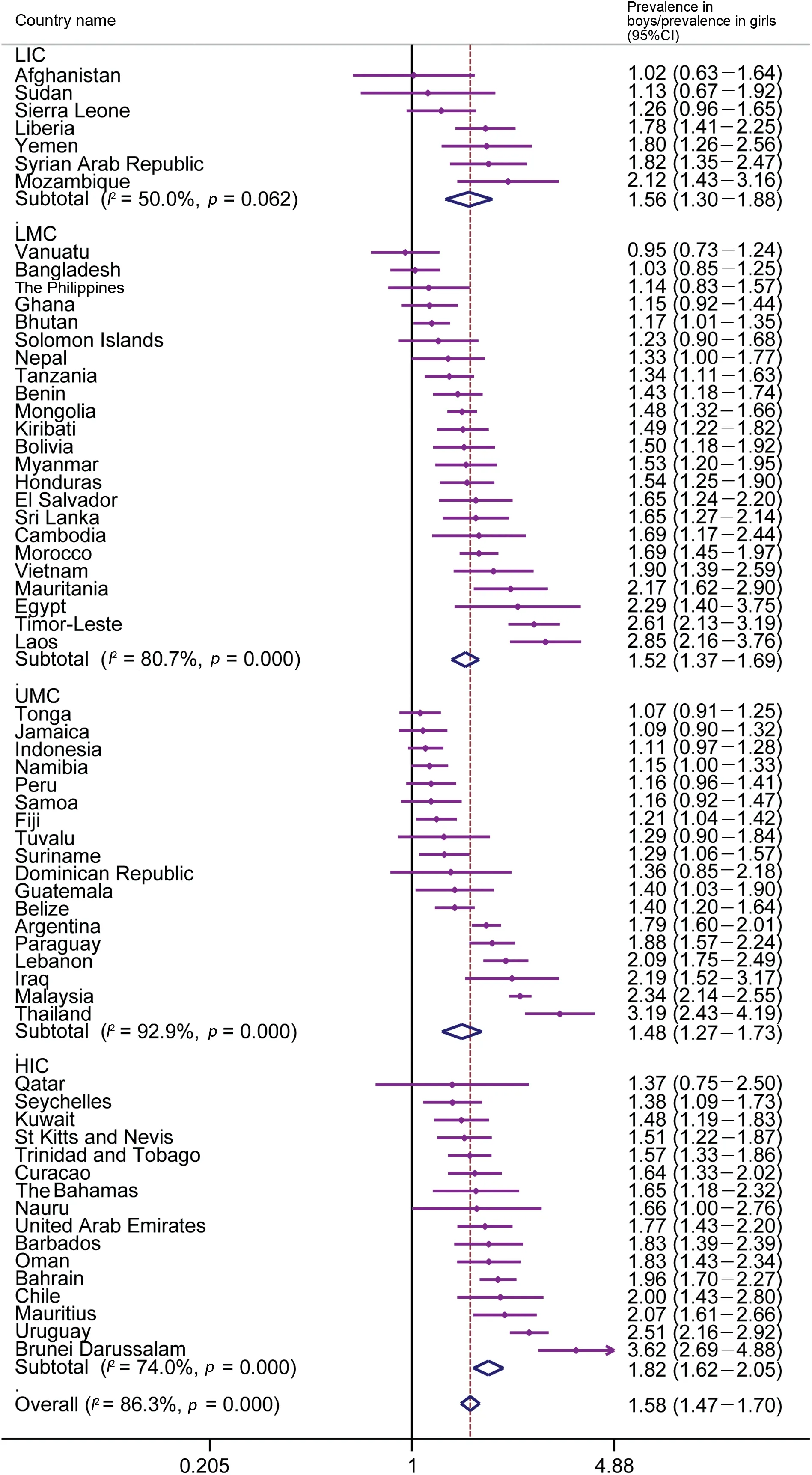
Fig. 4. Relative inequality in physical activity prevalence between boys and girls by country income groups. 95%CI=95% confidence interval; HIC=highincome countries;LIC=low-income countries;LMC=lower-middle-income countries;UMC=upper-middle-income countries.
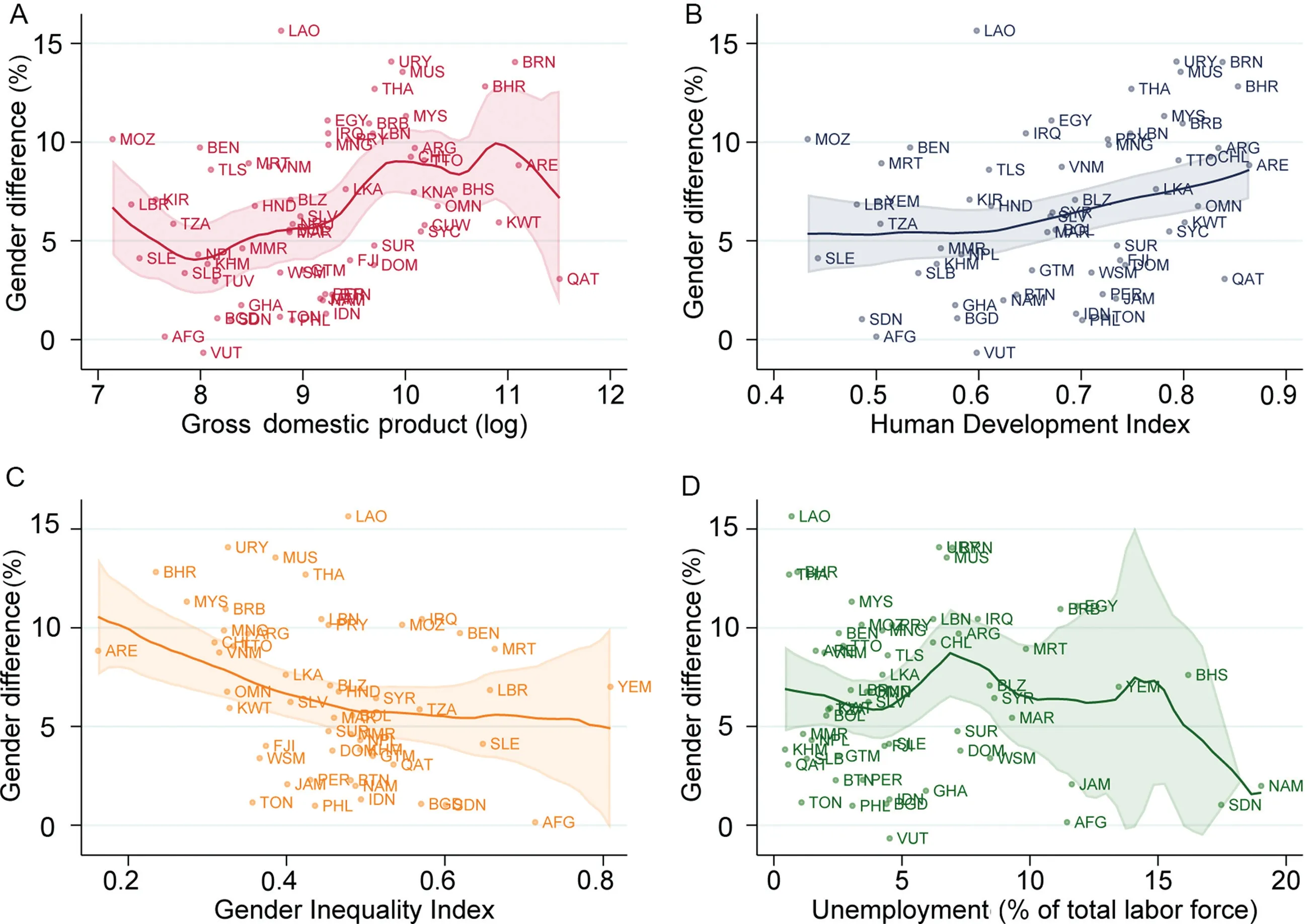
Fig.5. Relationships between absolute gender difference in physical activity with gross domestic product,Human Development Index,Gender Inequality Index,and unemployment percentage.
4. Discussion
Our results show that prevalence of PA in girls is lower than in boys in the large majority of the 64 countries from the Global South included in this study.In 47 of them,there is no overlap in the 95%CI. In addition, some contextual factors of the countries,such as GDP,HDI,and GII,are associated with the gender difference,although not always in the direction one would expect.
The lower prevalence of PA in girls has been reported previously.2,13,30-32Our results are in accordance with recent analysis based on the GSHS, addressing another set of countries, which shows a higher prevalence of insufficient PA in girls.11Several arguments could be made to explain these differences between girls and boys, based on the intrinsic sociocultural norms and barriers that girls face to be involved in PAs(e.g.,stereotypes,insecurity about body image,or cultural acceptability)or simply the gender-specific lack of opportunities to participate in PA. As a result, girls may also have less enjoyment from PA practice and less confidence in their sporting abilities, which could persist throughout adolescence.33Based on our results, it is possible to assume that this societal influence on girls’ PA is intrinsic in society and beyond any traditional determinant of PA. Therefore, to close the gender gap in PA,addressing those restrictive societal norms in multiple contexts, increasing the representation of women in sport,and encouraging girls to be active is essential.34
4.1. Measures of inequality
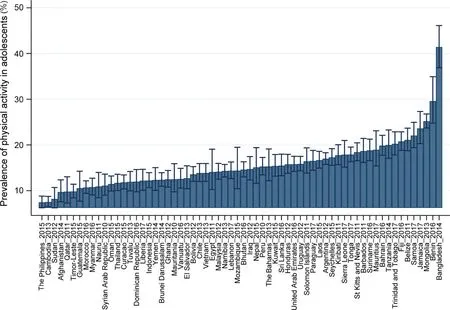
Fig.1. Physical activity prevalence in adolescents for 64 Global South countries.Data are shown as prevalence(%)or 95%confidence interval.
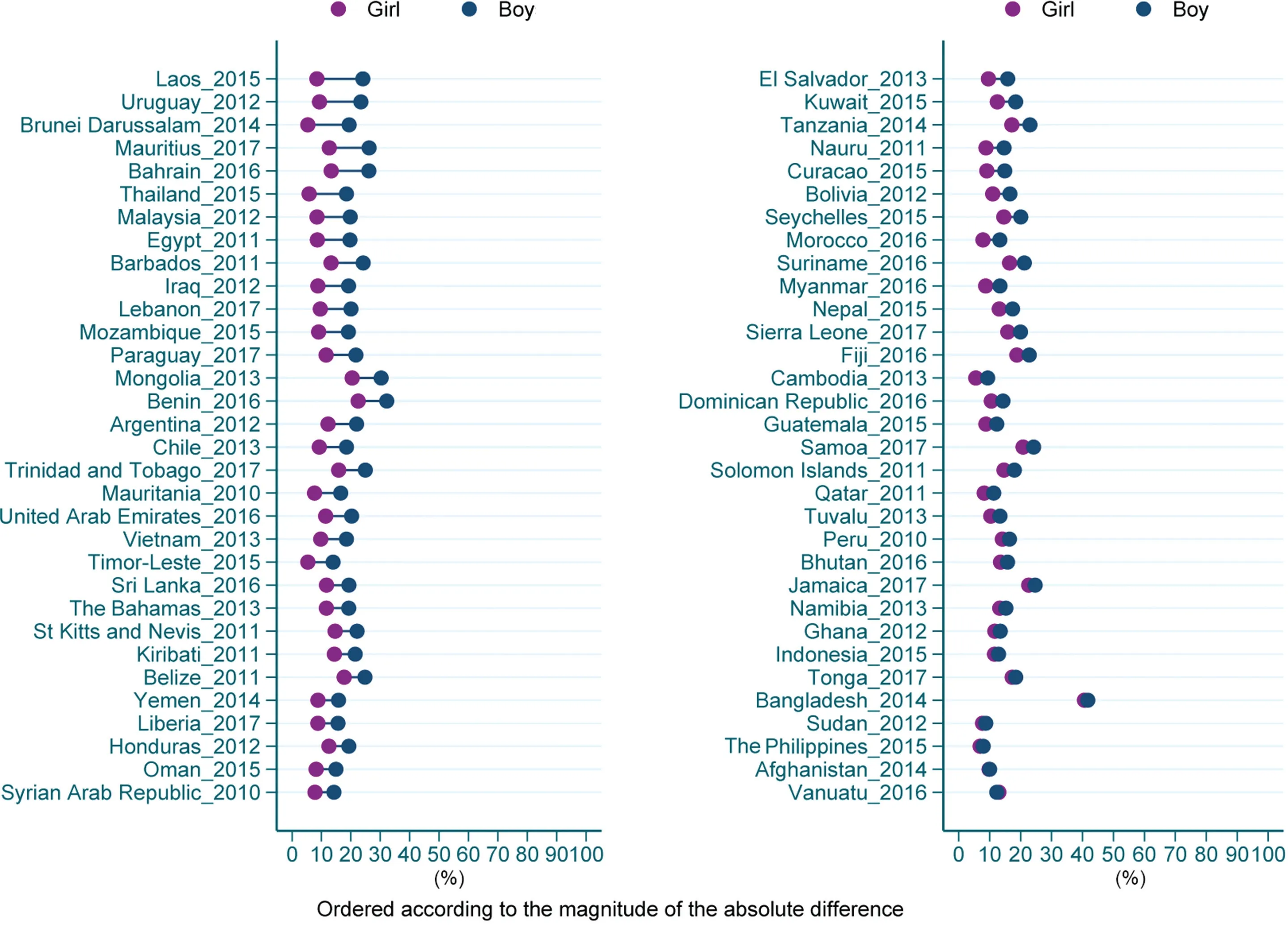
Fig.2. Prevalence of physical activity in adolescents according to gender.
In this study we presented 2 inequalities measures,one relative and the other absolute differences. The general patterns did not change according to inequality measure for most countries, but for a few of them, we can see differences according to the measure used.For example,in countries with lower PA prevalence, such as Cambodia, Myanmar, Morocco, Nauru,and Oman, high gender inequality according to absolute measure was not observed (all these countries present differences below 7 p.p.), probably as a consequence of their low overall PA prevalence. Conversely, when looking for relative inequality, we can see that these same countries presented higher inequalities according to the relative measure(for all of them, the PA prevalence is at least 50% higher among boys).In this sense, an advantage of applying the 2 methods is the 2 different messages that result: absolute measure is easier to interpret and very informative for policy makers who seek to identify how much we need to increase PA among girls to reach equality levels; relative measure is also important to show how unfair the inequality observed is.
4.2. The role of country context on PA gender inequalities
In general, our study showed that inequalities were higher according to increasing World Bank income groups. The domains of PA might be the key factor to understanding such a pattern. Leisure-time PA presents a higher contribution for total PA levels in high-income countries compared to their counterparts among adults8and, despite the lack of domainspecific analyses among adolescents in the literature, there is no reason to expect a different pattern.Therefore,considering leisure-time PA is the domain where intentional PA is performed,and transport and work-related PA are domains with a large predominancy of utilitarian PA (most common in lowand middle-income countries),it seems reasonable that a lower magnitude of inequalities is observed in these settings.35It is worth noting that another contextual characteristic not analyzed in our study is the proportion of out-of-school adolescents, which is larger in low-income countries compared to high-income countries.36Therefore, the school-going adolescent population we analyzed might not be representative of true gender inequalities. However, due to the very limited PA-related literature addressing out-of-school adolescents,2it is challenging to estimate how this population group would influence the magnitude of gender inequality. Finally, despite differences in terms of magnitude, it is concerning to observe that even when PA is a matter of choice (e.g., in the case of high-income countries where there are more opportunities),girls are still being left behind,probably because these opportunities are more often attentive to the preferences of boys than girls.
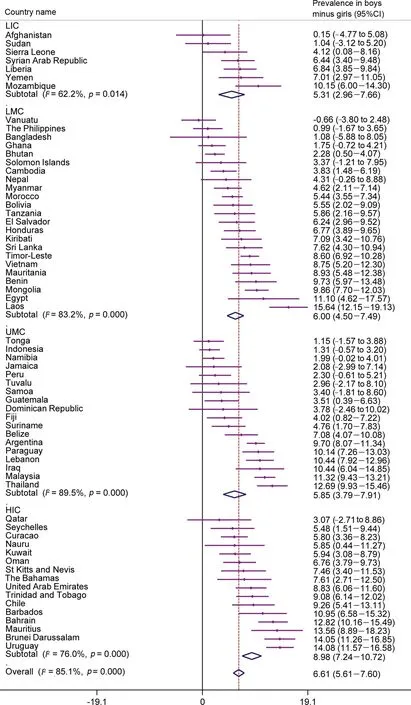
Fig.3. Absolute inequality in physical activity prevalence between boys and girls at country level and pooled by country income groups.95%CI=95%confidence interval;HIC=high-income countries;LIC=low-income countries;LMC=lower-middle-income countries;UMC=upper-middle-income countries.
When analyzing the influence of country-contextual factors on PA gender inequalities, HDI ranking showed the clearest pattern.Where the HDI ranking of the country was higher,the gender gap between boys and girls in PA practice was greater.In summary,the HDI is constructed based on life expectancy,schooling, and income and, therefore, does not reflect inequalities directly.37However, evidence shows that HDI ranking and country income are strongly and positively correlated.38Since PA inequalities are often related to income inequalities,39our findings should be interpreted in a way that considers the set of countries studied. In general, poor countries face more inequalities than rich ones.40,41However, in the present study,all countries included were from the Global South, where even the high-income countries face huge economic disparities.42-44This could help explain the higher gender inequalities found in countries with higher HDI rankings and in high-income countries.
Another interesting discussion regarding the positive association between PA levels and country income groups is related to the Inverse Equity Hypothesis,45,46which states that when there is a new health intervention or innovation,it tends to reach the more privileged groups first, thereby establishing an initial period of increasing inequalities. In the case of PA,the last 30 years were marked by new evidence about the benefits of PA; more efforts are being implemented recently in terms of interventions,particularly in high-income countries.47Considering that the interventions are not necessarily targeted at reducing gender inequality gaps,or even at providing opportunities that speak to girls,it is expected that population groups that are already more physically active would be more positively affected by those interventions.48
Our results showed an inverse association between GII rankings and gender inequalities in PA, which seems like a controversial result.Since the GII addresses several characteristics of the countries, such as health, empowerment, and labor, some components of the index might not translate well for adolescent PA in the Global South.However,a study done on data from the Health Behaviour in School-Aged Children survey, which included 36 countries from both the Global North and South,found the opposite result,with less inequality for adolescent PA in countries in the third tertile of GII.Thus,further research on the topic is needed to support the association between GII and gender PA inequalities.14
Some countries, such as Afghanistan and Bangladesh,present high GII rankings but no gender inequality for PA in the GSHS data; however, this result may not be well supported by other research in the region that suggests more PA engagement among boys than girls. For example, an earlier study showed that 76% of boys and 55% of girls met the MVPA guidelines in Bangladesh.49Varying gender inequality in PA may reflect traditional gender roles in Asian societies,where parents may be more concerned about girls doing activities in outdoor environments for a variety of reasons,including safety and security; as such, girls may be more inclined to engage in less active domestic activities (e.g.,cooking, household chores), while boys are more likely to engage in outdoor activities.Although walking for travel(the lead PA domain) was comparable across gender, girls were more likely than boys to participate in household chores and less likely to engage in soccer,basketball,bicycling,and jogging/running.49Also, girls might experience or perceive PA barriers differently from boys. For example, girls were more likely than boys to perceive an unsafe neighborhood, poor street lighting,and a lack of convenient places nearby as barriers to PA, which are likely to affect girls’ PA engagement in Bangladesh.50
4.3. Reducing PA gender inequalities
When discussing PA promotion, the governmental responsibility of ensuring universal access to public health must be considered. Even though efforts have been made toward implementing PA promotion policies, those initiatives often lack effectiveness.6,51In this sense,the school setting has been well documented as a valuable space for female PA promotion.52,53Evidence also highlights built environment,such as a neighborhood walkability,and living close to sports and recreational facilities as important correlates of girls’ PA.54However, given the massive effect had by the restrictive gender norms faced by women55on a daily basis,comprehensive policies and societal support are essential to increase girls’PA levels.
In terms of opportunities for interventions among adolescents, van Sluijs and colleagues2conducted an umbrella review about evidence-based interventions and suggested 3 key components to be addressed: supportive schools, multiutility urban environments, and the social and digital environment. Despite identifying that poor implementation is an important barrier to the success of school-based interventions,the authors highlighted that multi-component interventions seem to present better results than single-component interventions and that intra-curricular interventions have more success compared to those interventions based on extra-curricular activities only. In addition, the authors emphasize that built environment interventions among adolescents should address a range of activities,including active travel,play,and sports.2Finally, initiatives in this age group should focus on supportive social environments in- and out-of-school, including digital environment opportunities, as well as always consider the natural life contexts that exist during the adolescent transitionary period.
It is essential for policymakers and researchers to improve interventions by considering the context and aiming to target adolescent girls in order to reduce gender inequalities. The abovementioned digital environment opportunities are probably far from a reality in low-income settings, which are predominant in Global-South countries. In terms of equityoriented actions, evidence from a comprehensive review of reviews reinforces the concept that reducing health inequalities must be an intersectional and multidisciplinary effort. Among several strategies proven to be effective at reducing health inequalities,which should be considered when planning future actions, the authors highlighted: provide access to adequate and universal health systems; engage the community in the decision-making processes of interventions and policies;comprehend contextual conditions as social determinants of health;and make efforts to improve those determinants.56These strategies are key when planning interventions aimed at reducing health inequalities, and they could be implemented by Global South governments.
To help Global South countries improve their policies,some examples of countries that managed to promote a gender gap reduction in PA are relevant. Although the general trend for sex differences shows an increase in the gender gap, there are some countries that have reduced it(e.g.,Germany,Lithuania, Scotland, Slovenia, Sweden, and USA).57However, not surprisingly, some of this change is due to a strong reduction in the male prevalence instead of an increase in female PA practice. On the other hand, in Finland girls increased their participation in organized PA between 1977 and 2007. While at the beginning(1977-1979)there was a difference of about 18 p.p.-19 p.p. between the sexes, by 2005, the difference was 10 p.p.and by 2007,it had dropped to 6 p.p.58
4.4. Strengths and limitations
This work presents some limitations that should be discussed. The GSHS surveys used a global definition for PA,assessed by a single self-reported item,without distinguishing the different PA domains. This metric could overestimate PA prevalence due to the inclination to provide socially desirable answers,which could differ according to gender;for example,boys could overreport their PA more often, thereby widening the gap between boys and girls.59Also, this measurement method might present limited validity and reliability when compared to objective measures.60,61It is important to highlight that the GSHS questionnaire25was drawn from the previous WHO recommendations of at least 60 min of MVPA daily,and due to its method of measurement, it is impossible to evalute the compliance with current WHO guidelines(at least 60 min/day of MVPA on average).9
In addition, the GSHS sample includes only school-going adolescents and,therefore,results are not representative of the entire adolescent population of each country, and the results presented may not accurately represent female adolescent population of some countries where girls may be disproportionately attending schools for various reasons. Besides, the inclusion of 16-to 17-year-old adolescents in the GSHS target population since 2012 hampers comparisons between countries. Another important issue is the lack of more comprehensive gender identification/orientation questions in the GSHS,as in most national surveys, which hinders the assessment of gender inequalities beyond the male/female dichotomy.62Finally,results from the pooled estimates should be interpreted with caution considering the high heterogeneity observed by the I2estimates due to the specific differences of each country.
5. Final remarks
Quantifying worldwide gender differences in PA is important because it may increase recognition of the need to address the unethical gender disparities in PA participation across individuals’lifespans.Moreover,studies addressing PA inequalities are now relevant for implementing and monitoring the WHO Global Action Plan on PA 2018-2030. As demonstrated by our findings, PA in adolescents can be influenced by country-context,which may systematically lead to fewer opportunities for girls to be active. These findings reinforce that macro- and micro-level changes should be actively induced if we aim to increase population levels of PA in adolescents and promote equity in PA.Action plans at the local and global levels should target women’s empowerment in society beginning in childhood as an initial step to closing the gender gap in PA.Moreover,policies and interventions that aim to increase PA in girls should focus on local context and improving safety,affordability,and access to PA during leisure time and for transportation, particularly in countries where PA participation is not equally accessible for boys and girls.
Acknowledgments
The work of ICS was supported by the Funda¸c~ao de Amparo a Pesquisa do Rio Grande do Sul—FAPERGS(Number: 10/2020, Grant term: 21/2551-0000670-6), and Brazilian National Research Council(CNPq).
Authors’contributions
LICR conceived the paper outline and drafted the manuscript;AW conceived the paper outline,performed data acquisition and statistical analysis; CdSC conceived the paper outline. All authors helped in writing the manuscript; ICS supervised the work. All authors have read and approved the final version of the manuscript, and agree with the order of presentation of the authors.
Competing interests
The authors declare that they have no competing interests.
Supplementary materials
Supplementary materials associated with this article can be found in the online version at doi:10.1016/j.jshs.2022.01.007.
 Journal of Sport and Health Science2022年4期
Journal of Sport and Health Science2022年4期
- Journal of Sport and Health Science的其它文章
- The Journal of Sport and Health Science:Commemorating a decade of publishing milestones and impact
- Prevalence of meeting 24-Hour Movement Guidelines from pre-school to adolescence:A systematic review and meta-analysis including 387,437 participants and 23 countries
- Which psychosocial factors are associated with return to sport following concussion?A systematic review
- Do people with low back pain walk differently?A systematic review and meta-analysis
- Lymphangiogenesis contributes to exercise-induced physiological cardiac growth
- Influence of biological sex and exercise on murine cardiac metabolism