
椎动脉夹层致蛛网膜下腔出血的危险因素分析
2022-06-12 14:27孙洁连亚军陈媛
中国现代医生 2022年15期
孙洁 连亚军 陈媛


[摘要] 目的 探討椎动脉夹层致蛛网膜下腔出血(SAH)的危险因素。方法 前瞻性收集2011年8月至2019年12月郑州大学第一附属医院诊治的椎动脉夹层患者的临床资料。根据是否发生SAH分为SAH组(n=28)和non-SAH组(n=77),对比分析两组患者的人口学资料、既往史、入院后首次实验室指标等差异。采用多因素logistic回归分析椎动脉夹层患者SAH的相关危险因素。结果 共纳入105例椎动脉夹层患者,其中28例(26.7%)患者发生SAH[23例(82.1%)影像学上表现为夹层动脉瘤]。SAH组首发头痛、总胆固醇水平、中性粒细胞计数、D-二聚体水平均高于non-SAH组,LDL<1.8 mmol/L、尿酸水平均低于non-SAH组,差异有统计学意义(P<0.05)。多因素logistic回归分析显示,中性粒细胞计数高和低尿酸水平是椎动脉夹层患者SAH的危险因素。结论 椎动脉夹层患者影像学上常表现为夹层动脉瘤,多于头痛后出现SAH,中性粒细胞计数高、低尿酸水平是椎动脉夹层SAH的相关危险因素。
[关键词] 椎动脉夹层;临床特征;蛛网膜下腔出血;危险因素
[中图分类号] R743.35 [文献标识码] B [文章编号] 1673-9701(2022)15-0012-04
Analysis on risk factors for subarachnoid hemorrhage in patients with vertebral artery dissection
SUN Jie LIAN Yajun CHEN Yuan
Department of Neurology, the First Affiliated Hospital of Zhengzhou University, Zhengzhou 450052, China
[Abstract] Objective To investigate the risk factors for subarachnoid hemorrhage (SAH) in patients with vertebral artery dissection (VAD). Methods The clinical data of patients with VAD treated at the First Affiliated Hospital of Zhengzhou University from August 2011 to December 2019 were prospectively collected. These patients were divided into the SAH group (n=28) and the non-SAH group (n=77) based on the presence or absence of SAH, and the differences in demographic data, previous medical history, and laboratory indexes at the first examination upon admission were analyzed and compared between the two groups. The risk factors associated with SAH in patients with VAD were analyzed by multivariate logistic regression. Results A total of 105 patients with VAD were included, among whom 28 (26.7%) patients developed SAH and 23 (82.1%) patients showed dissection aneurysm on imaging. The degree of severity of the first symptom-headache, total cholesterol level, neutrophil count, and D-dimer level was higher in the SAH group than that in the non-SAH group, and the levels of low-density lipoprotein (LDL) (<1.8 mmol/L) and uric acid in the SAH group were lower than those in the non-SAH group, with statistically significant differences (P<0.05). Multivariate logistic regression analysis showed that high neutrophil count and low uric acid level were risk factors for SAH in patients with VAD. Conclusion Patients with VAD often show a dissection aneurysm on imaging and mostly develop SAH following headache, and high neutrophil count and low uric acid level are risk factors associated with SAH in patients with VAD.7CEC5C62-5815-494D-9E31-8D6FFC5082D0
[Key words] Vertebral artery dissection; Clinical features; Subarachnoid hemorrhage; Risk factors
头颈动脉夹层(cervicocerebral artery dissection,CAD)是由于内膜撕裂或血管破裂引起的动脉壁直接出血所致,其临床症状表现为头颈部疼痛、缺血性脑卒中、SAH、Horner综合征[1-2]。自发性椎动脉夹层(vertebral artery dissection,VAD)发病率约为1/100 000人/年[3]。与颈内动脉夹层相比,VAD更易出现SAH[4]。早期抗凝或抗血小板治疗对CAD是重要的,可减少中风、死亡和心血管事件的发生率[5],但合并SAH的患者要慎重考虑。因此早期识别VAD致SAH的高危患者是至关重要的,可早期评估预后与指导治疗。本研究探究VAD致SAH的相关危险因素,现报道如下。
1 对象与方法
1.1 研究对象
收集2011年8月至2019年12月郑州大学第一附属医院诊治的VAD患者127例,所有患者均行数字减影血管造影(DSA)和(或)计算机断层扫描血管造影(CTA)、磁共振血管造影(MRA)完成诊断。纳入标准[6]:①影像学上符合CAD的典型征象,如双腔征、内膜瓣、壁内血肿、线样征、夹层动脉瘤等;②动脉夹层部位累及椎动脉;③入院时头部CT或MRI证实SAH。排除标准:①合并脑梗死者;②同时累及前循环夹层者;③临床资料不完整者。最终纳入患者105例。本研究已通过郑州大学第一附属医院医学伦理委员会审批。
1.2 方法
根据首次入院时的影像学表现,将VAD患者分为蛛网膜下腔出血(SAH)组和非蛛网膜下腔出血(non-SAH)组。比较两组患者的临床资料,包括高血压、糖尿病、吸烟/饮酒史、高胆固醇血症、既往头痛史、近期感染和轻度头颈部创伤史等,低密度脂蛋白(LDL)以缺血性脑血管病患者二级预防标准1.8 mmol/L为界,分为LDL<1.80 mmol/L和LDL≥1.80 mmol/L。近期感染史:发病前1个月内发生的感染。低尿酸水平和低肌酐水平定义为低于正常参考范围下限值。
1.3 统计学方法
使用SPSS 26.0统计学软件进行数据分析,符合正态分布的计量资料以均数±标准差(x±s)表示,偏态分布的计量资料以中位数(四分位数间距)[M(P25,P75)]表示,计数资料以[n(%)]表示。计量资料组间比较采用Mann-Whitney U Test检验,计数资料组间比较采用χ2检验或Fisher′s exact检验,将上述P<0.1的变量共同纳入多因素logistic回归分析,P<0.05为差异有统计学意义。
2 结果
2.1 一般资料
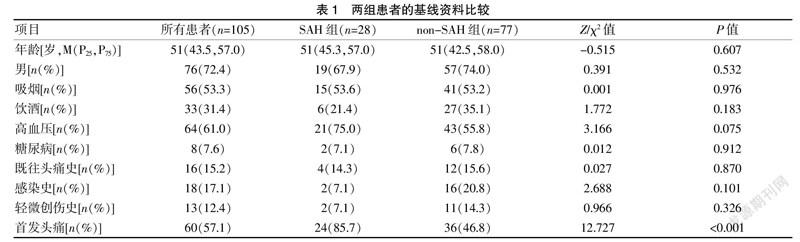
共纳入VAD患者105例,28例(26.7%)患者发生SAH,其中3例(10.7%)涉及双侧椎动脉。SAH组(n=28)男19例,女9例,年龄40~79岁,平均(51.75±1.55)岁;non-SAH组(n=77)男57例,女20例,年龄10~73岁,平均(48.40±1.58)岁。SAH组首发头痛比例高于non-SAH组,差异有统计学意义(χ2=12.727,P<0.001);两组间其他指标比较,差异无统计学意义(P>0.05)。见表1。28例SAH患者影像学特征见表2,其中4例(14.3%)复发,1例(3.6%)死亡。
2.2 两组的实验室指标及影像学比较
单因素分析结果显示,SAH组的总胆固醇水平、D-二聚体水平、中性粒细胞计数均高于non-SAH组,LDL、尿酸水平均低于non-SAH组,差异有统计学意义(P<0.05),两组间其他指标比较,差异无统计学意义(P>0.05)。见表3。
2.3 VAD致SAH的多因素分析
将表1、3中组间比较P<0.1的变量纳入多因素logistic回归分析,结果显示,中性粒细胞计数高和低尿酸水平是椎动脉夹层患者SAH的危险因素。见表4。
3 讨论
一项日本的研究报道脑动脉夹层中SAH多发生于椎动脉夹层[7]。本研究105例VAD患者中,28例(26.7%)合并SAH,其中3例累及双侧椎动脉,均继发SAH。Takahara等[8]发现双侧椎动脉夹层患者易出现缺血性卒中,与本研究相反,可能是由于本研究3例患者影像学上均表现为颅内夹层动脉瘤。
头颈部疼痛是颅内动脉夹层患者的预警症状,随后出现SAH和缺血性卒中[9]。本研究中60例(57.1%)VAD患者以头痛为首发症状,40%随后发生SAH。头颈部疼痛可能由血管壁直接撕裂引起,血管扩张刺激周围感觉神经纤维也可能是疼痛的直接原因[10]。
少数研究表明吸烟、优势侧椎动脉夹层、累及小脑后下动脉、VUBA>45°、珠线征是颅内夹层SAH的高危因素[11-12],但关于椎动脉夹层破裂的研究较少,相关风险因素尚不明确。本研究表明SAH组患者D-二聚体水平、LDL≥1.8 mmol/L、总胆固醇水平较non-SAH组高。D-二聚体水平升高往往表明人体内纤溶活性增强,对SAH预后不良有预测价值[13]。另外,有文献报道血浆D-二聚体水平高与未来脑出血风险增加相关,在抽血距脑出血时间最短的人群中更明显[14]。既往一项研究发现胆固醇水平与颈动脉夹层呈负相关[15]。而一项研究发现血清胆固醇可通过加剧炎症反应促进中膜退行性改变和颅内动脉瘤的进展[16]。本研究提示高胆固醇血症和高脂血症可能促进颅内夹层动脉瘤破裂。因此可推测胆固醇在夹层形成和破裂中的机制可能是不同的。
Forster等[17]发现与创伤性颈动脉夹层患者相比,自发性颈动脉夹层患者白细胞计数和CRP升高,提示炎症在自发性颈动脉夹层中发挥作用。另外,一項前瞻性大型队列研究发现基线期白细胞计数高与SAH发生率增加有关,表明炎症反应可能先于SAH[18]。一项大鼠的颅内动脉瘤破裂模型中,发现中性粒细胞可通过血管滋养血管聚集并加剧动脉瘤破裂部位的炎症反应,产生破坏组织的蛋白酶使动脉壁退行性改变导致颅内动脉瘤破裂[19]。本研究也发现中性粒细胞计数高可能与VAD患者SAH相关。因此推测炎症反应可能是椎动脉夹层动脉瘤破裂机制之一。研究表明,尿酸(UA)是一种重要的内源性抗氧化剂,通过清除自由基、抑制炎症级联反应、降低血脑屏障通透性等机制对神经起保护作用[20-21]。Song等[22]发现尿酸水平降低可增加缺血性卒中出血转化的风险,间接反映尿酸的神经保护作用。最近,Xiao等[23]发现低尿酸水平可通过上调Erk1/2-MMP轴的活性,增强弹性蛋白、胶原降解,从而破坏平滑肌-弹性蛋白收缩单位的完整性导致血管破裂。而且上述血管破裂可以被生理浓度的尿酸水平和p-Erk1/2特异性抑制剂部分抑制。这或许可以解释尿酸水平低的VAD患者SAH的风险较高的原因。本研究中19例患者尿酸水平降低,其中13例发生SAH,可证实既往研究结果。7CEC5C62-5815-494D-9E31-8D6FFC5082D0
綜上所述,VAD患者多以头痛为首发症状,当中性粒细胞计数高及尿酸水平降低时要警惕SAH的风险,及时给予介入干预。
[参考文献]
[1] Ortiz J,Ruland S. Cervicocerebral artery dissection[J].J Stroke Cerebrovasc Dis,2015,30(6):603-610.
[2] Wang Y,Cheng W,Lian Y,et al. Characteristics and relative factors of headache caused by cervicocerebral artery dissection[J].J Neurol,2019,266(2):298-305.
[3] Bonacina S,Locatelli M,Mazzoleni V,et al. Spontaneous cervical artery dissection and fibromuscular dysplasia: Epidemiologic and biologic evidence of a mutual relationship[J].Trends Cardiovasc Med,2021,32(2):103-109.
[4] von Babo M,De Marchis GM,Sarikaya H,et al. Differences and similarities between spontaneous dissections of the internal carotid artery and the vertebral artery[J].Stroke,2013,44(6):1537-1542.
[5] Rosati LM,Vezzetti A,Redd KT,et al. Early anticoagulation or antiplatelet therapy is critical in craniocervical artery dissection: Results from the COMPASS registry[J].Cerebrovasc Dis,2020,49:369-374.
[6] Hakimi R,Sivakumar S. Imaging of carotid dissection[J].Current Pain and Headache Reports,2019,23(1):2.
[7] Mori S,Takahashi S,Hayakawa A,et al. Fatal intracranial aneurysms and dissections causing subarachnoid hemorrhage: An epidemiological and pathological analysis of 607 legal autopsy cases[J].J Stroke Cerebrovasc Dis,2018, 27(2):486-493.
[8] Takahara M,Ogata T,Abe H,et al. The comparison of clinical findings and treatment between unilateral and bilateral vertebral artery dissection[J].J Stroke Cerebrovasc Dis,2019,28(5):1192-1199.
[9] Bond KM,Krings T,Lanzino G,et al. Intracranial dissections: A pictorial review of pathophysiology,imaging features,and natural history[J].J Neuroradiol,2021,48(3):176-188.
[10] Sheikh HU. Headache in intracranial and cervical artery dissections[J].Current Pain and Headache Reports,2016, 20(2):8.
[11] Matsukawa H,Fujii M,Shinoda M,et al. Comparison of clinical characteristics and MR angiography appearance in patients with spontaneous intradural vertebral artery dissection with or without subarachnoid hemorrhage[J].J Neurosurg,2011,115(1):108.
[12] Matsukawa H,Shinoda M,Fujii M,et al. Differences in vertebrobasilar artery morphology between spontaneous intradural vertebral artery dissections with and without subarachnoid hemorrhage[J].Cerebrovasc Dis,2012,34(5-6):393-399.7CEC5C62-5815-494D-9E31-8D6FFC5082D0
[13] Fukuda H,Lo B,Yamamoto Y,et al. Plasma D-dimer may predict poor functional outcomes through systemic complications after aneurysmal subarachnoid hemorrhage[J].J Neurosurg,2017,127(2):284-290.
[14] Johansson K,Jansson J,Johansson L,et al. D-dimer is associated with first-ever intracerebral hemorrhage[J].Stroke,2018,49(9):2034-2039.
[15] Debette S,Metso T,Pezzini A,et al. Association of vascular risk factors with cervical artery dissection and ischemic stroke in young adults[J].Circulation,2011,123(14):1537-1544.
[16] Shimizu K,Miyata H,Abekura Y,et al. High-fat diet intake promotes the enlargement and degenerative changes in the media of intracranial aneurysms in rats[J].J Neuropathol Exp Neurol,2019,78(9):798-807.
[17] Forster K,Poppert H,Conrad B,et al. Elevated inflammatory laboratory parameters in spontaneous cervical artery dissection as compared to traumatic dissection[J].J Neurol,2006,253(6):741-745.
[18] Soderholm M,Zia E,Hedblad B,et al. Leukocyte count and incidence of subarachnoid haemorrhage: A prospective cohort study[J].BMC Neurol,2014,14:71.
[19] Kushamae M,Miyata H,Shirai M,et al. Involvement of neutrophils in machineries underlying the rupture of intracranial aneurysms in rats[J].Sci Rep,2020,10(1):151.
[20] Lucca G,Comim CM,Valvassori SS,et al. Increased oxidative stress in submitochondrial particles into the brain of rats submitted to the chronic mild stress paradigm[J].J Psychiatr Res,2009,43(9):864-869.
[21] Romanos E,Planas A M,Amaro S,et al. Uric acid reduces brain damage and improves the benefits of rt-PA in a rat model of thromboembolic stroke[J].J Cereb Blood Flow Metab,2007,27(1):14-20.
[22] Song Q,Wang Y,Cheng Y,et al. Serum uric acid and risk of hemorrhagic transformation in patients with acute ischemic stroke[J].J Mol Neurosci,2020,70(1):94-101.
[23] Xiao N,Liu T,Li H,et al. Low serum uric acid levels promote hypertensive intracerebral hemorrhage by disrupting the smooth muscle cell-elastin contractile unit and upregulating the Erk1/2-MMP axis[J].Transl Stroke Res,2020,11(5):1077-1094.
(收稿日期:2021-11-01)7CEC5C62-5815-494D-9E31-8D6FFC5082D0
猜你喜欢
上海医药(2016年23期)2016-12-22
华夏医学(2016年4期)2016-12-12
华夏医学(2016年4期)2016-12-12
中国实用医药(2016年28期)2016-12-07
科教导刊·电子版(2016年26期)2016-11-21
科技资讯(2016年19期)2016-11-15
中国实用医药(2016年24期)2016-10-17
中国实用医药(2016年22期)2016-08-19
中国实用医药(2016年20期)2016-08-11
