
Comparison of the performance of MS enteroscope series and Japanese double- and single-balloon enteroscopes
2022-06-11 07:39:50JinHuaLiuDanYangLiuYongFengYuanXueJunSunShuMeiShan
World Journal of Gastroenterology 2022年13期
Jin-Hua Liu, Dan-Yang Liu, Yong-Feng Yuan, Xue-Jun Sun, Shu-Mei Shan
Abstract
Key Words: Intestinal ascariasis; Intestinal variation; Crohn's disease; Serum gastrin; Small intestine endoscope
INTRODUCTION
The small intestine is the longest organ in the digestive system, and the average length varies among different species[1 -3 ]. Thus, the precise treatment of small intestine disorders remains a challenge for clinicians[4 -6 ]. In 2003 , Yamamoto et al[7 ] from Jichi Medical University (Tokyo, Japan), together with Fuji Photo Optical Co., Ltd., developed a double-balloon endoscope and applied it in clinical practice[8 ,9 ]. The double-balloon small intestine endoscope was developed by Yamamoto et al[10 -12 ] in Japan.During double-balloon small intestine endoscopy, an over tube with a balloon on top is added to the original push-type endoscope, along with the addition of a balloon at the top of the master camera.Small intestine endoscopy can be completed by alternately pushing-pulling the balloons at the overtube and the master camera. The single-balloon small intestine endoscope is a small bowel endoscope designed by Olympus, Japan, in an attempt to avoid patent infringement[13 ]. The hook-pull action of the front-end of its master camera replaces the master camera of the double-balloon small intestine endoscope.
In 2005 , we also initiated research and development on the MS series of small intestine endoscopes.The past ten years have witnessed the evolution of five generations of our small intestine endoscope.The MS-1 small intestine endoscope is a negative-pressure device that is advanced into the small intestine in a paralleled alternating manner, and has a long detection time. Based on the design of the MS-1 small intestine endoscope, the MS-2 small intestine endoscope was designed with two delivery devices, along with fixing rings and a metal slide. The MS-3 small intestine endoscope abandoned the fixing rings and metal slide and fixed the power and transmission parts together. The MS-4 small intestine endoscopeused a different fixation method to avoid the risk of bowel perforation under extreme working conditions. This new type of small intestine endoscopehad increased stability and speed during the examination, with fewer slippage events. The detection time was not significantly different between the MS-4 small intestine endoscope and MS-3 small intestine endoscope. The design of our latest MS-5 small intestine endoscope has been finalized, and its development is in progress.
The Japanese double-balloon small intestine endoscope has gradually been accepted by patients with the development of painless anesthesia. In this study, we aimed to analyze the detection time of the MS series of small intestine endoscopes and the detection time of the single-balloon small intestine endoscope (SBE) and double-balloon small intestine endoscope (DBE), investigated the possible reasons for the prolonged detection time of small intestine endoscopy.
MATERIALS AND METHODS
Experimental study
In vivoexperiments were conducted in 20 Living adult pigs weighing 100 ± 20 kg. The animals were fed with water for two days and fasted for four hours before each experiment. Bowel preparation was routinely performed and each type of MS small intestine endoscope was checked before the experiment.Intravenous anesthesia with propofol and ketamine was applied. Following intravenous anesthesia,oxygen was provided to the pigviaa nasal catheter at 3 L/min, and the vital signs were continuously monitored. The MS series of small intestine endoscopes was performed by a single endoscopist. When the auxiliary power tube was lubricated with paraffin oil, the camera was inserted into the main auxiliary power tube. Whether the endoscope could slide smoothly through the power tube was examined. After entering the upper part of the small intestine at 20 cm, the auxiliary power system was opened, the MS-1 small intestine endoscope used a double drive power pipe, the auxiliary power catheters were worked alternately; MS-2 to MS-4 small intestine endoscopes used four drive power pipes, MS-1 to MS-3 small intestine endoscopes worked with negative pressure power and MS-4 small intestine endoscope worked with positive pressure power, the auxiliary power catheters of group 1 and group 3 were pushed 40 -50 cm to the distal end, group 1 and group 3 were given power catheter pressure or balloon dilatation, then the power catheters of groups 1 and 3 were pulled back to the starting position of groups 2 and 4 . When the auxiliary power catheters of groups 2 and 4 were pushed 40 -50 cm to the distal end, the auxiliary power catheters of groups 2 and 4 were injected with pressure,and then the power catheters of groups 2 and 4 were pulled back to the proximal end of groups 1 and 3 .At the same time, the catheter was pulled back to the back of the catheter in groups 1 and 3 , and then the catheter in groups 1 and 3 was pushed forward again. When the tube was folded or if the camera was difficult to insert, the extension distance of the power arm and the operating frequency were adjusted according to the insertion depth. The condition of the small intestine was observed and the detection times of MS-2 to MS-4 small intestine endoscopes were recorded. The changes in intestinal tissue using the MS series of small intestine endoscopes were observed and compared before and after the MS series of small intestine endoscopes. Venous blood (3 -5 mL) from the pigs was collected before and after the experiment, and the changes in intestinal tissue after the MS series of small intestine endoscopes were observed after the examination. The MS series of small intestine endoscopes was assisted by a nurse during camera insertion. Using the auxiliary power system, the endoscopist repeatedly pushed the power device to continuously push into the small intestine to the distal end of the camera, thus completing the examination of the entire small intestine. After the examination, venous blood was collected again when anesthesia had worn off. After the completion of each type of small intestine endoscopy experiment, the pigs were allowed to rest, the time to return to normal diet and the time to return to normal stool were recorded, and the next type of small intestine endoscope experiment was performed after 15 days of normal feeding. After the experiment, the live pigs returned to their normal living state.
Clinical data
The detection times of the MS series of small intestine endoscopes were measured. Data on the detection times of SBE and DBE in the following four hospitals were analyzed: (1 ) Guangdong Provincial People's Hospital: 40 patients including 26 males and 14 females underwent Japanese DBE; (2 ) Shengjing Hospital Affiliated to China Medical University: From January 2009 to November 2013 , DBE (Fujino EN-450 P5 Double-Balloon small intestine endoscope, Japan) was performed in 78 patients (including 41 males and 37 females). No definite lesions were found before the procedure; (3 ) Affiliated Hospital of Zunyi Medical College: Small intestine endoscopy (SIF-Q260 type, Olympus, Japan) was performed in 17 patients with clinically suspected small bowel diseases from January to October 2010 ; (4 ) Zhongshan Hospital Affiliated to Fudan University: SBE (SIF-Q260 , Olympus, Japan) was performed in 148 patients with suspected small bowel diseases from June 2009 to March 2011 .
Observational indicators
To observe the effect of the MS series of small intestine endoscopes on gastrointestinal tract, the changes in serum gastrin levels and intestinal tissue were observed and compared before and after the MS series of small intestine endoscopes examination. The time required for the examination was recorded.
Statistical analysis
Statistical analysis was performed using the SPSS software package 21 .0 . The measurement data are expressed as mean ± standard deviation (X± SD).
RESULTS
The experiment duration was 3 mo. One case of Ascarislumbricoides (Figure 1 ), one of suspected Crohn's disease (Figure 2 ), one small intestinal diverticulum (Figure 3 ) and one anesthesia accident were observed in pigs.
The serum gastrin level was 22 .36 ± 2 .88 pg/mL before the MS-1 small intestine endoscope examination, and was 22 .33 ± 2 .98 pg/mL after the examination. There was no difference in theselevels before and after the MS-1 small intestine endoscope experiment (P > 0 .05 ), and there were no abnormalities in the intestinal tract. The time required for inspection was 2 .30 ± 0 .15 h. After completion of the MS-1 small intestine endoscope experiment, the pigs returned to their normal diet after 4 h and defecation returned to normal after one day.
The serum gastrin value was 21 .88 ± 3 .18 pg/mL before the MS-2 small intestine endoscope examination, and was 22 .08 ± 2 .96 pg/mL after the examination. There was no difference in these levels before and after the MS-2 small intestine endoscope experiment (P > 0 .05 ), and there were no abnormalities in the intestinal tract. The time required for inspection was 1 .50 ± 0 .30 h. After completion of the MS-2 small intestine endoscope experiment, the pigs returned to their normal diet after 4 h and defecation returned to normal after one day.
The serum gastrin value was 22 .28 ± 3 .06 pg/mL before the MS-3 small intestine endoscope examination, and was 21 .78 ± 3 .76 pg/mL after the examination. There was no difference between these levels before and after the MS-3 small intestine endoscope experiment (P > 0 .05 ).Ascarislumbricoideswas found in one case, small intestinal diverticulum was found in one case and suspected Crohn's disease was found in one case. The time required for inspection was 0 .67 ± 0 .33 h. After completion of the MS-3 small intestine endoscope experiment, the pigs returned to their normal diet within 3 h and defecation returned to normal within one day. The pig withAscarislumbricoidesinfection was isolated and treated with albendazole and ivermectin for one week. Small intestinal diverticulum and suspected Crohn's disease were not treated.
Serum gastrin level was 22 .30 ± 3 .08 pg/mL before the MS-4 small intestine endoscope examination,and was 21 .66 ± 3 .93 pg/mL after the examination. There was no difference in these levels before and after the MS-4 small intestine endoscope experiment (P > 0 .05 ). The small intestinal diverticulum and the suspected Crohn's disease were as before. The time required for inspection was 1 .00 ± 0 .13 h. One experimental pig had an anesthesia accident due to excessive ketamine application in the later stage of the MS-4 small intestine endoscope experiment, and the other 19 pigs returned to their normal diet 3 h after the MS-4 small intestine endoscope experiment, and defecation returned to normal after 0 .5 days.NoAscarislumbricoideswas detected in the MS-4 small intestine endoscope group. All 20 experimental pigs completed the relevant experiments, including one case which developed cardiac arrest due to excessive infusion of anesthetics, and in the other 19 cases no abnormalities were found (Table 1 ).
There were no differences in serum gastrin between the groups (P> 0 .05 ).
A total of 283 small intestine endoscopic procedures (including 165 SBE sessions and 118 DBE sessions) were performed in the four hospitals. The detection time was 1 .36 ± 0 .07 h for SBE and 2 .01 ±0 .25 h for DBE, and the overall detection time for the Japanese small intestine endoscopes was approximately 1 .68 ± 0 .16 h.
In Guangdong Provincial People's Hospital, the average detection time for DBE in 40 patients was 147 ± 28 .5 min. In Shengjing Hospital Affiliated to China Medical University, 78 patients successfully completed DBE, and the average examination time was 91 .54 ± 22 .59 min. In the Affiliated Hospital of Zunyi Medical College, the duration of SBE ranged from 30 to 80 min (mean: 45 min) in 17 patients,among whom one patient had an accidental bowel perforation, which improved after surgical repair. In Zhongshan Hospital Affiliated to Fudan University, 148 patients underwent 166 sessions of SBE, with an average duration of 83 .4 min (range: 11 –180 min). The detection time was 1 .36 ± 0 .07 h for SBE and 2 .01 ± 0 .25 h for DBE, and the overall detection time of the Japanese small intestine endoscopes was approximately 1 .68 ± 0 .16 h (Table 2 ).
DISCUSSION
The small intestine includes the duodenum, jejunum and ileum, and each part has no clear boundary[14 ]. Microscopic observations can only be preliminarily judged by color, mucosal annular folds, small intestinal villus density, intestinal wall lymphatic follicles and so on[15 ].The main physiological function of the small intestine is digestion and absorption[16 ]. In addition to continuous digestion by gastric juice, pancreatic juice and bile in the small intestine, the mucosal glands of the small intestine canalso secrete a variety of gastrointestinal hormones, including gastrin, trypsin and cholecystokinin.Hormones are chemical substances produced by endocrine cells and are highly efficient in transmitting information[17 -20 ]. There are many types of hormones and their levels are extremely small (mostly in the range of nanograms and even picograms)[21 ]. They are neither the energy source of the body nor structural substances in the human body. However, they play essential roles in coordinating physiological processes such as metabolism and growth/development by transmitting information.Research on the changes of gastrin before and after the MS series of small intestine endoscopes examination can provide theoretical support for the safe application of small intestine endoscopes.
Analysis of the changes in gastrin may help determine the impact of small intestine endoscopes on the internal environment of the digestive system, thus research and development of small intestine endoscopes are important.

Table 1 Detection time and serum gastrin level of MS series of small intestine endoscopes

Table 2 Detection time of the Japanese small intestine endoscopes

Figure 1 Ascarislumbricoides.

Figure 2 Suspected Crohn's disease.
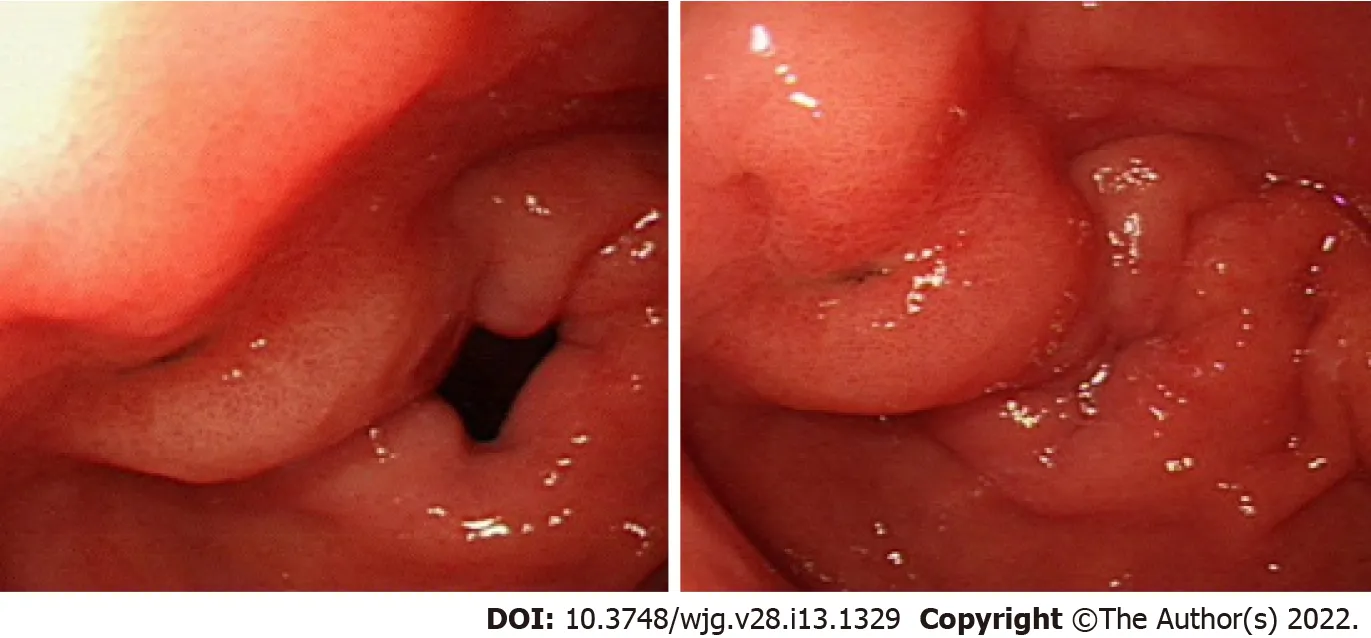
Figure 3 Small intestinal diverticulum.
In the experiments performed in the present study, we found that the MS series of small intestine endoscopes had little effect on the gastrointestinal tract, and the experimental animals soon returned to normal. At the same time, we also found that diseases are often found in living organisms, such asAscarislumbricoides, suspected Crohn's disease and small intestinal diverticulum[22 -24 ].Ascarislumbricoidescan be cured quickly by the combined application of albendazole and ivermectin[25 ].At present, there isno good solution for small intestinal diverticulum and small intestinal tumor[26 ,27 ]. In the future, the precise treatment of lesions may be realized through small intestine endoscopes and laparoscopy.
The incidence rate of gastrointestinal diseases has reached 20 % in China. The incidence rate of small intestinal diseases is approximately 2 .5 % of digestive system diseases. The number of people with small intestinal diseases in China is about 1 .4 billion × 20 % × 2 .5 % ≈ 7 million every year, these people were diagnosed by capsule endoscopy, double balloon small intestine endoscopy and single balloon small intestine endoscopy[28 ,29 ]. Each year, many patients attend tertiary general hospitals for hospital screening layer by layer to choose surgical treatment. However, due to the lack of small intestine endoscope locations, some patients have incomplete resection, intestinal leakage and intestinal obstruction. If these patients have the money to continue treatment, they could attend Nanjing Army General Hospital, which is a laminar flow ward. With regard to small intestinal tumors requiring surgery, although they only account for 5 % of gastrointestinal tumors (the 7thedition of Huang Jiasi's Surgery), they cannot be ignored.
The past ten years have witnessed our efforts in the research and development of the MS series of small intestine endoscopes. From the type MS-1 to MS-5 , the performance of our devices has been constantly improved, and the detection time has been gradually shortened. The MS-1 small intestine endoscope is a negative-pressure device that is advanced into the small intestine in a paralleled alternating manner, and the detection time is long. In 2008 , we adjusted the design to develop the MS-2 small intestine endoscope based on the patented drawings of the pipette small intestine endoscope, and its detection time was slightly shorter when compared with the MS-1 small intestine endoscope.However, slippage of the small intestine endoscope persisted due to the extremely poor stabilities of the fixing rings and the metal slide, making the MS-2 small intestine endoscope unfeasible for clinical applications. In 2010 , we further optimized our design and developed the MS-3 small intestine endoscope based on the patented design of the built-in straw-type small intestine endoscope. This newgeneration device had a shorter detection time than the MS-2 small intestine endoscope. It had higher stability and speed and fewer slippage events during small intestine endoscopy; however, negativepressure perforation occurred in some experiments. Two articles describing the MS-3 small intestine endoscope were published in the Chinese Journal of Digestive Endoscopy and Chinese Journal of Gastrointestinal Surgery, respectively, and our research on this device also won the third prize of the Dalian Science and Technology Progress Award in 2012 .In 2012 , by adopting a new working principle,we developed the MS-4 type based on the patented design of the catheter balloon-type small intestine endoscope. The MS-4 small intestine endoscope has significantly higher stability and speed, along with fewer slippage events[30 ]. The detection time of the MS-4 small intestine endoscope did not decrease compared with the MS-3 small intestine endoscope. Notably, the MS-4 small intestine endoscope has obtained the production license from Liaoning Provincial Food and Drug Administration. In 2018 , we completed the design of the MS-5 small intestine endoscope based on the latest and most practical design. In this new endoscope, we optimized the structure of the auxiliary power system using a fourdrive design. Relevant studies have been carried out since then.
Our team is trying to further optimize the MS series of small intestine endoscopes, particularly to shorten the detection time of small intestine endoscopy. The clinical application of these endoscopes will facilitate the examination, diagnosis, and treatment of gastrointestinal diseases and solve existing problems. To perform new types of surgery, a small intestine endoscope is combined with laparoscopic resection of intestinal lesions. This reduces open surgery, avoids intestinal adhesions or intestinal obstruction caused by open surgery, increases the diagnostic accuracy and cure rate, and thus further improves the capability and quality of medical services.
CONCLUSION
Intestinal ascariasis is a common disease in pigs. Some pigs have abnormal intestinal variations. After continuous upgrade and improvement, the MS-3 and MS-4 small intestine endoscopes appear superior in terms of detection time.
ARTICLE HIGHLIGHTS
ACKNOWLEDGEMENTS
The author would like to thank Dalian Mingsheng Technology Development Co., Ltd. and Harbin Institute of Technology for skillful technical assistance.
FOOTNOTES
Author contributions:Liu JH, Liu DY and Sun XJ designed the research; Liu JH, Liu DY, Yuan YF, Sun XJ and Shan SM performed the research; Liu JH, Liu DY and Sun XJ contributed new reagents/analytic tools; Liu JH analyzed the data; Liu JH and Sun XJ wrote the paper.
Supported bythe 2020 Liaoning Provincial Natural Science Foundation General Project, No. 2020 -MS-332 .
Institutional review board statement:The study was reviewed and approved by the Academic Committee of Dalian Friendship Hospital Institutional Review Board [(Approval No. YY-XS-2019 -001 -1 ]).
Institutional animal care and use committee statement:All procedures involving animals were reviewed and approved by the Institutional Animal Care and Use Committee of the Ethics Committee of Dalian Friendship Hospital (IACUC protocol number: [Protocol No. YY-LL-2020 -015 ]).
Informed consent statement:All study participants, or their legal guardian, provided informed written consent prior to study enrollment.
Conflict-of-interest statement:Xue-Jun Sun has received fees for serving as a speaker for The First Affiliated Hospital of Xi'an Jiaotong University; Jin-Hua Liu has received research funding from Liaoning Provincial Natural Science Foundation; Yong-Feng Yuan is an employee of Harbin Institute of Technology; Shu-Mei Shan owns stocks and/or shares in Dalian Mingsheng Technology Development Company; Jin-Hua Liu and Dan-Yang Liu owns patent Builtin Straw type small intestine endoscope: China, 200920351611 .5 [P]. 2010 -09 -08 ; and Catheter balloon type small intestine endoscope: China, 200920351612 .X [P]. 2010 -09 -08 .
Data sharing statement:Technical appendix, statistical code, and dataset available from the corresponding author at URL. Participants gave informed consent for data sharing.
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4 .0 ) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is noncommercial. See: https://creativecommons.org/Licenses/by-nc/4 .0 /
Country/Territory of origin:China
ORCID number:Jin-Hua Liu 0000 -0002 -5818 -2834 ; Dan-Yang Liu 0000 -0002 -6169 -5390 ; Yong-Feng Yuan 0000 -0002 -2182 -3789 ; Xue-Jun Sun 0000 -0003 -0178 -5551 ; Shu-Mei Shan 0000 -0001 -8568 -3880 .
S-Editor:Wang LL
L-Editor:A
P-Editor:Wang LL
 World Journal of Gastroenterology2022年13期
World Journal of Gastroenterology2022年13期
- World Journal of Gastroenterology的其它文章
- Therapeutic drug monitoring in inflammatory bowel disease: At the right time in the right place
- Endoscopic resection for early gastric cancer: Towards a global understanding
- Generic and disease-specific health-related quality of life in patients with Hirschsprung disease: A systematic review and meta-analysis
- Locoregional therapies and their effects on the tumoral microenvironment of pancreatic ductal adenocarcinoma
- Increased prognostic value of clinical–reproductive model in Chinese female patients with esophageal squamous cell carcinoma
- Management of incidentally discovered appendiceal neuroendocrine tumors after an appendicectomy